
Introduction
Low back pain (LBP) is a condition affecting more than 500 million people,1 making it the number-one cause of disability worldwide.2 Between 60%-85% of people will experience LBP at some point in their life.3 Additionally, nonspecific-LBP – defined as LBP without evidence for a specific cause4 – can make diagnosis, treatment, and categorization difficult. It is estimated that up to 90% of all LBP cases are nonspecific.5 The difficulty in establishing a clear etiology for nonspecific-LBP can lead to unnecessary medical procedures,6 prolonged pain, and increased healthcare costs.7 In total, the financial burden of nonspecific-LBP in the United States is estimated to cost anywhere from $80-$600 billion or more per year,8 with the majority of this financial toll stemming from work loss or other household productivity loss.8 Chou and Shekelle found that time taken away from work was heavily influenced by psychosocial factors, such as pain coping behaviors and fear avoidance.9
Patients with nonspecific-LBP are generally encouraged to continue with their activities of daily living, as activity is more beneficial than rest for timely recovery.10 While a variety of physical activities have been shown to improve chronic nonspecific-LBP, the specific type of activity yielding the most benefit has yet to be determined.11–14 Similarly, many conventional biomechanical and ergonomic interventions (e.g., insoles, back braces, and education on proper lifting techniques) yield minimal benefit.15,16 Beyond conventional interventions, other non-pharmaceutical approaches have demonstrated effectiveness for nonspecific-LBP. These include acupuncture, spinal manipulation, massage, and traction, as well as mind-body interventions such as yoga and mindfulness-based stress reduction. While these therapies typically lead to modest, short-term improvements in pain levels, they may be most beneficial when integrated into a multidisciplinary rehabilitation approach.17
Pharmacologic interventions for nonspecific-LBP are usually limited to pain management, often to support the capacity to do physical exercises.18 Typically, non-steroidal anti-inflammatory drugs (NSAIDs) are used as a first line treatment for nonspecific-LBP. NSAID usage is recommended for the shortest duration of time19,20 and not all NSAIDs may be indicated. Recent evidence suggests acetaminophen may offer minimal benefit to the patient for pain or mobility issues.21 In persistent cases of nonspecific-LBP, opioids have been used, though there is evidence correlating its use to extended disability claims when prescribed within the first six weeks of an injury.22 Additionally, while opioids have historically been used to treat persistent LBP, their use carries significant risks. Research shows that long-term opioid therapy for chronic pain is linked to several adverse outcomes, including heightened risk of overdose, substance abuse, bone fractures, heart attacks, and sexual health issues.23 These risks appear to increase with higher doses.23 Invasive treatment strategies, such as surgery, percutaneous procedures, analgesic procedures, local anesthetics, and corticosteroids for nonspecific-LBP should also be avoided, as there is low level evidence supporting their use.24,25
One of the challenges with managing nonspecific-LBP is that research has shown there are distinct subcategories of patients, with some groups responding better to certain treatments than others.26 For example, studies have demonstrated that specific clusters of physical and psychosocial factors can predict which patients are more likely to benefit from manual therapy interventions.27 This recognition of patient subgroups has led to the development of classification tools to help guide treatment decisions. The Keele Start Back Tool (SBT) represents one such approach to patient stratification.28
The Keele Start Back Tool (SBT) is a validated questionnaire that can be used to stratify nonspecific-LBP patients into groups based on prognostic indicators for treatment.29 Patients are stratified as low, medium, or high-risk groups based off their responses to the questionnaire.28 Each subgroup contains different degrees of morbidity and recommendations for specialist intervention. The SBT aims to shorten the time needed to see a specialist, thereby reducing pain, financial burden, and psychological trauma.28,29 Effectively, the SBT allows practitioners to triage patients into different treatment pathways that match their clinical profile. Low risk subgroup population are recommended to be treated by primary care physicians or physical healthcare providers, as best-practice guidelines suggest they can be successfully treated with over-the-counter medications, stretches, and exercise. Medium risk subgroup population should be seen by physical healthcare providers (e.g., chiropractors and physical therapists), in addition to their primary care physicians. Finally, high risk subgroup population should be seen by both primary care physicians and physical healthcare providers, but also seek cognitive-behavioral therapy. Goertz et al30 demonstrated how chiropractic manipulation can aid in pain and disability reduction due to LBP, along with usual medical care in a military population with LBP.30 This study explores the application of the SBT questionnaire within a chiropractic training setting in the United States.
