

Introduction
Low back pain (LBP) epidemic continues to escalate with a significant economic and societal impact as a major socioeconomic public health concern and the leading burden of disability worldwide.1 According to the latest epidemiological data, globally more than half a billion people are affected by LBP which is forecasted to increase over 800 million by 2050.1 This high prevalence rate has substantial social and economic impact in the United States with direct total costs of US$315 billion for spine conditions with surgical procedures contributing to most of this cost.2 A recent meta-analysis reported LBP was associated with considerable economic cost, high rate of hospitalization and prolonged hospital length of stay in high income countries.3 The aetiology of LBP is multifactorial, and a range of factors contribute to development of LBP including injury, structural deformities, age-related changes, occupational ergonomics, psychosocial, post-traumatic stress disorder and lifestyle factors.4,5 In particular, exposure to workplace and lifestyle factors account for more than a third of disability burden.1 North America productivity losses attributed to occupational ergonomic factors have been reported as the highest economic losses worldwide.6
In primary care, a considerable number of patients (up to 48%) transition from acute to chronic LBP7 with lifestyle-related factors, baseline disability, and psychological comorbidities associated with this transition.7 In the United States, LBP treatment is among the highest healthcare expenditure with an annual increase of 5.3%8,9 and estimated US$1920 in productivity losses per person.10 Furthermore, LBP is the most frequent reported reasons for allied health and primary care physician visits,11,12 and ranks as one of the top presenting complaint in emergency settings in Australia and North America.13
First line of therapy for patients with LBP depends on the functional limitation, origin and severity of pain. The primary goal of therapy is to manage pain, reduce disability as well as restore functional loss and productivity.14 Treatment options for LBP broadly include pharmacological, non-pharmacological (rehabilitative) or surgical interventions. Pharmacotherapy for management of LBP irrespective of the duration of symptoms includes paracetamol and Non-steroidal Anti-inflammatory Drugs (NSAIDs) as first options with muscle relaxants or antidepressants recommended by clinical practice guidelines as second-option medication.15 However, the effect sizes of these drugs are small, and there is potential for serious adverse effects with limited supporting evidence on benefits for long-term use in management of LBP.16 Non-pharmacological treatments such as chiropractic, physical therapy, exercise, and cognitive behavioural therapy have been found to offer specific benefits in selected patients with moderate to severe LBP with no single treatment option considered superior.17,18
Surgical interventions have been shown to have similar improvements in pain and function compared to multidisciplinary rehabilitation.19 However, there are potential adverse risks and increased resource utilization associated with surgical procedures.20 In addition, following spine surgery 5% to 40% of patients with recurrent LBP are diagnosed with failed back surgery syndrome21–23 and an estimated annual cost of US $18,195 to US $21,402 per patient.24
More recently, non-surgical spinal decompression (NSD) therapy was developed as a novel spinal decompression motorized technology designed to deliver segmental distraction using a highly sensitive computerized feedback system.25 The aim of the NSD is to alleviate LBP and associated symptoms through expansion of intervertebral spaces to reduce herniation and intra-discal pressure while restoring disc height during treatment.26,27 NSD therapy offers several biomechanical advantages over conventional traction therapy. Firstly, distraction tension applied in NSD therapy can significantly reduce the intradiscal pressure (-100 to -600 mmHg) in the nucleus pulposus of herniated discs.28 This negative pressure inside the spinal canals occurs through the expansion of intervertebral foramen resulting in improved oxygen and nutrient uptake which can promote disc rehydration and minimize pressure on nerve roots facilitating disc regeneration and relief of stress on facet joints.28,29 Secondly, distraction intensity in NSD therapy can be gradually increased without causing reflex paraspinal muscle contraction thus allowing for application of a greater decompression force which is controlled by a computerized feedback mechanism.30 Another important advantage of NSD therapy in addressing herniated disc is that unlike conventional traction, the stress on posterior longitudinal ligament is reduced which in turn relaxes the posterior lumbar paraspinal muscles and reduces the internal pressure of the disc.26,31 Several studies have demonstrated effectiveness NSD treatment in improvement of pain and function of patients with LBP and associated symptoms.32–35
Therefore, the purpose of this report was to examine clinical outcomes of LBP using NSD combined with other conservative treatments for patients with LBP and associated symptoms. Considering the increasing global prevalence of LBP, economic and disability burden, opioid pain medication crisis in United States, as well as the substantial cost associated with spinal surgical procedures, NSD may offer a viable non-invasive treatment of choice for those patients with LBP who do not improve with conventional treatments.
