
Introduction
Neurofibroma, a benign tumor, can be a sporadic solitary mass or part of a broader syndrome known as neurofibromatosis type 1 (NF1).1 The presence of multiple neurofibromas is seen with the diagnosis of NF1, which is caused by autosomal dominant gene mutations.1 Recently, the use of next-generation sequencing has been developed and used to identify the gene mutations of NF1 to aid in diagnosis of the syndrome.2 Diagnosis of an individual mass as a neurofibroma is accomplished via diagnostic imaging and biopsy, detailed later in this manuscript.3 While the prevalence of isolated neurofibromas is unknown, NF1 is the most common neurocutaneous syndrome, estimated to effect 1 in 3000 individuals.4 Typical presentations of NF1 involve numerous hyperpigmented skin macules known as café-au-lait spots, skin neurofibromas, and potential optic gliomas, central nervous system tumors, peripheral or spinal neurofibromas, and skeletal abnormalities.4 Neurofibromas extend from Schwann cells, but also contains fibroblasts, mast cells and other components which differentiates these from Schwannomas.5
Neurofibromas can be subtyped into diffuse, plaque-like skin enlargements; localized, intraneural tumors affecting a solitary site; or plexiform, affecting multiple nerve fascicles and associated with large nerves and plexi.6 When affecting nerve roots, the tumor has been seen to be more infiltrative, entrapping sensory ganglion cells and making resection more challenging for fear of affecting the nerve fascicle.5 Solitary intraneural neurofibromas are seldom associated with NF1, as opposed to plexiform which has become pathognomonic for the condition.5,6 Plexiform neurofibroma also has the potential to become malignant, and exclusively occurs with NF1 patients.7 Pain is the most common symptom of neurofibromas, though it has been shown that less than 5% of NF1 patients have symptomatic lesions.3 A recent retrospective study of lumbosacral plexus tumors that underwent surgery, found 22.5% of these to be neurofibroma in origin with 59.5% of total patients reporting leg pain as the most common symptom.8
This case describes a patient with solitary intraneural neurofibroma of the left lumbosacral plexus. He was deemed not a candidate for surgical intervention and instructed to trial conservative treatment for symptom management.
CASE REPORT
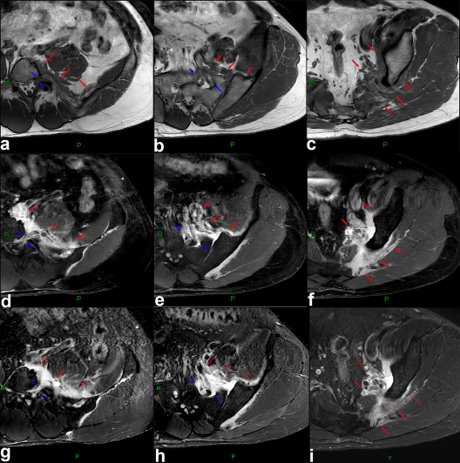
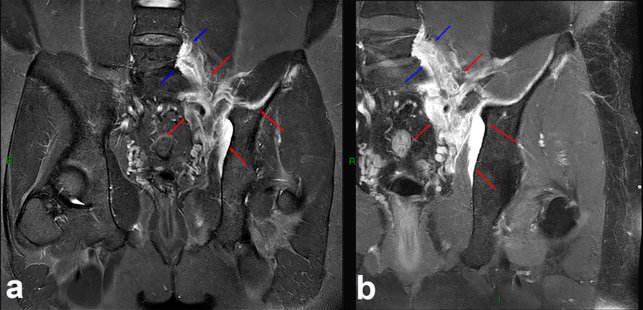
The patient provided written consent for publication and his case was approved by the Privacy Officer. We followed CARE guidelines of reporting for case reports.9 A 33-year-old Asian male was referred, by their VHA primary care provider, to a Veterans Health Administration (VHA) chiropractic clinic for lower back and left hip pain. Between time of referral placed and him being seen by us (approximately 4 months), magnetic resonance imaging (MRI) of the left hip was ordered due to ongoing pain. This showed nonspecific infiltrative fluid and soft tissue edema around the left sacroiliac joint, which appeared to extend toward the lumbosacral junction. VHA radiologists recommended a follow-up lumbar spine MRI, which demonstrated a STIR hyperintensity with involvement of the left L5-S1 and S1-S2 neuroforamen expanding into the left pelvic sidewall into the left iliac fossa (see figures 1 and 2). Follow-up computerized tomography (CT) was obtained, demonstrating similar perineural mass without bony involvement (figure 3). He was then referred to VHA neurosurgery department, who recommended biopsy of the mass. Shortly thereafter, he came to the chiropractic clinic for work-up with ongoing complaint of lower back pain with radiation of pain into the left lateral thigh, described as sharp and shooting. There was no numbness/tingling or weakness of the leg; pain occurred with walking and prolonged standing. He had been unable to find any palliative measures. He had trialed physical therapy 1 year prior without benefit. Review of systems were remarkable for anxiety and depression, managed by VHA mental health services and and he was HIV positive and being managed by VHA infectious disease people. He rated pain intensity and interferences with an average pain as a 7 out of 10, pain’s interference in enjoyment of life 8 out of 10, and pain’s interference with general activity 8 out of 10 (PEG scale).10
