
Introduction
Musculoskeletal disorders include a wide range of conditions affecting muscles, bones, joints, and connective tissues, and are among the most common health problems worldwide and a leading cause of disability. Low back pain is one of the most prevalent musculoskeletal disorders, affecting about 20% of adults in the United States and Europe, generating substantial economic burden.1,2 Chiropractors are healthcare professionals who specialize in the diagnosis and treatment of musculoskeletal disorders, particularly those affecting the spine, using manual manipulation techniques such as spinal adjustments to alleviate pain and improve function.3,4 Chronic low back and neck pain are frequent reasons for seeking chiropractic care, yet evidence is limited by a scarcity of large, high-quality randomized trials and the individualized nature of treatment.
Clinical trials investigating chiropractic care for patients experiencing spinal pain primarily focus on quantitative outcomes such as pain scales, ranges of motion, orthopedic tests, and changes in various questionnaires (e.g. Oswestry, Roland-Morris). Patient-reported outcome measures are essential because patients usually provide the best assessment of their own health status, but such data are not routinely collected in chiropractic practice. The Medical Outcomes Study 36-Item Short-Form Health Survey (SF-36) and its revision, SF-36v2 were developed as brief, generic self-reported measures usable across a wide range of ages and medical conditions.5–8 The SF-36v2 provides 8 scale scores and 2 summary scores (Physical Component Summary [PCS] and Mental Component Summary [MCS]) and has demonstrated good reliability and validity, including in populations with spinal disorders.5–9 There is a relative paucity of longitudinal studies in chiropractic settings that employ such broad, generic health-related quality-of-life instruments alongside traditional quantitative clinical outcomes, which motivated the choice of SF-36v2 in this study to monitor changes in both physical and mental health over time.
This study aimed to evaluate changes in health-related quality of life over three months in adult patients with low back and/or neck pain undergoing chiropractic care only in Italian private practices. The primary objective was to assess changes in SF-36v2 PCS and MCS scores from baseline to three months in this observational cohort.
Methods
Ethical Approval and Participating Chiropractors
This research was conducted in 37 Individual Chiropractic Private Practices in Italy and in accordance with the Declaration of Helsinki. The study protocol was approved by the University of Bari, Italy, Research Ethics Board (REB #: 1045). The study was also reviewed and approved by the Italian Chiropractic Association Ethics Committee and Scientific Committee. Thirty-seven licensed Italian chiropractors in private practice participated in the study in their individual practices throughout Italy.
Study Population
One hundred and sixty-three adult patients were divided into 81 adult male and 82 female patients aged 18-65 years old, presenting with neck pain and associated disorders or non-specific low back pain. Patients recruited in the study were patients who presented to individual Chiropractic practitioners in private practice between December 2023 and December 2024. All patients underwent a physical examination to confirm eligibility for chiropractic care and rule out obvious contraindications (spinal metastasis, severe osteoporosis, severe spinal stenosis, severe herniated discs with radiculopathy). Chiropractors informed eligible patients about the study objectives and invited them to participate; written informed consent was obtained from all participants.
