


INTRODUCTION
Vertebral compression fracture (VCF) is the most common fragility fracture reported in the literature with approximately 1 to 1.5 million occurrences annually in the United States.1 The thoracolumbar junction between T12-L2 comprises 60-75% of fracture sites with another 30% at the L2-L5 region.1 Although is the most common consideration for VCFs, approximately 30% of VCF may occur with an aging population at higher risk of low energy fragility fractures.1 The patient also presented with psoriasis, which has an increased risk of osteoporosis and fracture by 7-26%, particularly as the severity of psoriatic lesions progresses, as compared to the general population.2 Osteoporosis is one of the most common and costly diseases with one in two women and one in five men experiencing an osteoporotic fracture after the age of 50.2 Osteoporotic fractures can result in pain, immobility, loss of independence, placement in a long-term care facility and can lead to depression, isolation and other complicating health comorbidities.2 A study of approximately 159,000 patients with psoriasis found increased prevalence of additional risk factors for osteoporosis and fracture including diabetes, alcohol abuse, smoking, depression, antidepressant use, corticosteroids, methotrexate, and cyclosporine.2
CASE REPORT
A 61-year-old male sought care at a chiropractic college outpatient outreach clinic for evaluation and care of neck pain and stiffness upon right rotation for several days after “sleeping funny” and low back pain and stiffness at the L5 level for approximately 3 months. He denied injury and radiculopathy and noted reduced ability to walk long distances and sleep. He revealed a history of episodic low back pain of varying intensities over decades of time with inconsistent impact on Activities of Daily Living (ADL). He reported daily use of an ACE inhibitor and blood thinner. The patient denied any pre-existing conditions, particularly prior vertebral compression fracture, low bone density, psoriasis or addiction issues of any kind. Family history was reported as non-contributory. All exam findings were negative for red flags or other contributory findings.
Radiographic examination of the cervical and lumbar spine identified adequate bone density, (decreased bone density cannot be identified on plain radiographs until more than 30-50% of bone mass has been lost3), cervical, lower thoracic and lumbar disc degeneration, and cervical and lumbar zygapophyseal osteoarthrosis.
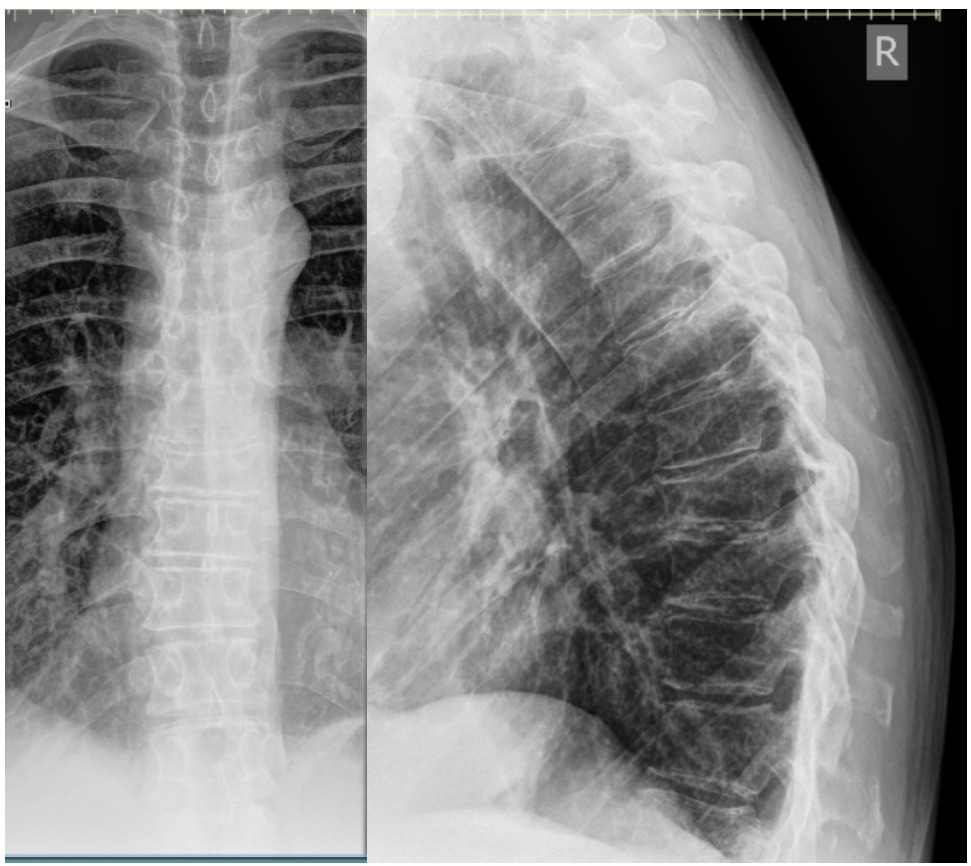
The patient was treated with Thompson drops and reported improved range of motion with decreased pain and stiffness in both the cervical and lumbar regions within the first 3 treatment visits. Intermittent chiropractic treatment for minor complaints continued for approximately two years until the patient reported new onset of upper thoracic pain with occasional radiation of pain to the right arm intermittently with no injury. After 5 treatment visits over the course of 4 weeks with little improvement, radiograph examination of the thoracic spine was ordered.
