

INTRODUCTION
Ehlers-Danlos Syndrome (EDS) is a heterogenous group of connective tissue disorders characterized by joint hypermobility, skin hyperextensibility, and tissue fragility. Of the five primary subtypes, hypermobility type EDS (hEDS) is the most common but also the most challenging to diagnose due to its lack of a definitive genetic marker. Research shows hEDS is genetically autosomal dominant in nature, although the exact genetic etiology is unknown.1 hEDS clinically presents as generalized joint hypermobility, related musculoskeletal conditions, and soft tissue fragility.2
For clinical diagnosis of hEDS, the 2017 International Classification of Ehlers-Danlos Syndrome created major and minor criteria that must be present. To clinically diagnose hEDS, generalized joint hypermobility through the Beighton Score, systemic manifestations of a more generalized connective tissue disorder, positive family history with one or more first degree relatives, musculoskeletal complications, absence of skin fragility, and exclusion of other heritable or acquired connective tissues.2 Due to its systemic manifestations, this disorder can be debilitating and often impairs the quality of life of the person.2,3
Treatment for hEDS requires a multidisciplinary approach focusing on prevention of progression and complications. The inclusion of neurologists, behavioral psychologists, and orthopedists are appropriate providers for comanaging patients with hEDS. Physical therapy can be beneficial in improving mobility and strengthening periarticular muscles. In many cases, management may also include anti-inflammatory drugs, acetaminophen, and/or serotonin and norepinephrine reuptake inhibitors to assist in pain management.3 Chiropractic has been introduced within the multimodal approach, but further research is needed to investigate its impact for patients with hEDS.4 A 2024 case report on a 24-year-old hEDS patient found that chiropractic treatment, combined with exercise and manual pressure release, provided short-term symptom relief. However, the patient reported symptoms returning within 2-3 days after each session. This suggests chiropractic care can help manage symptoms in hEDS patients and highlights the need for further discussion about its role in treatment.5 The goal of this case report is to describe the case management of a patient with hEDS under chiropractic care.
CASE REPORT
History
A 47-year-old female with a 5-year history of chronic neck and low back pain with radiation into the right buttock sought chiropractic care. Her symptoms first started in 2011 with severe low back pain that affected her daily tasks, sleep, and emotional health. In addition to her chronic pain, the patient also reported being diagnosed with anxiety, irritable bowel syndrome, hypertension, and arthritis. The Patient also reported having a history of frequent migraine headaches and reported a family history of her mother having an autoimmune condition.
Due to the severity of pain, an L5-S1 discectomy was performed in 2011 after the diagnosis of a herniated disc. This provided temporary relief of low back pain, but did not provide relief for her neck pain. Over the next 6 years, the patient managed many of her symptoms with her primary care provider as she was experiencing systemic symptoms associated with hEDS such as joint instability, irritable bowel syndrome, hypertension, and anxiety. In 2017, the patient underwent additional evaluation and was diagnosed with hEDS.
Between 2017 and 2024, the patient sought care from a physical therapist, primary care provider, and occasional chiropractic care consisting of gentle, low-force techniques such as instrumented assisted, manual, and drop techniques. The patient reported she had symptom relief through each chiropractic session, but results were temporary, and she would return for treatment when her symptoms returned. Due to joint instability because of hEDS, she underwent left ankle reconstructive surgery in August of 2022 and right knee reconstruction in May of 2022. However, in April of 2023, she had to undergo a second right knee surgery due to joint instability. Over time her low back pain and neck pain progressively worsened, and she was experiencing lumbar pain with bending, turning, and standing which in turn affected her work and led to a lack of quality sleep. This led to her seeking chiropractic care consistently in May of 2024. Using a Quadruple Visual Analog Scale (QVAS), with 0 being no pain at all and 10 being the worst pain imaginable, the patient reported a 4 at rest and a 6 with activity. Clinical assessment outcome tools, the Neck Disability Index and Oswestry Low Back Pain Questionnaire, were used and scored 21/50 and 18/50, respectively.
Physical Examination
The patient appeared to be in no acute distress and her vitals included a temperature of 98.2 °F and blood pressure of 122/74. She was 70 inches tall and weighed 185 pounds with a BMI index of 26.54.
During examination, the Beighton Scale was performed to assess hypermobility. Scoring is based on the following criteria: passive dorsiflexion of the 5th finger beyond 90°, passive flexion of the thumb to forearm, hyperextension of the elbow beyond 10°, hyperextension of the knee beyond 10°, and forward trunk flexion with knees fully extended and palms resting on the floor. Each test is scored as one if unilateral or two if bilateral.2 The patient scored an 8/9 using the Beighton Scoring system for hypermobility. This is due to the patient not being able to fully forward flex the trunk with knees fully extended and palms resting on the floor because to pain. Cervical range of motion was performed, and she reported pain in all ranges of motion. Active cervical flexion was measured at 60°/70°, extension 50°/70°, left lateral flexion 30°/45°, right lateral flexion 20°/45°, left rotation 70°/90°, and right rotation 60°/90°. Sensory testing of the dermatomes C4 through T1 was normal. Muscle strength testing of bilateral bicep brachii, triceps, wrist extensors, wrist flexors, finger extensors, finger flexors, finger adductions, and finger abduction were all 5/5 indicating normal function of the muscles. Deep tendon reflexes of bilateral bicep brachii, triceps, and brachioradialis were graded a +2. Her active lumbar flexion was measured at 70°/70°, extension 20°/30°, left lateral flexion 25°/25°, right lateral flexion 25°/25°, left rotation 30°/30°, and right rotation 30°/30°. The patient reported pain upon lumbar extension. Neurological findings indicated decreased sensation along the L4 and L5 dermatomes most likely due to post-surgical complications after her right knee and left ankle reconstructive surgeries.
