











INTRODUCTION
TARS or Thrombocytopenia Absent Radius Syndrome is a rare syndrome, which was first reported by Shaw and Oliver in 1959.1 This syndrome is characterized by thrombocytopenia, the absence of both radii and the presence of thumbs. Because of the absence of the brachioradialis muscles, but presence of the brachiocarpalis muscles,2 there are deformities of the elbows and the wrists. The attachment sites for the new muscle (brachiocarpalis) are on the anterolateral aspect of the proximal humerus near the deltoid muscle and on the carpus (wrist) (See Figure 1).

Most of those with TARS have short stature, as noted in dwarfism, and there is often scoliosis (See Figure 2).

We discuss the case of a 47-year-old Caucasian female cadaver with TARS examined in the anatomy laboratory at a chiropractic college. The term achondroplasia is a specific genetic type of dwarfism, while dwarfism is a term for short stature. People that have dwarfism or achondroplasia usually have normal intelligence and a normal life expectancy. Those with dwarfism or achondroplasia have shorter than normal arms and legs and larger than normal head. Hypochondroplasia, which is a mild incomplete form of achondroplasia, is due to a mutation in fibroblast growth factor receptor 3 (FGFA3) gene, which does not allow for proper skeletal development. People with hypochondroplasia have short stature, short limbs, broad hands and feet, large head, and possibly other abnormalities, including bowing of legs, swaying of lower back, and limited range of movement of elbows.
Chiropractic treatment for individuals with dwarfism/achondroplasia is not well documented in the literature, but the use of interventions, such as manual therapy, massage therapy, aquatic therapy, and combination of cervical traction with compression for such individuals and those with TARS may be beneficial for their quality of life. Consequently, we conducted a narrative review to identify possible benefits of chiropractic care in improving the quality of life in these patients.
DISCUSSION
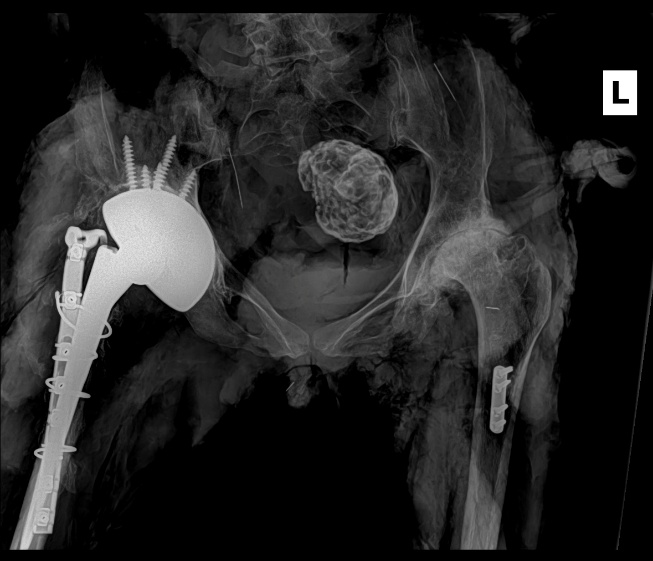
Numerous cadavers have been dissected throughout the years at our chiropractic institution to enable students to learn about normal and even abnormal anatomy to further their medical education. A cadaver of a 47-year-old Caucasian female with a cause of death of thrombocytopenia absent radius syndrome (TARS) sparked our interest in learning more about this syndrome and how chiropractic modalities may be of benefit in helping in daily activities in such patients. There were several interesting findings noted as the complete dissection of the cadaver was performed. We decided to get x-rays (after dissection) of the cadaver for documentation of the different abnormalities and surgical procedures. Radiographic findings noted in this cadaveric case demonstrate the absence of radii. In addition, post-mortem (post-dissection) radiographs showed a total right hip replacement, a total left knee replacement, and surgical repair with plate and screw placement of the left femur (See Figures 3a and 3b).3


These surgical repairs were most likely due to osteoarthritic changes in the bone related to the disease. To support the reasoning for the repairs being due to probable arthritic changes, there were gross findings of arthritic changes of the right knee and hypoplasia of the patella, a finding seen with TARS (See Figure 4).

Clinodactyly, which is often seen in cases of Down syndrome, plus opposition of the thumbs were findings of the cadaveric TARS case (See Figures 5a and 5b).