Osteopenia, an old concave compression fracture deformity of the T9 superior endplate, and a well-corticated right T8 rib fracture with callus formation were seen. At this time the patient revealed that he was taking medication for Factor V Leiden, an inherited blood clotting disorder. Chiropractic care using Thompson drops continued and within an additional 4 weeks the thoracic pain resolved.
Approximately 10 weeks later the patient reported injury to the low back while carrying a large, heavy object and stepping down, resulting in moderate, non-radiating pain with both rest and activity. Radiographic examination of the lumbar spine revealed a compression fracture of the inferior aspect of L3 with step defect, possibly acute, and ununited left L2 and L3 transverse processes, age indeterminate. The patient was referred for DEXA bone density examination and cross-sectional imaging (CT) to further evaluate the extent of the L3 compression fracture.
Chiropractic care using Thompson drops in unaffected spinal regions continued for the next 5 weeks. After a 7-month absence from care, the patient returned reporting midline and centrally worsening non-radiating low back pain after a fall on his back and buttocks approximately 3-4 months prior in his bathroom. He was seen by his medical doctor prior to the treatment visit for this incident and had been referred to physical therapy. He denied head injury, fracture, loss of consciousness, saddle paresthesia or changes with bowel and bladder function. Radiographic examination of the lumbar spine demonstrated superior and inferior endplate fractures of the T12 vertebral body with 60% vertical loss of height not evident on previous examination. Osteoporosis was reported at this time. Examination with CT and MRI were recommended for further characterization of the T12 compression fracture due to the severity of radiographic presentation. The patient was referred to his primary care physician for co-management and the provider was contacted directly due to the loss of vertebral body height (see Table 1 for overview of progression of care).




The medical provider and patient agreed to co-management and health documentation was shared. It was discovered through medical office visit notes that the patient had previously reported to a local hospital system for a closed head injury after a fall while getting out of a car. He was hospitalized for four days and found to be hyponatremic, as attributed to a combination of diuretic and beer potomania with an elevated blood alcohol level. The CT of the brain was negative for intracranial hemorrhage, skull fracture or other pathology. Osteopenia was identified and attributed to use of warfarin for several years as documented in a 2008 DEXA scan. This information was unknown by the chiropractic physician prior to initiating care or at any point as care continued. Medical records also noted the patient typically drank two alcoholic beverages, (usually beer), several days per week with increased use on the weekends.
A known association between alcohol consumption and osteoporosis exists with a linear increased risk for fracture with higher alcohol consumption4. A rationale for the detrimental impact on bone health of excessive or consistent alcohol intake includes bone remodeling whereby bone formation is largely uncoupled with bone resorption4. Alcohol may impact bone microarchitecture which impacts cortical thickness and trabecular bone volume4. Hormone dysregulation by alcohol overconsumption may interfere with bone metabolism4. Nutrient absorption is also impacted by excessive alcohol consumption with malabsorption of calcium from the intestine leading to decreased levels of circulating serum calcium and thus calcium deficiency4.
DISCUSSION
Vertebral compression fracture (VCF) prevalence increases with age, reaching 40% incidence in the general population by age 805. While most patients with VCF are managed without hospitalization, vertebral compression fractures can cause severe physical limitations, chronic back pain, functional limitations, and significant disability5. Multiple adjacent vertebral fractures can lead to progressive kyphosis of the thoracic spine and other comorbidities, including decreased appetite resulting in poor nutrition and decreased pulmonary function5. This progressive decline in health and vitality contributes to levels of increased morbidity and mortality in patients with these fractures as compared to those in the general population5.