Orthopedic testing resulted in a positive Shoulder Depression test for bilateral cervical pain. Soto Hall test produced sharp pain down the cervical spine upon cervical flexion. Cervical Distraction test was negative and provided no relief. Maximal Foraminal Compression test was negative bilaterally. Kemp’s test produced localized low back pain bilaterally. Slump, Yeoman’s, Hibb’s, and Ely’s tests were all negative for sacroiliac (SI) pain or reproduction of low back pain. Valsalva’s test was negative.
Chiropractic Examination
During posture assessment the patient presented with anterior head carriage. During palpation assessment bilateral hypertonicity of the trapezius, cervical, thoracic, and lumbar paraspinals was identified. Right pelvic internal rotation listing was found associated with decreased SI fluid motion. The L2 segment had decreased left rotation, T3 and T8 segments had decreased flexion and right rotation, and C2 had decreased flexion and left rotation.
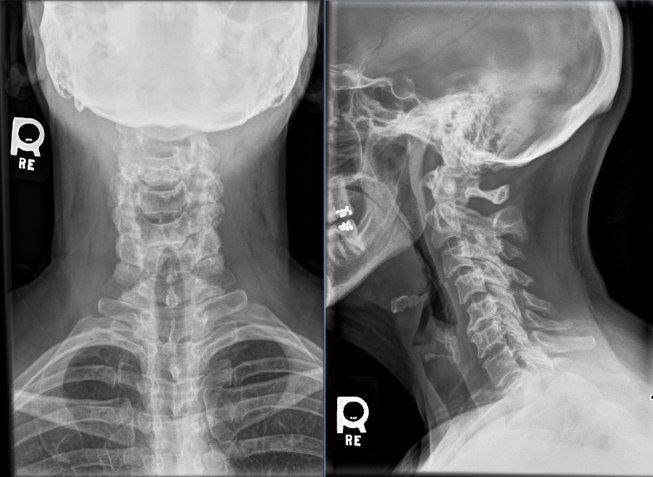
Prior to adjustment, cervical and lumbar radiographs were performed. These images can be seen in figures 1-3. Cervical spinal canal narrowing was predominant at C5-C6 and to a lesser extent at C2-C3, C3-C4, C4-C5, and C6-C7 with adjacent endplate osteophytosis. Retrolisthesis was identified at C5. Corresponding right uncinate hypertrophy was predominate at C4 and C6. Additionally, moderate zygapophyseal joint subchondral sclerosis with joint margin osteophytosis on the left of C2-C6 and right of C3-C7 was present.These findings indicated mild cervical kyphosis, cervical disc degeneration of C5-C6 and to a lesser extent C2-C3, C3-C4, C4-C5, and C6-C7, predominate uncinate hypertrophy and facet arthropathy, and grade I spondylolisthesis of C3 and to a lesser extent C2 and C4.
Lumbar spine radiographs showed disc narrowing at L5-S1 with a disc vacuum phenomenon, subchondral sclerosis, and joint margin osteophytosis. This is consistent with the partial laminectomy surgery the patient reported. Lower thoracic and lumbar spine generalized minor disc narrowing and endplate osteophytosis was identified. Zygapophyseal joints at L4 through S1 had mild subchondral sclerosis and joint margin osteophytosis. These findings indicated a left lateral thoracolumbar curve and generalized lower thoracic and lumbar spine degenerative disc disease most predominant at L5-S1.



Management
The initial treatment plan consisted of high-velocity, low-amplitude (HVLA) adjustments. She received care once a week for 6 weeks, once every 2 weeks for 6 weeks, then came once a month for the last month of care, totaling 4 months of care. She received adjustments with a Thompson drop table in the pelvic region. This is where the table drops down as the thrust is delivered to decrease forces applied. Within the thoracic region, double thenar diversified technique was delivered. This is when the doctor places both thenars on the transverse processes in the thoracic spine. Within the cervical region, instrument assisted adjusting was used to reduce rotational forces. The patient tolerated the adjustments well and reported improvement with low back and neck pain.
Outcomes
After her treatment plan of 4 months, the patient’s Neck Disability Index score went from 21/50 to 17/50 and her Oswestry Low Back Questionnaire score went from 18/50 to 11/50. Her numeric pain scale rating decreased from a 4/10 at rest to a 1/10 and her pain with activity decreased from a 6/10 to a 3/10. After every visit, the patient reported pain relief and stated she was able to be pain free for longer periods of time.