Abnormal positioning of the ulna at the carpus and shortened ulna were also identified in this case (See Figure 6).

The measurement of the left ulna was 10.3 centimeters in length. Per Srivastava et al. in 2013, normal ulna length is 25.33 +/- 1.88 centimeters.4 Specifically for females, the normal ulna length is 22.70 +/- 1.17 centimeters.4 The ulna length in our TARS case was less than half usual normal length for females.
Other non-bony abnormalities but interesting and important findings in this TARS cadaveric case were cardiac and genitourinary anomalies, including a left sided brachiocephalic trunk (See Figure 7), a smaller right common carotid artery compared to the left (See Figure 8), a right sided aortic arch (See Figure 9), apparent status-post surgical repair of Tetralogy of Fallot, and polycystic horseshoe kidney (an extremely rare, combined finding with about 20 documented cases in the literature) (See Figure 10), and other findings: hepatosplenomegaly, subhepatic cecum (See Figure 11), a small rectosigmoid polyp, hemorrhage and necrosis of the right substantia nigra and cerebral peduncle, and hemorrhage of right basis pontis and medulla. The hemorrhages in the brainstem were most likely a complication of the thrombocytopenia associated with this syndrome. Intracranial hemorrhages are a major cause of mortality in TARS. Also, there was torsion of the right uterine tube with a calcified adnexal mass (fibrous tumor).