Imaging Protocol
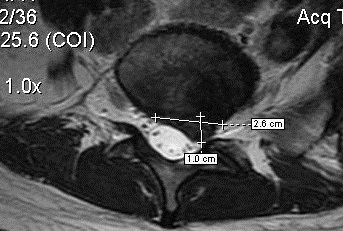
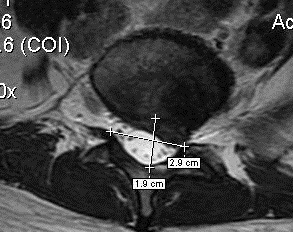
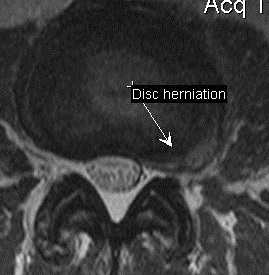
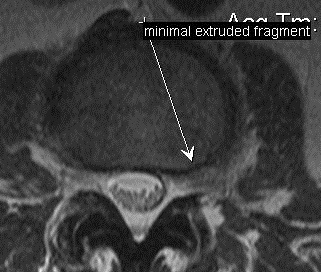
To determine the change in herniated disc following NSD therapy, Magnetic Resonance Imaging (MRI) was performed before the start of therapy and four to six months after the end of all therapy sessions. MRI of the lumbar spine was performed utilizing a 1.5 T magnet. Standard imaging with sagittal T1, T2 and STIR sequences along with an axial T2 sequence were obtained. The type of herniation including disc protrusion, extrusion, and sequestration was indicated. To evaluate the dimensions and volume of the intervertebral disc herniation, the herniation index was used as described previously.31 The herniation index was calculated utilizing the axial image demonstrating the greatest degree of distortion of the posterior intervertebral disc margin. The calculation involved multiplying the maximal anteroposterior (AP) dimension of the intervertebral disc herniation by the width of the herniated disc material (Figure 1) and then dividing this value by the product of the sagittal diameter of the spinal canal and the width of the spinal canal at the same axial level. (Figure 2) The formula for the calculation is described in Herniation Index equation.


Herniation Index equation: AP disc herniation X Width disc herniation/AP sagittal canal X Width sagittal canal X 1000 = Herniation Index
Figure 1 is divided by Figure 2. The product is multiplied by 1000. The resulting value is the herniation index.
NSD Treatment Protocol
The NSD treatment protocol included 20-30 sessions of spinal decompression over an 8-to-10-week period with 20 to 30 minutes active treatment sessions. At the start of each session, the treating clinician positioned the patient lying supine on a specialized decompression table fitted with adjustable body harnesses. To initiate active treatment, based on a computerized algorithm the decompression table gently stretched the spine of the patient. As the patient’s muscles resist the applied distraction, sensors detect this resistance and reduce the tension until muscles are relaxed before applying the stretch again to achieve maximum decompression.
The ratio of hold to rest time was 1:1 and the oscillation ranged from 10%-50% decrease between hold and rest. This indicated that if the patient was stretched at 60 pounds, the table hold was at full strength for 30 seconds, then reduced hold for 30 seconds in the range of 54 to 30 pounds followed by 60 pounds.