_including_select_axial_t1_pre-contrast_(a-c)__axial_t1_po.jpeg)
_and_t1_post_contrast_(b)_mri_images_demonstrate_similar_imaging_character.jpeg)
_image_demonstrates_a_soft_tissue_density_mass_(red_arrows)_.png)
On examination, the patient was neurologically intact with muscle stretch reflexes of the lower extremities 2+ bilaterally, muscle strength 5/5 and sensation to light touch normal in both extremities. He performed Romberg’s position, heel and toe walk without difficulty. Clonus was absent bilaterally with rapid ankle jerk, as was Hoffman’s reflex. Moderate restrictions in lumbar flexion and extension and minimal restriction with bilateral lumbar lateral flexion were observed. Lumbar extension and lateral flexion bilaterally produced left hip/lateral thigh pain. Straight leg raise on the left was positive for lateral thigh pain. Prone hip internal rotation produced localized pain in the left hip. Hypertonicity and tenderness was noted of the bilateral lumbar paraspinal and left gluteal musculature. At that time, he was diagnosed with myofascial pain of the lumbar spine and left hip with radicular pain complicated by unknown infiltrative mass of the lumbosacral plexus.
During report of findings at initial visit, we told the patient he should complete the recommended tests on the unknown mass. He was hesitant to do so, hoping the mass was benign and simply wanting non-invasive treatment to his lower back and leg for pain. We explained to the patient that no manual therapy would “fix” his current pain experience, especially without knowing in full detail if the mass was the cause of his symptoms. In addition, anything beyond light myofascial work to the area would be contraindicated at the time. He consented to this care, while agreeing to follow-up with the recommending studies on the mass.
A trial of manual therapy was initiated, consisting of myofascial work of the above mentioned hypertonic musculature using a Vibracussor® device and manual myofascial release. Approximately 6 weeks later, he had completed biopsy and received diagnosis of benign solitary intraneural neurofibroma. He was awaiting follow-up with the neurosurgery team to discuss surgical options, but in the meantime was interested in any palliative measures. We agreed to provide flexion-distraction therapy to the lumbar spine; however it was re-iterated that any benefit would likely be short-term. Over the next 4 visits, flexion-distraction did provide mild short-term decrease in lower back pain and patient had follow-up with co-management of VA Neurosurgery and Oncology teams. A follow-up MRI of the lumbar spine depicted the mass as stable. However, due to the extent of the mass, resection would result in sacrificing the L5-S2 nerve roots, and thus was deemed not a good surgical candidate. He was cleared to undergo conservative management for symptoms, but radiation therapy would be considered if symptoms progressed.
Over the following 5 visits, HVLA manipulation was trialed to the lumbar spine. At first session of this therapy, pre-load position testing was done with patient giving feedback to comfort levels and left lower extremity symptoms. He tolerated positioning, light thrust, and standard full thrust to segmental area without exacerbation of symptoms during treatment. He concurrently started working with a VHA pelvic floor physical therapist after neurosurgical team referral, with a focus on lower extremity mobility and strengthening. After 5 visits using HVLA as part of the therapeutic plan, he again completed a PEG scale rating pain as a 6 out of 10, pain’s interference in enjoyment of life 6 out of 10, and pain’s interference with general activity 4 out of 10. Over the course of an additional 5 chiropractic visits, patient noted decrease in lower back and left lower extremity symptoms with daily activities that lasted for about 1 week’s time after treatment. He is currently working towards goal of running long distances again with being able to lightly jog for one mile. He is also able to tolerate 20 minutes on a stationary bike without increased pain. At his final visit for chiropractic care, PEG scale scores remained unchanged and trial of care was completed. No adverse events occurred during course of care. Het has also completed another follow-up MRI, again showing stable mass 1 year after initial imaging.