Methods
Approval to conduct this study was granted by the Institutional Review Board at Parker University (#A-00170). This prospective observational study collected data from all new LBP patients between the ages of 18-65 years presenting to the Parker University Wellness Clinics located in Dallas and Irving, TX between March 5th, 2018, and April 6th, 2018. Forms in Spanish were provided for native Spanish speakers. Excluded from screening were Parker University students, employees, direct affiliates, and alumni.
Study data were collected via iPad and managed using REDCap electronic data capture tools hosted at Parker University. REDCap (Research Electronic Data Capture) is a secure, web-based application designed to support data capture for research studies, providing 1) an intuitive interface for validated data entry; 2) audit trails for tracking data manipulation and export procedures; 3) automated export procedures for seamless data downloads to common statistical packages; and 4) procedures for importing data from external sources.31,32 All data were collected in an anonymous format, and no personal identifiers that could link participants to the data were ever collected. Participation was voluntary, and respondents were not compensated for taking part in the study. After each new patient reviewed the consent form and signed it, they were asked to complete a questionnaire that recorded their age, sex, weight, height, ethnicity, race, employment status, educational status, smoking status, and duration of LBP. Participants were also asked about their expectation of improvement from care.33 For this question, participants were asked to rate their expectation of improvement from 0 to 100, with 0 meaning no chance of improvement and 100 meaning a very probable chance of improvement. Then the SBT questionnaire was administered to stratify LBP patients into 3 risk groups. This questionnaire has 9 items that asks about pain, disability, fear, anxiety, and depression.28 All items were answered with agree1 or disagree (0), except a single question (“Overall, how bothersome has your back been the last two weeks?”) which had a 5-point rating scale ranging from not at all (0), to slightly (0), moderately (0), very much1 and extremely1 bothersome. Total scores ranged from 0 to 9 (best to worst prognosis). The last 5 items of the SBT are used to create a psychosocial subscale with 5 as the maximum score (with 5 indicating high risk for development of chronic LBP.28 Overall scores between 0 and 3 stratify into the low-risk group; medium risk is categorized by overall scores of at least 4, with maximum psychological sub-scores of 3; and finally, high risk is categorized by scores of 4 or 5 on the psychosocial subscale. The SBT was developed for LBP patients seeking care from primary care physicians34 and further evaluated in several patient populations.35–37 No introduction of the SBT was given to students or supervising clinicians for this project. See Appendix A for a copy of the SBT which was administered to all patients.