We conducted a literature search over a 9-month period, from May 2024 to February 2025. Our primary focus was on peer-reviewed literature published between 2009 and 2024. However, in the interest of historical context and completeness, we also included two secondary sources predating this range—specifically, one article from 2003 and another from 1959—that were relevant to our research scope.
To identify relevant literature, we employed a range of targeted search terms and phrases, including achondroplasia, dwarfism, hypochondroplasia, and combinations thereof with terms such as TARS, chiropractic manipulative therapy, aquatic therapy, adjustments for dwarfism, surgery, manual therapy, massage therapy, ultrasound, and dwarfism treatment. These search strategies were applied across major academic databases and repositories.
Both authors independently reviewed the collected literature, selecting studies that explicitly documented treatment modalities applied to individuals with achondroplasia. We excluded sources that lacked specific outcome data or did not present clearly defined results related to treatment efficacy. Our inclusion criteria were designed to ensure that only clinically relevant and data-supported interventions were analyzed in the final synthesis.
Our search terms yielded a total of 20 articles, of which 14 were retained for inclusion based on relevance to our research criteria. Interventions identified in the literature for individuals with dwarfism or achondroplasia include a variety of conservative and rehabilitative therapies, such as manual therapy, massage therapy, aquatic therapy, and a combination of cervical traction with cervical compression.5–7
Further treatment modalities described in the literature include high-velocity, low-amplitude (HVLA) thrust manipulations applied to the lumbar spine and extremities, as well as sacro-occipital technique (SOT), which is characterized by low-velocity low-force mobilization intended to gently influence craniosacral and pelvic dynamics.5,7 These techniques have been explored as part of multimodal chiropractic and rehabilitative approaches aimed at improving musculoskeletal alignment and reducing discomfort associated with skeletal dysplasia.
Spinal curvature disorders, which are frequently observed in individuals with achondroplasia, have shown responsiveness to spinal manipulation therapy.8Additionally, structured exercise programs and physical rehabilitation have been shown to improve functional mobility in children with achondroplasia, particularly post-surgically or when managing joint-related limitations.8,9 Particularly, aquatic therapy is highlighted as a valuable modality due to its low-impact environment and capacity to support joint movement without excessive mechanical stress.6
Outcomes
Improvement in mobility and reduction in pain were seen across multiple studies for patients with dwarfism, achondroplasia, or hypochondroplasia.10 One paper described a 63-year-old woman with hypochondroplasia experienced restoration of hip mobility and improved gait biomechanics following a course of myofascial massage therapy.5 Similar trials conducted demonstrated a significant increase in sagittal cervical lordosis using a combination of cervical traction and cervical compression in patients undergoing spinal care.7
A 2018 case study reported by the ALPE Foundation described improvements in motor skill development, muscle tone, and joint mobility in a 20-month-old infant with achondroplasia following an aquatic therapy regimen.6 In addition to these functional improvements, some studies suggested an association between these interventions and increased overall survival outcomes.5,10
While no studies specifically documented chiropractic interventions in patients with thrombocytopenia-absent radius syndrome (TARS), the shared musculoskeletal abnormalities between TARS and conditions like achondroplasia suggest that similar therapeutic benefits might be possible.1,10,11 Given these overlaps, conservative therapies such as chiropractic care and physical rehabilitation may warrant further investigation in TARS populations.
After 14.6 weeks of extension-compression 2-way cervical traction combined with spinal manipulation, participants in a controlled clinical trial demonstrated a significant increase in sagittal cervical lordosis.7 Post-treatment outcomes—following 38 visits over a 14.6-week period—were compared to those from a group that received only 3 weeks of treatment. The longer-duration group exhibited notable improvements in both global and segmental cervical alignment. Additional findings included a reduction of anterior head weight-bearing by 11 mm, an increase in Cobb angles averaging 13–14°, and a mean improvement of 17.9° in the angle of intersection of posterior tangents between C2 and C7.7
Manual therapy also produced functional improvements in patients with hypochondroplasia. One case described a 63-year-old female librarian, standing 4’4" (132 cm), who was the only known family member with hypochondroplasia.5 Diagnosed with this bone growth disorder—characterized by defective conversion of cartilage into bone due to point mutations in the fibroblast growth factor receptor, the same gene implicated in achondroplasia—the patient experienced restoration of hip mobility and enhanced gait biomechanics following myofascial massage therapy.5
Our literature review also highlighted work by the ALPE Achondroplasia Foundation exploring the connection between achondroplasia and aquatic therapy.6 In a 2018 case study, a 20-month-old female demonstrated notable gains in motor skill development, muscle tone, and joint mobility. By 25 months of age, she was meeting the motor milestones of a 21-month-old, a marked improvement from her 15-month equivalent performance at the study’s start. Additional benefits observed included improved abdominal strength, enhanced balance and coordination, lengthening and strengthening of back musculature, and increased lung capacity. Follow-up by Dr. Carmen Barreal emphasized that aquatic therapy may help infants aged 12–14 months with achondroplasia improve motor expressivity, balance, and limb coordination.6
A thorough musculoskeletal assessment of segmental spinal postures and rehabilitation concentrating on promoting spinal and hip flexibility is needed in children with achondroplasia8,12; therefore, a complete chiropractic examination is beneficial in these children. Myofascial massage therapy does help reduce adhesions and increase circulation to help restore lower extremity range of movement by increasing dorsiflexion and plantar flexion, and this type of therapy has shown to cause an increase in average distance walking before needing rest in a 63-year-old woman with hypochondroplasia.5 In a nonrandomized clinical control trial by Harrison et al., they found that chiropractic biophysics technique of extension-compression 2-way cervical traction combined with spinal manipulation decreased the intensity of chronic neck pain and improved cervical lordosis with evidence of increased segmental and global cervical alignment after 38 visits over 14.6 weeks.7 Per Dr. Carmen Barreal regarding aquatic therapy in infants between 12-14 months of age with achondroplasia, there was improvement of motor expressivity, balance, and limb strength. Manual treatment like gentle joint mobilization, soft tissue techniques, and postural correction exercises may also be of benefit for those who have dwarfism/achondroplasia.
Limitations
One of the limitations of this paper is that literature on chiropractic treatment modalities for patients with thrombocytopenia absent radius syndrome is essentially non-existent. Also, the information about those with dwarfism undergoing chiropractic treatment is small, so therefore further research into such treatment modalities would help us to better understand this disease process and other such diseases.
Chiropractic care does improve quality of life in those with dwarfism and achondroplasia and possibly also those with TARS. The main issues related to the quality of life in these patients are: 1) pain, 2) compromised physical function, and 3) impaired overall functional health status due to lumbosacral spine issues. About 2/3 of adults with achondroplasia have chronic pain, which is higher than that noted in the general population. Physical function is compromised due to limited walking endurance and loss of ability to do daily living activities (e.g. bathing and toileting) by themselves. Decline in functional health status often occurs in the 4th and 5th decades of life.
In summary, additional investigation and research are required to determine the importance of chiropractic modalities in treating those with achondroplasia/dwarfism and more specifically TARS, considering the musculoskeletal abnormalities in the cadaveric case we saw in the anatomy laboratory at our institution. Multidisciplinary care is a must for those with achondroplasia/dwarfism and TARS.