Data Collection
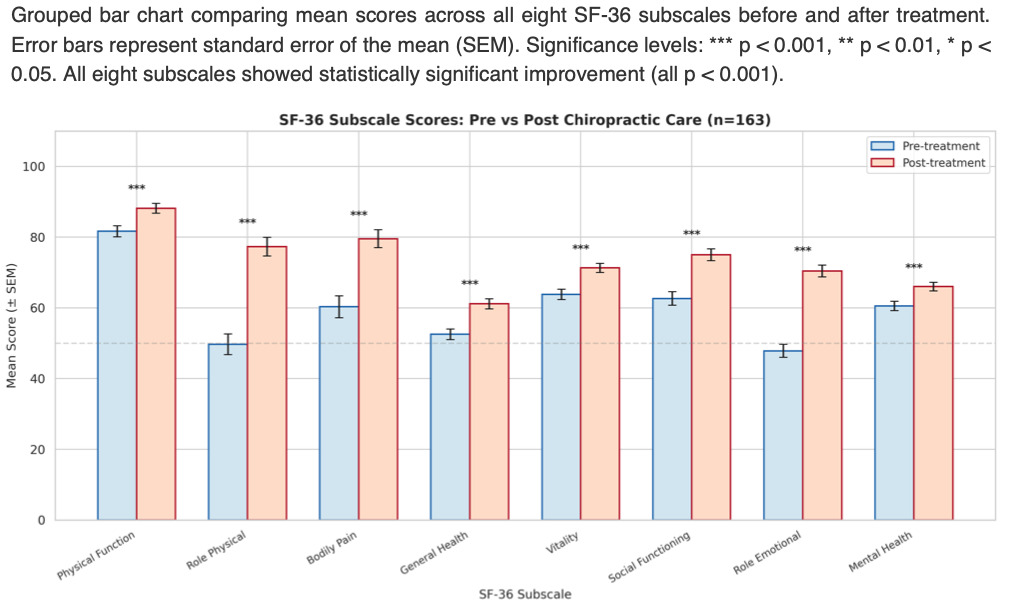
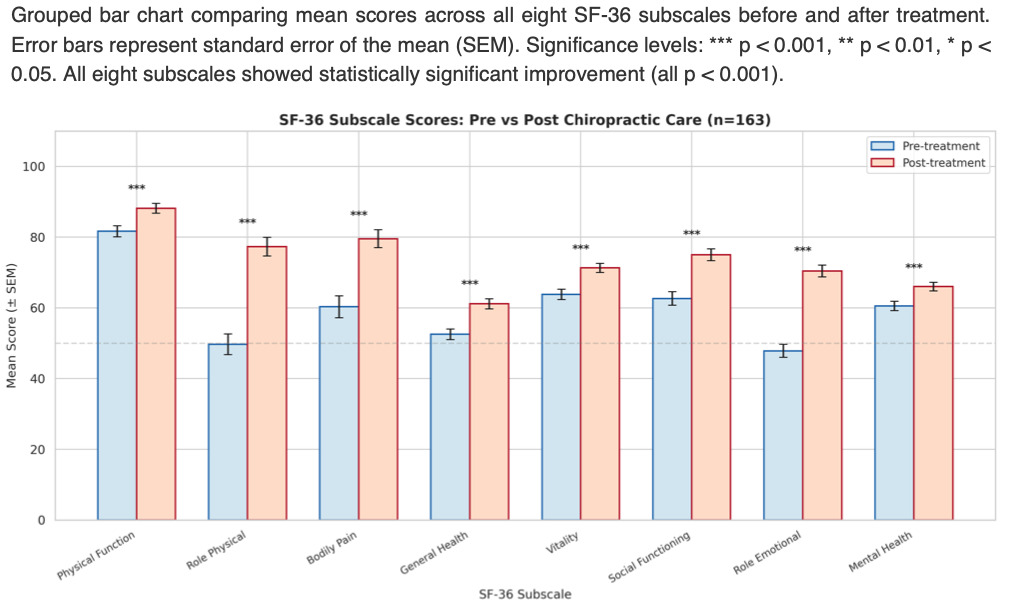
An electronic web-based SF-36v2 questionnaire was used to collect data. SF-36 consists of 36 items that are employed to calculate scores on 8 dimensions: Physical Functioning, Role Limitations due to Physical Health Problems, Bodily Pain, General Health, Vitality, Social Functioning, Role Limitations due to Emotional Problems, and Mental Health.5–8 The PCS and MCS scores are weighted summations of these 8 scales.8,9 Higher scores indicate better health status.
Patients completed the first questionnaire before beginning care, and then monthly for 3 consecutive months. The first month was considered acute care, followed by 2 months of maintenance care. An alpha level of p<0.05 was considered statistically significant for all measured variables.
Chiropractic Management
At each visit, patients received a full-spine chiropractic assessment, including sacroiliac joints, to identify dysfunction warranting adjustment. Clinical indicators included joint tenderness or pain on palpation, restricted intersegmental range of motion, asymmetric segmental muscle tension, skin and connective tissue changes, (These can include altered texture (e.g., bogginess), color changes (redness, paleness), vasomotor disorders (affecting blood flow), electro-resistance changes, or trophic changes), tissue thermal variation, and Derifield-Thompson leg-length inequality. Patients underwent full spine chiropractic adjustments only; no other modalities or physical therapy was used.