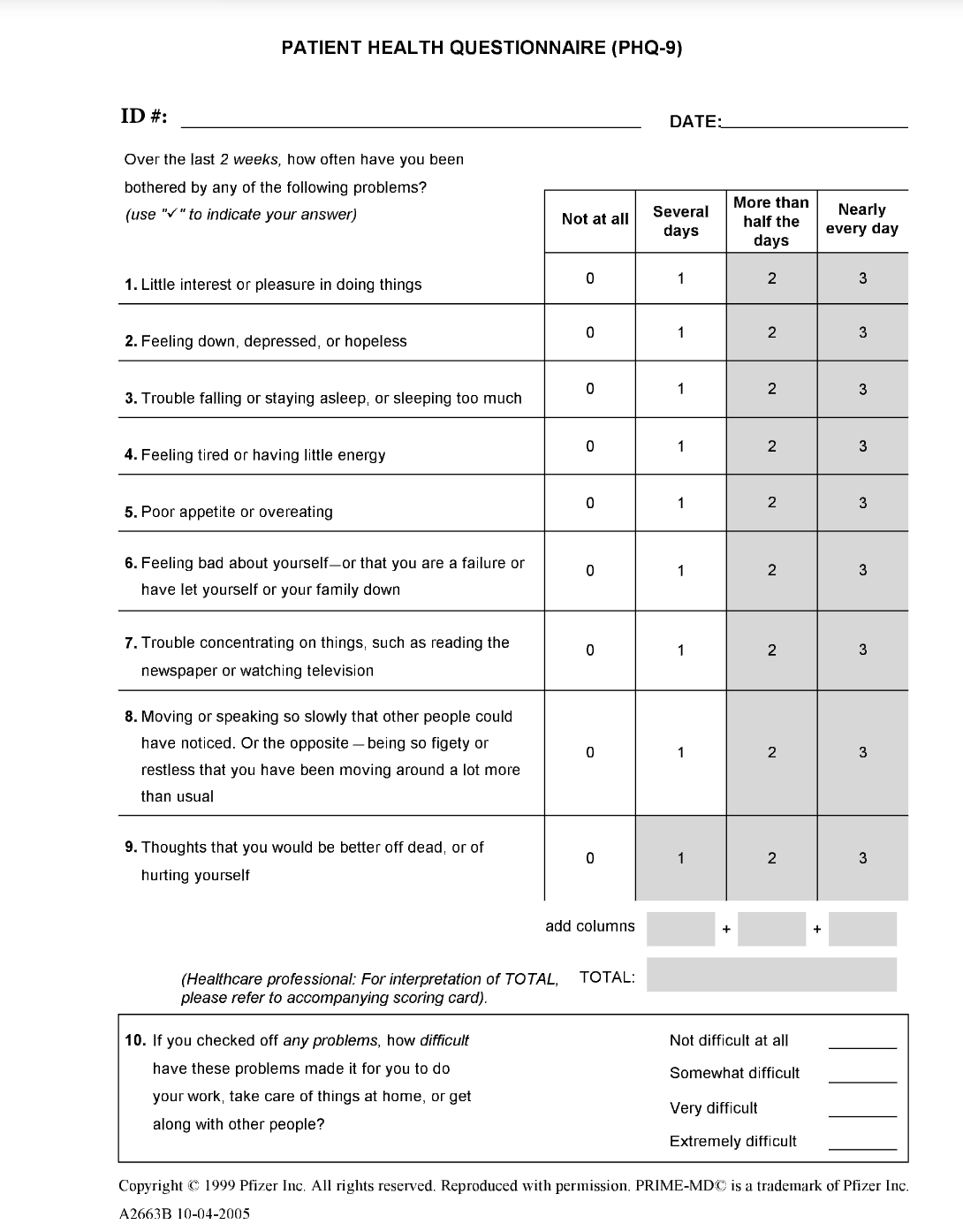
High-risk patients were also prompted to complete the Patient Health Questionnaire-9 (PHQ-9) questionnaire to evaluate depression status.38 The PHQ-9 tool is a validated depression measuring tool with generalizable capabilities, including in the primary care and obstetrics-gynecology fields, and strongly correlates with other measure of depression.38 All patients with answers that pointed to self-harm or suicidal ideation were immediately followed up with by the study investigator and faculty doctor. This follow-up included mental health resources and documentation in the patient’s healthcare records. See Appendix B for a copy of the PHQ-9 which was administered to high-risk patients only.
For all patients that completed the SBT, a chart review of the first 4-weeks of care was completed to retrieve patient follow-up information and treatment provided. The chart review included chief complaint, history, range of motion, neurological, orthopedic, and palpatory examination data, as well as Oswestry Disability Index (ODI)39 and Visual Analog Scale (VAS)40 for pain intensity (0 = no pain, 100 = worst pain imaginable) scores from the initial visit. Follow-up visits collected date of treatment and Numerical Rating Scale (NRS)41 for pain (0 = no pain, 10 = worst pain imaginable). All data were used to calculate descriptive statistics with Microsoft Excel.
Results
Of the 188 new patients screened, 163 (86.7%) met eligibility criteria and were invited to participate. Of those 163, 87 (53.4%) were interested in participating and completed the baseline survey. The reasons for exclusions were: 6 did not meet age criteria; 49 did not have LBP; 21 did not sign the consent / declined to participate. Demographic data of the enrolled participants are shown in Table 1.
Low-Risk Subgroup
As shown in Table 1, the low-risk subgroup had 57 participants. The majority were female (n=31, 54.3%) with an average age of 34.6 (±14.77) years. Participants reported their race as mostly Caucasian (n=39, 68.4%) or African American (n=7, 12.3%) and were predominantly non-Hispanic (n=41, 72.0%).
Most participants (n=40, 71.4%) reported being currently employed, with others reporting being unemployed/laid off (n=9, 16.1%) or disabled/on leave (n=7, 12.5%). Educational status ranged from high school or less (n=6, 10.7%), some college/occupational training (n=9, 16.1%), associate’s/bachelor’s degree (n=33, 58.9%), master’s degree (n=6, 10.7%), to doctorate (n=2, 3.6%).