CASE REPORTS
Case One
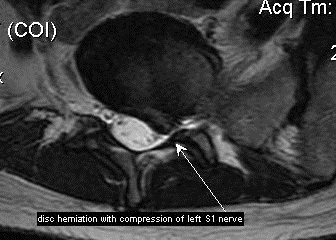
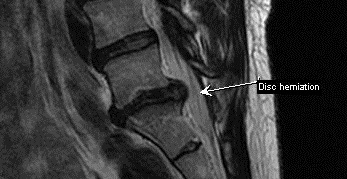
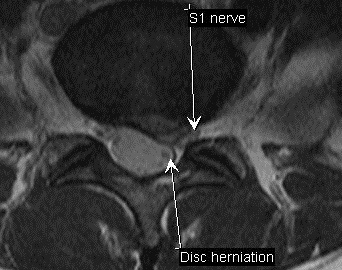
A 36-year-old female had severe low back pain and referring pain into her left calf. She rated her low back and leg pain intensity a 10/10 on the Visual Analog Scale. (VAS) The patient had experienced recurrent lower back pain in the past with rapid recovery through chiropractic care. Prior to attending the clinic, the patient has been experiencing lower back and leg pain in the last few months with little relief. One week prior to presenting, she sustained an injury during weightlifting at the gym and her pain increased to 10/10 on VAS. The patient quality of life was drastically affected by pain as she was unable to carry out daily life activities such as inability to pick up her children, perform household chores, walk, exercise, sleep or work effectively. She was referred for an MRI of her lumbar spine which revealed at L5-S1 level a prominent paracentral discal herniation measuring 25 mm wide and 11.7 mm in the AP dimension (Figure 3) with 511 calculated as the herniation index value. There was a severe compression of the left S 1 nerve root noted. (Figure 3) A sagittal view of the disc herniation at L5-S1 is provided. (Figure 4)
The treatment plan for this patient consisted of NSD combined with low level light therapy, electrical muscle stimulation, strength training with power plate, cold pack, manual therapy and chiropractic manipulation as needed for eight weeks. After two months, the patient reported 90% improvement with full recovery after three months where she resumed normal daily activities. At four-month follow-up post-treatment, the patient continued to be pain free. The patient MRI showed a 29.5% decrease in size of the disc herniation at L5-S1 with the intervertebral disc herniation measuring 18 mm wide and 10.8 mm in the AP dimension. (Figure 5) Based on MRI findings, 360 was calculated as the herniation index. The left S 1 nerve root is now visible on the axial image. (Figure 6) Figure 5 is the sagittal image of the post treatment MRI of this patient.


Figures 3 and 4. These findings are from the preliminary MRI of patient 1. The axial (Figure 3) and sagittal (Figure 4) images are used to demonstrate the disc herniation at L5/S1. There is a complete compression of the left S1 nerve root noted between the disc herniation and the lamina/facet of the left posterior arch.


Figures 5 and 6. These images, sagittal (Figure 5) and axial (Figure 6), are taken after a period of 8 weeks of NSD therapy combined with conventional chiropractic care. There is a change in signal intensity of the intervertebral disc herniation. The intervertebral disc herniation has decreased in size. The left S1 nerve root is now visible in the left subarticular recess. (Figure 6) A reduction in compression of the left S1 nerve root is indicated.
Case Two
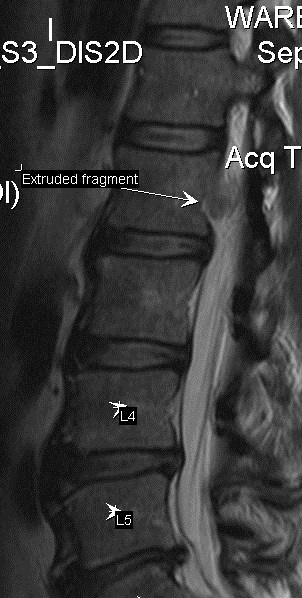
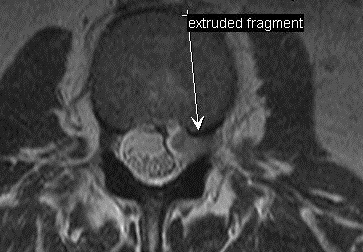
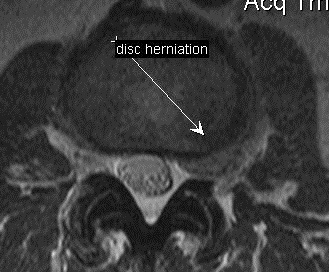
A 54-year-old male had moderate low back pain and referring pain into his left anterior thigh extending to the knee for the past 4 weeks. There was no history of trauma and pain reportedly started during recovery from an illness. The patient rated low back and leg pain intensity a 7/10 on the VAS. He received conservative management for 3 weeks until an MRI was ordered. During this treatment, the patient reported hearing a pop while leaning forward and rated his pain intensity on a VAS as 10/10. The MRI identified several disc lesions. At the L2-L3 vertebral level, a large left foraminal disc extrusion measuring 8 mm by 19 mm wide with a cephalic migration of disc material measuring 18 mm was identified. Figure 7 (sagittal view) identifies the mass of disc material in the left neural canal at the sub-pedicle level L 2. An axial view at the L2-L3 disc level (Figure 9) and an axial view in the sub-pedicle level of L 2 (Figure 8) are provided to further illustrate this disc herniation. At this intervertebral disc level, a herniation index of 319.5 was determined. At the L4-L5 vertebral level a 3.3 mm circumferential disc bulge was demonstrated. At the L5-S1 level a central disc protrusion of 13.3 mm wide and 6.3 mm in the AP dimension with a herniation index of 153.6 was identified.