Patients were initially seen 1-2 times per week for the first month, then monthly. Chiropractic manual or instrument-assisted adjustments were administered using diversified, Activator, Thompson, sacro-occipital technique (SOT), upper cervical, or Gonstead techniques, all at the chiropractor’s discretion. No physical therapy modalities were used as adjunctive therapy; patients underwent chiropractic adjustments only for the duration of 3 months.
Statistical Analysis
Data were analyzed using R software (version 4.3.1). A non-parametric Wilcoxon signed-rank test was used to compare paired PCS and MCS scores before and after 3 months of chiropractic care. Statistical significance was defined as p<0.05.
Results
One hundred and sixty-three patients completed all three SF-36v2 questionnaires over the three months. Pre and Post treatment result show improvement in all parameters (Fig 1). The statistical analysis demonstrated highly statistically significant (p<0.001) changes for both physical and mental components. Among participants, the mean PCS score increased from 44.7±10.5 at baseline to 51.0±9.7 at 3 months. The mean MCS score increased from 41.8±7.7 to 46.0±7.0 over the same period (Fig. 2). Wilcoxon signed-rank tests confirmed that changes in both PCS and MCS were highly significant (p<0.001).

Discussion
In this cohort of Italian adults with non-specific low back and/or neck pain, 3 months of chiropractic care were associated with statistically significant improvements in both physical and mental health-related quality of life. The magnitude of change (approximately 6.3 points for PCS and 4.2 points for MCS) suggests clinically meaningful improvement, although minimally important differences for SF-36v2 can vary by population and condition.
Possible Mechanisms
The improvements observed may relate to changes in pain and disability, mediated by complex biochemical and neurophysiological processes. Pro-inflammatory cytokines (IL-1β, IL-6, TNF-α) contribute to acute and chronic pain and neuropathic hyperalgesia.10,11 Anti-inflammatory cytokines such as IL-10 act as inhibitors of pro-inflammatory cytokines and are reduced in chronic diffuse pain. Chiropractic care and spinal manipulative therapy (SMT) have been linked to modulation of inflammatory mediators12–14
Other proposed mechanisms include modulation of the endocannabinoid system, which may mediate analgesic and mood effects of joint and spinal manipulation, and neuroplastic changes in central nervous system processing. SMT has been associated with altered somatosensory activation, sensorimotor integration, motor unit behaviour, and corticospinal excitability, potentially improving motor control and reducing recurrent neuromusculoskeletal pain.15–18 Mechanotransduction at the cellular level—where cells sense mechanical cues and translate them into biochemical signalling, in part through cytoskeletal structures—may also be involved in the response to spinal loading.
Improvements in MCS may be partly explained by reduced pain and disability and the known associations between chronic musculoskeletal pain, depression, anxiety, social functioning, and interoceptive awareness.19–22 Regulation of the autonomic nervous system and endocannabinoid system has also been suggested as a mechanism by which chiropractic care might improve mood and related symptoms.23,24
These mechanistic explanations are speculative in the context of this study, as no biochemical or neurophysiological measures were collected; they are based on prior research and provide possible pathways linking chiropractic care to changes in pain and quality of life. In our future study, we will be including blood biochemical parameters during Chiropractic acute care and follow-up maintenance care. These will include saliva Cytokines and Endocannabinoid levels and their precursors.
Limitations
Key limitations include:
Recruitment from Italian chiropractic practices, which may limit generalizability to other settings.
Exclusive reliance on self-reported SF-36v2; no objective clinical measures or biomarkers were obtained
Analysis focused on baseline versus three-month outcomes without detailed exploration of trajectories or subgroup effects
Nevertheless, the study demonstrates the feasibility of collecting standardized patient-reported outcomes in routine chiropractic practice and suggests that patients with spinal musculoskeletal pain report substantial improvements in physical and mental health over three months of chiropractic care.
Conclusion
In this 3-month longitudinal observational study of 163 adults with low back and/or neck pain receiving chiropractic care in Italian practices, statistically significant improvements in SF-36v2 Physical and Mental Component Summary scores were observed. These findings suggest that chiropractic care may be associated with improved health-related quality of life in patients with spinal musculoskeletal pain. Because of the uncontrolled design and potential confounding, causal conclusions cannot be drawn. Future controlled studies with longer follow-up and inclusion of mechanistic measures are needed to confirm these associations and clarify underlying biological and neurophysiological mechanisms.