Introduction
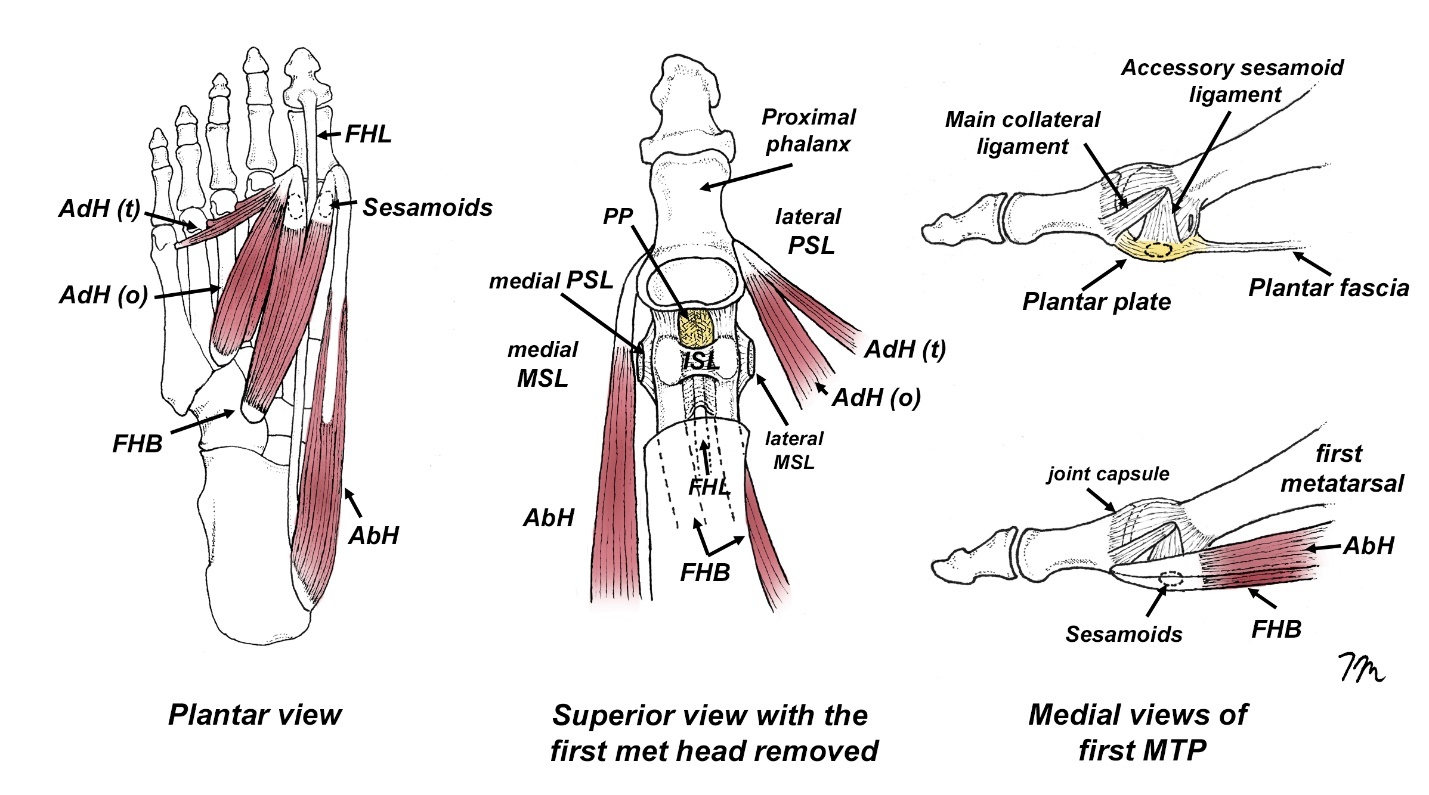
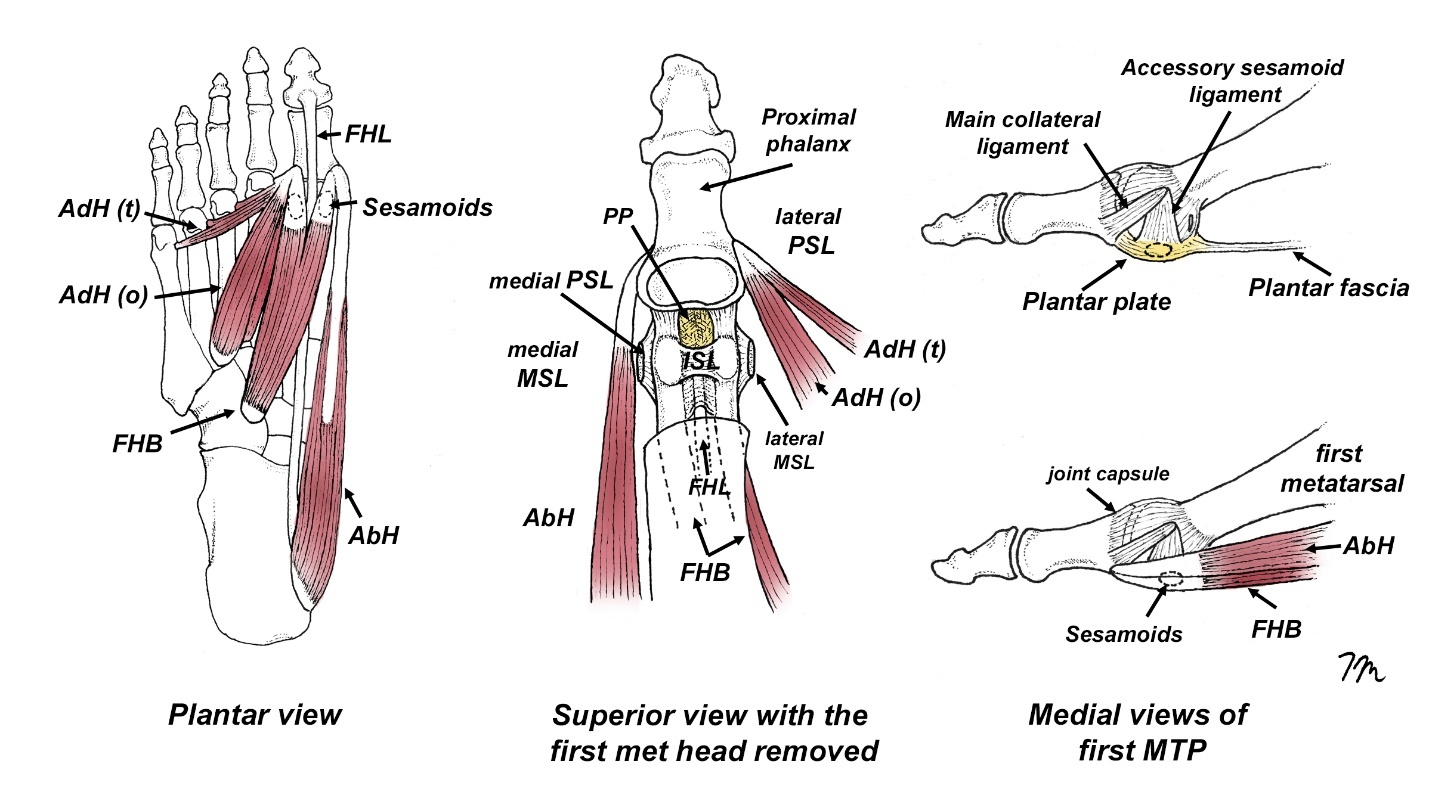
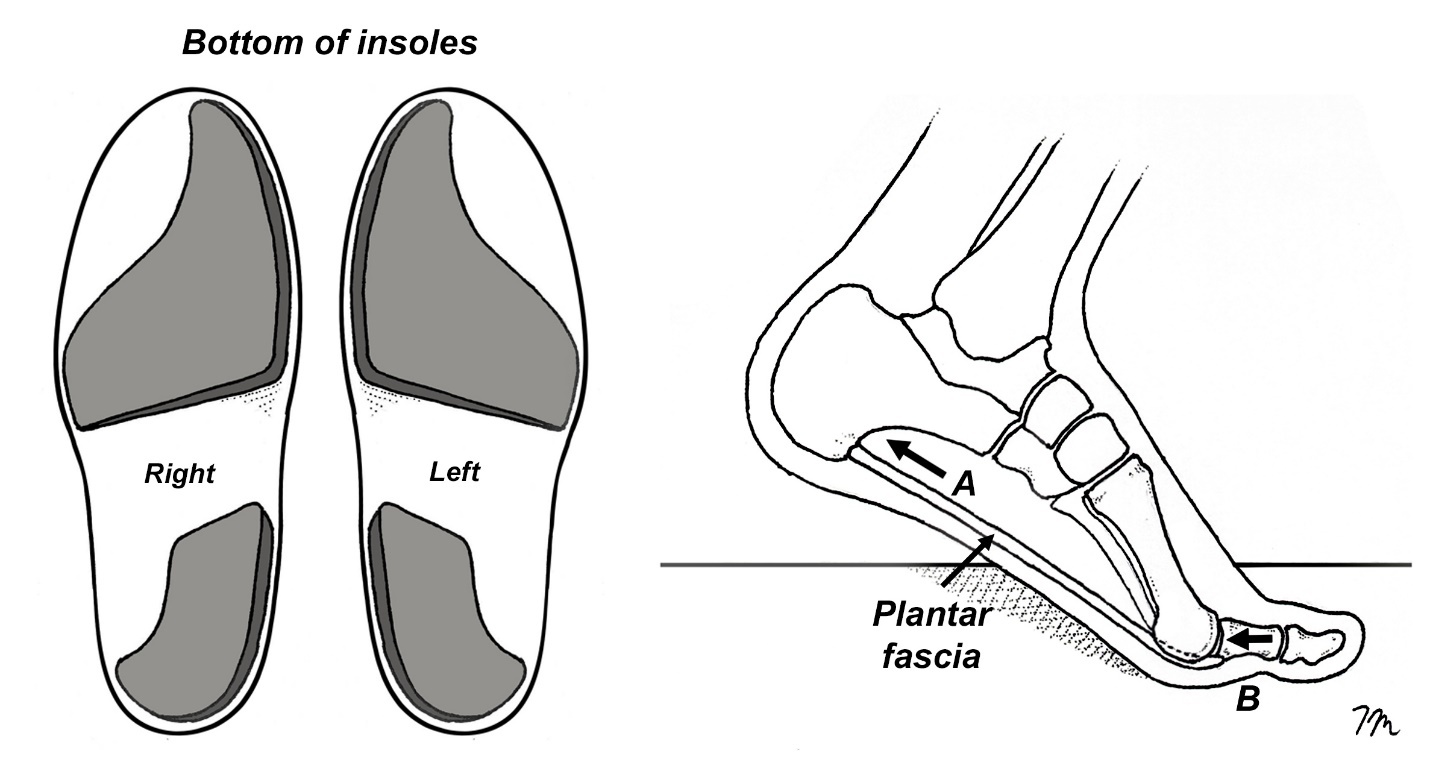
The term turf toe was initially introduced in 1976 by Bowers and Martin to describe a hyperextension injury of the first MTP in football players wearing flexible shoes while playing on synthetic turf.1 The rapid and often extreme range of first MTP dorsiflexion associated with this injury is particularly likely to damage the flexor hallucis brevis tendon, the sesamoids, and the plantar plate located beneath the first metatarsal head (Fig. 1). While turf toe injuries occur in sports such as soccer, jujitsu, and rugby, they are most commonly found among professional football players, with approximately 45% experiencing this injury at some point during their careers.2 While some authors claim that turf toe injury rates on the new synthetic turfs are comparable to turf toe injury rates while playing on grass, a 2025 review of 1.2 million injuries over 5 years suggests otherwise. Reiad et al.3 looked at