Symptoms of VCF may include sudden onset back pain, increased intensity of pain during standing or walking, pain that decreases when lying in a supine position, pain that increases during palpation over the affected area, and decreased spinal mobility due to pain5. Complications of VCF include consistent low-grade back pain, increasing thoracic kyphosis, and lumbar lordosis, impaired pulmonary function and respiratory capacity, a protuberant abdomen with early satiety and weight loss, accelerated bone density loss, deep vein thrombosis due to inactivity, and psychosocial components of low self-esteem with other emotional and social isolation5. These compression fractures can have a slow and insidious onset that may only initially present as low-grade back pain, possibly leading a clinician to avoid consideration of vertebral compression fracture in the absence of a trauma history. The realization that VCF can occur with little to no significant trauma is an important consideration when considering imaging examination to detect fractures.
After the second VCF was identified on radiographic examination of the lumbar spine, considerations into comorbidities were explored. This is when the patient revealed that he had Factor V Leiden. It is one of the most common hereditary hypercoagulability disorders that also causes hypofibrinolysis and the development of transient osteoporosis of the hip due to ischemic causes6.
Management options included improvement of bone density through food, supplementation, or pharmaceuticals. As an outreach patient enrolled in the hardship program providing no cost clinical care, the patient expressed concerns about access to nourishing foods supportive of bone health due to difficulty with transportation. In addition, he had concerns with the affordability of nutrient dense foods or supplementation associated with building bone health. These concerns are common in patients experiencing food insecurity, the condition of not having access to sufficient food or food of an adequate quality to meet one's basic needs. The USDA defines food insecurity as a lack of consistent access to enough food for every person in a household to live an active, healthy life. Food insecurity is associated with decreased nutrient intake and poor health with consequences of possible low bone mass, especially in children7. Bone is a living tissue with nutrient requirements for appropriate structural integrity7. Of the estimated 10.2 million people in the U.S. population 50 and older that suffer from osteoporosis, inadequate nutrition is a major risk factor8. Adequate levels of calcium and vitamin D through food or supplementation significantly reduces the risk of fractures by 15% and reduces risk of hip fractures specifically by 30%8. As of 2018 the United States Census Bureau reported that 11.8% of the U.S. population lived at or below the poverty line8. Low-income populations have been shown to be at risk for inadequate calcium and vitamin D intake8.
After the third VCF occurred, consideration for the impact of psoriasis on bone health was also researched. This diagnosis was discovered after review of notes from the medical physician. The patient presented to every appointment with long pants and long-sleeved shirts and did not report medication for psoriatic lesions. As an immune-mediated chronic inflammatory skin disease that impacts 2% of white populations, it has a visibility that can cause social stigmatization, pain, discomfort, psychological distress, and a reduced quality of life9. In this pathology, cytokine overactivity leads to keratinocyte hyperproliferation that creates thickened inflamed plaques that have a silvery scaley appearance9. It is theorized that the coverage of skin and avoidance of physical activity are contributing factors to bone density loss9. Metabolic syndrome can occur with extensive psoriasis9. Systemic T-cell activation also plays a key role in the development of a T-helper 1 type cytokine pattern with secretion of interleukin (IL)-2, IL-6, interferon (IFN) and tumor necrosis factor (TNF)9. IL-6, IFN and TNF are involved in bone metabolism regulation and the pathogenesis of osteoporosis9.
Office visit notes by the primary care physician also revealed that alcohol was involved in the recent trauma with a reported pattern of chronic alcohol use and possible abuse. There were no indicators during the numerous patient visits to the chiropractic office that alcohol may be a factor to consider. Once the patient was out of acute pain he ceased care.
Limitations
This report describes a single patient's clinical presentation, diagnostic evaluation, and management. Generalization of the content of this report to any other individual with a similar clinical presentation is to be avoided.
CONCLUSION
This case report describes the clinical presentation, radiographic findings, risk factors for and complications of vertebral compression fracture with multiple co-morbidities and emphasizes the importance of a thorough and consistent case investigation process that may unfold outside of the initial case intake process. However, no matter how thorough the case history interview may be or intake paperwork may be written, when a patient denies certain medical history or withholds critical information needed for care, that is outside of the control of the providing clinician. In this case, the patient was an alcoholic with multiple factors contributing to weaker bone and increased risk for fracture that in the least would have provided an opportunity for intervention efforts to help prevent the VCFs that did occur through patient education. For those of an outreach population that may have challenges with transportation to access medical care or nourishing food, additional intervention to make appropriate referrals and provide community resources may be necessary and imperative to improving quality of life and reducing risk of fracture, disability and morbidity.
CONSENT
Written informed consent was obtained from the patient for publication of this case report and any accompanying images.