DISCUSSION
Hypermobile Ehlers-Danlos Syndrome is a complex and multifaceted condition that affects connective tissues throughout the body. It is characterized by joint hypermobility, frequent injuries, and chronic pain, along with systemic manifestations such as fatigue, dysautonomia, and gastrointestinal symptoms.2 This case of a 47-year-old woman with hEDS highlights not only the challenges of managing the condition but also the critical role of patient adherence to a care plan. She previously visited a chiropractor infrequently during the years before she came into our clinic but did not stick to a patient care plan and did not see the same results.
This case report is one of the few describing the results of chiropractic care for a patient with hEDS in conjunction with secondary systemic disorders. The patient’s recurrent joint fixations , chronic pain, fatigue, and anxiety illustrate the profound impact of hEDS on daily life. These symptoms can feel overwhelming, often leading to frustration and a sense of hopelessness. Effective management of hEDS requires a comprehensive care plan, typically including physical therapy, lifestyle adjustments, pain management strategies, and, in some cases, surgical intervention. Chiropractic management is not commonly included in “typical” care plans due to limited research.6 However, the outcomes from this case report suggest that chiropractic care may offer benefits for pain and disability as evidenced by the patient’s improvements in both Neck Disability Index and Low Back Oswestry Questionnaire and Oswestry scores as well as in the numeric pain scale.
Chiropractic care has been shown to reduce pain and disability in similar cases, including patients with EDS.4,6 In one instance, a patient showed significant improvement in pain and disability through the use of manually assisted techniques, such as the Activator method, combined with stabilization and corrective exercises.6 Notably, previous cases also reported a reduction in the use of anti-inflammatory medications when chiropractic care was integrated into the treatment plan.6 In this case report, medication usage was not monitored, making it unclear whether the observed pain reduction was solely due to chiropractic care or influenced by concurrent medication use. However, she used anti-inflammatory medications in the past and still had pain, thus one may conclude that chiropractic care had some impact on reducing pain and disability levels. In future assessments, tracking medication usage would be a valuable variable to measure, as many EDS patients rely on pain medications.1,3
An additional study in the literature also explored chiropractic care for patients with hEDS where a 22-year-old female with severe neck and low back pain sought care. She also had headaches and bilateral hand pain with stiffness. The patient was treated with a 21-month care plan in which she received low force joint manipulation in addition to soft tissue therapy that included Graston Technique most often but also included manual myofascial release and post-isometric relaxation technique. After her treatment plan, her Neck Disability Index and Oswestry Low Back Questionnaire showed decreases in disability and pain.4 This study shows similar results to our study but has the addition of soft tissue therapy. Future studies may wish to explore differences between the two treatment options and if one has a greater effect or if they work best in conjunction with each other.
The psychological and emotional aspects of hEDS also play a role in adherence. Chronic pain, social isolation, and the invisible nature of the condition can lead to feelings of frustration or mistrust toward the healthcare system.3,7 Addressing these barriers requires a patient-centered approach that emphasizes open communication, shared decision-making, and realistic goal setting. A pilot study involving 12 women with hEDS demonstrated that a combination of physical therapy, cognitive-behavioral therapy, group discussions, and physical training—alongside three months of home exercises—resulted in significant improvements in daily activity performance, increased muscle strength, reduced kinesiophobia, and decreased self-perceived pain.8 While these findings suggest potential benefits of a multimodal approach, the role of chiropractic care in this context remains unclear, as no evidence of its effectiveness was noted in the study.8 Furthermore, research on this type of comprehensive intervention for hEDS patients is still limited, underscoring the need for further investigation. However, two case reports have shown that chiropractic treatment in addition to daily home exercise programs including postural exercises can result in positive structural changes in cervical curve and Cobb’s angle as well as improvement in chronic symptoms and overall function.6
Effective Treatment requires an individualized, empathetic approach. Recognizing that patients may feel overwhelmed, it is vital providers focus on setting achievable goals, offering consistent support, and involving patients in the development of their care plans. Regular check-ins, access to mental health resources, and education on the importance of long-term management can empower patients to stay engaged in their care.7 In addition to carefully crafted treatment plans with multiple providers, addressing the psychological aspect of chronic conditions like hEDS may help patients’ mental health along with their physical health.
Limitations
This case study focuses on a single patient, so the findings cannot be generalized. Additionally, there is limited research on the effects of chiropractic care for hypermobile-type Ehlers-Danlos Syndrome, making it difficult to fully support our conclusions. Therefore, further research is needed to better understand the impact of this treatment approach on a broader population.
CONCLUSION
This case report describes the management of a patient with hypermobility-type Ehlers Danlos Syndrome. Using multiple types of chiropractic techniques including Thompson, instrument assisted, and diversified techniques provided improvement in the patient’s pain and quality of life. Chiropractic has a role in management of hEDS, but may be best when used as a multimodal approach to patient care.
Consent
The patient provided written informed consent.