The treatment plan for this patient included NSD together with low-level light therapy, electrical muscle stimulation, strength training with power plate, cold pack and manual therapy. After 2 months of this combined treatment, he reported 90% improvement in pain intensity with no referring pain into left leg.
At 5-month follow-up post therapy, MRI showed considerable reduction in the disc herniation at multiple lower lumbar spine levels. (Figures 10-12) The intervertebral disc at the L2-L3 level demonstrated a 7 mm by 19 mm disc herniation with a value of 267 for the herniation index. There was a 4-mm cephalic migration of disc material which had reduced by 14 mm (Figure 10) and there was no mass of herniated material visible in the left sub-pedicle region of L 2. (Figure 10) Axial images (Figure 11 and Figure 12) demonstrate the difference in appearance at the disc level (Figure 11) and above the disc (Figure 12). The percentage difference in the size of the intervertebral disc herniation at the L2-L3 level was 16.5%, over the 5 months, with a 78% change in the size of the migrated disc fragment identified during this period. At follow-up, there was no evidence of interval change of the disc bulge at L4-L5 level which is consistent with a circumferential annular bulge. The L5-S1 intervertebral disc demonstrated a 5 mm by 12.3 mm central disc protrusion with a calculated 122.6 herniation index which represented a 20.2% reduction compared to the initial presentation.



The MRI findings of the herniated mass along the posterior body margin of L 2 is identified on sagittal (Figure 7) and axial (Figure 8) images. The herniation at the L2-L3 disc level is appreciated on Figure 9.



Following 8 weeks of NSD therapy, follow-up magnetic resonance imaging is taken. The mass of the extruded disc material is significantly reduced and no longer visible along the posterior body margin of L 2. (Figure 10) The size of the disc herniation is reduced in the intraforaminal region at the disc level (Figure 11) and above the disc level. (Figure 12)
Case Three
A 45-year-old male had low back pain and radiating pain into his left calf rating pain intensity at an 8/10 on the VAS. There was no history of recent injury and pain reportedly started four months prior to presentation at the clinic. The patient reported a lower back injury eight years prior with complete resolution. Before attending the clinic, 2 months prior an MRI showed an L4-L5 disc protrusion which measured 21 mm wide, 11 mm in the AP dimension and with a 5 mm cephalic migration of disc material. There was impingement on both the right and left L5 spinal nerve roots. There was also severe degenerative disc disease present at L5-S1 and posterior displacement of the nerve roots at the subarticular recess level. The herniation index of 375.1 was calculated
The patient had received 2 epidural injections during the past 4 months, with very little relief. His chief complaint was waking up multiple times during the night with severe pain, which was also present during walking, sitting, and other physical activities.
The treatment plan for this patient included a combination of NSD therapy with low level light therapy, electrical muscle stimulation, strength training with power plate, cold pack, manual therapy and chiropractic adjustments for 3 months. Following this, the patient reported 75% improvement in pain and was able to have uninterrupted sleep. At 5-month follow-up, the patient had fully recovered and returned to full daily activities. At the 6-months follow-up post-intervention, MRI showed reduced disc herniation and inflammation around the L5 right nerve. At the L4-L5 vertebral level the disc herniation measured 19.3 mm wide and 11 mm in the AP dimension. A cephalic migration of disc material extending approximately 5 mm above the inferior endplate of L4 was present. The herniation index of 340 was calculated which represented a decrease of 9.4% in size of the disc herniation.