Pain and Treatment
The majority of participants experienced LBP for either less than 1 month or greater than 1 year. The average VAS at baseline for this group was 31.6 ± 19.2. Participants in this subgroup had an average expectation of significant improvement of 67.8/100 (SD: 21.4).
Of the 57 participants in the low-risk subgroup, 47 (82.5%) participants received at least 1 treatment during the study. For those receiving treatment, the average number of visits was 3 (SD: 1.91) with a range of 1 to 8 visits. Only 6 (10.5%) of the participants in this subgroup had their four-week evaluation. Out of these, the average number of visits was 6.5 ± 4.62 with a range of 0 to 14 visits within the four-week period. The average NRS change (from first to last visit) was 1.0 (±2.2).
Medium-Risk Subgroup
As shown in Table 1, the medium-risk subgroup had 24 participants. The majority were female (n=18, 75.0%) with an average age of 37.3 (±14.94) years. Participants reported their race as mostly Caucasian (n=19, 79.2%) or Asian-Pacific Islander (n=4, 16.7%) and were predominantly non-Hispanic (n=14, 58.4%).
Among those reporting employment status (n=21, 88%), most were currently employed (n=14, 66.7%), with others reporting being unemployed/laid off (n=4, 19%), disabled/on leave (n=2, 9.5%), or being a student (n=1, 4.8%). Educational status ranged from high school or less (n=3, 12.5%), some college/occupational training (n=7, 29.2%), associate’s/bachelor’s degree (n=11, 45.8%), to master’s degree (n=3, 12.5%).
Pain and Treatment
Participants reported LBP duration ranging from less than 1 month to greater than 5 years, with approximately half experiencing LBP for more than 1 year. The average VAS at baseline was 50.2 (±17.6). Participants had an average expectation of improvement of 73.6/100 (±20.2).
Of the 24 participants, 18 (75.0%) received at least 1 treatment during the study. For those receiving treatment, the average number of visits was 4.1 (±3.51) with a range of 1 to 13 visits. Only 5 (20.8%) completed their four-week evaluation, with these participants averaging 6.2 (±3.04) visits (range: 3-10) within the four-week period. The average NRS change from first to last visit was 0.2 (±2.07).
High Risk Subgroup
The high-risk subgroup had 6 participants. Half were female (n=3, 50.0%) with an average age of 42.0 (±15.49) years. Participants reported their race as mostly Caucasian (n=5, 83.3%) or African American (n=1, 16.7%) and were predominantly non-Hispanic (n=5, 83.3%).
Half of the participants were currently employed (n=3, 50.0%), with others reporting being unemployed/laid off (n=1, 16.7%) or being a student (n=2, 33.3%). Educational status ranged from high school or less (n=1, 16.7%), some college/occupational training (n=2, 33.3%), associate’s/bachelor’s degree (n=1, 16.7%), to master’s degree (n=2, 33.3%).
Pain and Treatment
LBP duration ranged from less than 1 month to greater than 5 years with an even distribution throughout the sample. The average VAS at baseline was 63.0 (±12.1). Participants had an average expectation of improvement of 84.0/100 (±16.8).
All participants (n=6, 100%) received at least 1 treatment during the study. The average number of visits was 5.2 (±1.6) with a range of 4 to 8 visits. None of the participants completed their four-week evaluation. The average NRS change from first to last visit was 0.8 (±4.02). The average PHQ-9 score was 10.5 (±9.72), with four participants scoring at or above “moderate depression.”38
Discussion
This study investigated the use of the SBT in an academic, chiropractic teaching clinic in the United States without specific training for student providers, staff, and supervising clinicians. Previous research with this questionnaire has primarily been conducted in the United Kingdom, Denmark, and Norway.29,42,43 This was, to our knowledge, the first use of the SBT in an academic chiropractic clinic in the United States. The study successfully enrolled 87 participants and provided useful clinical stratifications of LBP patients seeking care at in academic setting. Additionally, it was simple to administer, and could be easily implemented. However, follow-up data were found to be extremely limited, with only 10%, 20% and 0% of the low, medium, and high-risk participants returning for care at 4-weeks, respectively. Further, given the extremely low follow-up across all groups, and particularly the high-risk group – where psychosocial variables are of greater prevalence – it is important that any use of the SBT in an academic, clinical setting also focus on training for continuity of care and patient follow-up.