Discussion
Current recommendations for symptomatic neurofibromas heavily lean towards resection of the lesion, if able to be performed without compromising important neural structures.10 Possible surgical interventions include hemilaminectomy, spinal fusion, and microsurgery.3 Adjuvant therapy (radiation or chemotherapy) has also been utilized when resection is incomplete or not an option.3 However, specifically in the setting of neurofibromas, evidence is lacking and mostly drawn from treatment of similar tumors.7 Evidence does exist for various medications as treatment for neurofibromas in the setting of NF1, mostly with conflicting results though.11 There is no consensus in the most optimal conservative symptomatic treatment, and such treatment is usually offered on a case-by-case basis depending on provider preference. The first report of a solitary neurofibroma, not as part of neurofibromatosis, comes from Borchardt in 1927.12 Chin reported 3 cases of solitary neurofibroma causing thigh pain, all resected with improvements in function and pain.13 Argyrakis reported a patient with right lumbosacral plexus neurofibroma causing medial thigh pain and muscle weakness that was resected with full resolution of symptoms.14
MRI is the most sensitive and specific study for imaging diagnosis of neurofibromas. Extent of the tumor and adjacent organ involvement is best characterized on MRI due to its superior contrast. On MRI, neurofibromas are typically T1 hypointense and T2 hyperintense, and demonstrate heterogeneous enhancement.6 Although MRI is superior in characterization of soft tissue involvement, CT is better at depicting possible osseous involvement.15 In addition, biopsy to detail “waxy, dark, thin nuclei embedded in thick irregular collagen fibers” is useful.3
Examples exist within the literature of chiropractic care in the setting of NF1. In 2003, Gajeski and colleagues detail the treatment of a 45-year-old woman with both cervical and lumbar neurofibromas.15 In that case, only drop-table spinal manipulation was performed to the lumbopelvic region. Cervical treatment was contraindicated due to extent of osseous changes from the neurofibromas. A more recent case from Mignelli et al depicts a 21-year-old female with cervical spine affected by NF1 neurofibromas.16 She was treated with cervical flexion-distraction and soft-tissue mobilization. Other cases exist in chiropractic literature of trials of care in the setting of masses. Cox describes treatment of a facet synovial cyst utilizing flexion-distraction manipulation.17 More recently, Chu and colleagues detail treatment of a patient’s radicular pain with flexion-distraction later to have found to be caused by a lumbar Schwannoma.18
Guidelines for chiropractic care in the setting of low back and radicular pain outline absolute and relative contraindications to HVLA manipulation. The chiropractic clinical practice guidelines for spinal manipulation of low back pain outlined that local primary bone tumors, local metastatic bone tumors, spinal cord tumors, and structural instability are absolute contraindications.19,20 Spinal manipulation in the setting of tumors or cancer is otherwise listed as a relative contraindication, and additional steps are recommended to be taken in regard to informed consent and documentation of any additional risk to the patient. It should be re-iterated that this case depicts treatment of radicular lower extremity symptoms and not the neurofibroma itself. This should also be explained to patients during informed consent with realistic outcomes and goals agreed upon before initiating a trial of care.
The transient relief of radicular pain reported by the patient is difficult to interpret. Current evidence provides a few possible contributing factors.21 First, hypoalgesia, dopamine production and opioid responses could explain decreased pain stimuli from the low back and lower extremity. Second, changes to muscle activity could produce increased functional ability in the short-term after treatment. Finally, the patient’s preconceived expectations of treatment effectiveness could contribute to improvement experienced with care.
Limitations
There is scarce evidence of conservative management in the setting of lumbosacral plexus tumors, especially with solitary intraneural neurofibromas. The individual presentation of the patient and their specific surgical options should be taken into consideration. As this patient’s care occurred at an integrated hospital setting, co-management and review of electronic health records was likely easier than in a private practice setting. In addition, provider preferences along with patient’s tolerance and preference for different treatments will influence care. This case depicts the treatment of radicular pain in the setting of solitary intraneural neurofibroma without any reported adverse events, but should not be generalized to all presentations or tumor causes of radicular pain. Trials of care should be undertaken with caution and use of gradual progression of forces, similar to that described in this case, is recommended to judge patient tolerance.
Conclusion
Solitary intraneural fibroma is a potential cause of radicular pain. Depending on extent of involvement and symptoms, surgical resection may be recommended. In cases where this is not an option, conservative management including chiropractic care may be considered to help patients manage symptoms.
Acknowledgments
The authors received indirect support from their institution in the form of computers, workspace, and time to prepare the article. The views expressed in this article are those of the author and do not reflect the official policy or positions of the United States Department of Veterans Affairs or the United States Government. No conflicts of interest to disclose.