Case Four
A 59-year-old woman had persistent lower back pain and right leg pain extending to her right ankle. She rated her pain intensity a 7/10 on the VAS. The history revealed previous recurrent episodes of lower back pain which were resolved with Chiropractic care. The patient had sustained an injury to her low back during kayaking 4 months earlier with unsuccessful treatment. Her chief complaint was pain during daily activities such as walking, driving and working. MRI revealed an L5-S1 disc protrusion measuring 10 mm abutting the right exiting L5 nerve root. A disc herniation measuring 30 mm wide and 8.3 mm in the AP dimension at the L4-L5 level with evidence of annular tear and a resultant herniation index of 452 was identified on the imaging study.
The treatment plan for this patient included application of NSD combined with low level light therapy, electrical muscle stimulation, strength training with power plate, cold pack and manual therapy. She reported 80% improvement after 4 weeks of treatment, with complete recovery at 6 weeks. She found her quality of life had considerably improved and she was now able to enjoy driving, sleeping and working. At six-month follow-up post-treatment, the MRI showed considerable resorption of the L5-S1 disc herniation with no pressure on the exiting right L5 nerve. The disc herniation at L4-L5 measured 26.7 mm wide and 7 mm in the AP dimension, with a calculated herniation index of 320.4 which represented a 29.1% reduction at follow-up.
Discussion
After three decades, LBP remains as the most common condition contributing to long-term sickness absence, early disability payment and retirement.36 Treatment ranges in cost and invasiveness from conservative therapies to surgical intervention with lack of agreement on the most appropriate LBP management strategy. The considerable research in understanding the aetiology of LBP and progress in identifying appropriate treatment options has not translated into the development of more effective and safer therapies to lower prevalence of LBP epidemic. Given the considerable impact of persistent back pain on the health-related quality of life and economic cost, it is critical to manage LBP effectively and identify strategies to prevent its transition to chronic pain.37 The current research study investigated the impact of NSD therapy on patients with LBP and demonstrated that NSD was an effective treatment option when combined with other modalities to alleviate pain in patients with LBP and associated symptoms. All 4 patients achieved full recovery from pain with clinically meaningful reduction of their disc herniation and significant improvement in quality-of-life following NSD combined with conservative therapy.
Despite lack of quality systematic review on efficacy of NSD, several randomized controlled trials have shown the effectiveness of NSD therapy for managing LBP and symptoms associated with lumbar radiculopathy as well as lumbar disc herniation or protrusion compared with other modalities.26,32,38 The findings of our study are consistent with previous controlled trials that have demonstrated effectiveness of NSD therapy when combined with other conservative interventions.32–35 In an earlier controlled study of patients with chronic LBP, NSD therapy combined with physical therapy was more effective at reducing pain from moderate to minimal disability. and improving function than conservative treatment as stand-alone (hot-pack, interferential current therapy and ultrasound).35 A more recent study found that in patients with subacute lumbar radiculopathy, combining NSD with routine physical therapy was more effective at reducing pain intensity and functional disability while improving lumbar range of motion and quality of life compared to physical therapy alone.32 In patients with LBP due to chronic lumbar disc prolapse, NSD therapy combined with core stabilization exercises was significantly more effective at reducing pain and disability than core stabilization exercises alone.34 Similarly, in patients with pain in the lumbopelvic region, a combination of NSD therapy with conventional physiotherapy and lumbar stability exercise showed better outcomes in terms of pain and disability scores than those of the control group.33 Collectively, these findings support our findings and application of NSD as a promising non-invasive adjunct to conservative treatment approaches for management of the patient with LBP and associated symptoms.
Conclusion
The current study further adds to the accumulating evidence that have demonstrated the potential of NSD as an effective and safe therapy for management of patients with LBP and associated symptoms. This case series also highlights the benefit of imaging findings to demonstrate the clinical improvement in pain and function of patients with LBP. Prospective and controlled trials are needed to confirm our findings and investigate the impact of NSD on clinical and radiographic measures in patients with LBP compared to other conservative modalities.