Of the patients that received at least 1 visit, the low-risk group had the lowest average treatment visits, NRS and Oswestry scores compared with the medium-risk and high-risk groups. While these data are preliminary, it does support that the SBT appears to adequately stratify patients presenting to an academic chiropractic clinic. However, despite the relative success in implementation of SBT in this study, a substantial number of patients did not continue with care to the 4-week re-evaluation. In the medium and high-risk group, these dropouts are concerning. It is unclear from our data collected from the clinic records, if patients switched providers, improved fully, or indeed, were now dealing with their musculoskeletal and psychosocial ailments on their own.
While our data do not provide exact causes for the low rate of patient return at 1 month, there are several potential factors to consider. First, it is possible that patients experienced a full abatement of their chief complaints. While this potentially feasible in the low-risk group, where complaints are more likely to be uncomplicated, it becomes increasingly dubious in the medium and high-risk groups, respectively. Similarly, while it is possible that these patients sought alternative care, this is unknown as well as to whom or what they may have self-referred. Instead, we consider this study as leading evidence that continuity of care may have played an outsized role in patient dropout. This study collected through the transition period between two scholastic periods (in this case, trimesters). More specifically, data collection began one week before the end of the spring trimester, carried through a 2-week break, and into the start of the next summer trimester. While the clinics do not close during this period, their total activity does decrease. During this period, vacations are common, and it is expected that student providers will begin to rotate under new supervising clinicians, leave the student clinics for an outside clinical rotation, or indeed, even graduate. When student providers rotate or leave the clinics, it is a common practice for their patients to remain under the care of the supervising clinicians (and likely a new student provider), rather than attempt to follow the original student to a new location or group.
With this in mind, it is entirely possible – likely even – that these patients were caught in between multiple student providers. These student providers may or may not have been using the SBT, or even have been able to continue the care being provided by the previous student provider. As such, flare ups, lack of care and/or having to re-establish trust and confidence with a new provider or modality could all be exacerbating factors to dropout. This, in turn, highlights a greater problem with 1) standardization across providers44 and 2) continuity of care across providers in an academic clinical setting. As such, it is important that future use of the SBT in an academic, clinical setting not only track patient dropout more closely – and attempt to understand why these events are happening – but also implement a plan based on providing as continuous and similar care as possible, to ensure that patients are not “getting lost in the shuffle.”
Knowing the depression scores utilizing the PHQ-9 provides us an opportunity to compare the scores of the SBT to further understand the accuracy of the tool within a chiropractic academic clinic. Bener et al45 demonstrated a correlation of psychological factors, including depression, to LBP. Additionally, Henschke, Maher, & Refshauge46 provided evidence of the detriment of depression to exasperate LBP morbidity. Understanding the degree of depression associated with LBP morbidity using the SBT may provide valuable insight into LBP treatment in the future.47
Limitations
This was a preliminary study and is not without limitations. First, the applicability of this study to other healthcare professions is limited. Work by Field suggests that there may be differences in high-risk patients within chiropractic settings compared to those carrying high-risk in primary care medical settings.48 Further, Beneciuk notes that significant differences exist between patients that self-refer for chiropractic care versus those referred by their primary care physicians.49 The population seen at an academic chiropractic institution may not reflect the same patients seen in other clinics and/or by other healthcare professions. That being said, this is the first study to examine chiropractic patients in an academic teaching clinic in the United States using the SBT and may be transferable to similar American chiropractic educational programs. Lack of data for later patient visits (i.e., patient drop-out) is also a limiting factor in this study. Though the information contained in this study point to plausible factors, the study design precludes a full understanding of these findings. Future studies should be designed to examine these questions.
Conclusion
It appears that the SBT is easy to administer in a US academic clinical setting to patients who present with musculoskeletal pain and for clinicians to interpret, requiring only minutes to complete.36 However, future studies should exercise caution regarding patient attrition and incorporate organized follow-ups for patients who discontinue care.
Acknowledgements
The authors thank Parker University and the associated students and staff that assisted with the implementation of the research.
Funding and Conflicts of Interest
No funding was provided for this research. The authors declare that they do not have any conflicts of interest for this research.

__387311_.png)