injury rates in a wide range of sports played on different surfaces and determined compared to playing on grass, football players were 6.3 times more likely to injure their toe while playing on artificial turf. The authors cite several biomechanical studies suggesting that artificial turf exhibits greater rotational stiffness, decreased force absorption, and provides “less cleat release” than natural grass.
DISCUSSION
In a frequently cited study analyzing factors contributing to the onset of turf toe, Rodeo et al.2 reported that the primary mechanism of this injury involves a player’s foot positioned on the ground with the first MTP joint dorsiflexed; subsequent contact by another player to the posterior aspect of the foot then generates a downward force, resulting in rapid and excessive dorsiflexion of the first MTP joint. This contact-related mechanism of injury is described in the vast majority of articles as the primary cause of turf toe injury in the NFL. Despite being widely referenced, turf toe injuries related to player-to-player contact are actually less frequent than previously thought. According to George et al., only 32% of these injuries involve direct contact with another player, while 35% happen without contact, typically when an athlete makes a quick change in direction, which increases both the speed and range of first MTP dorsiflexion. This is consistent with research showing that running backs and quarterbacks are more likely to experience a turf toe injury.4
Because the forces associated in contact-related turf-toe injuries are extreme, management typically requires increasing shoe midsole stiffness and/or using graphite insoles to limit first MTP dorsiflexion. In contrast, noncontact-related turf toe injuries may be managed by controlling the first MTP during dorsiflexion and strengthening the intrinsic muscles and tendons responsible for decelerating this movement. It is important to recognize the differences between contact and noncontact turf toe injuries, as just like ACL injuries, noncontact turf toe injuries are often modifiable and amenable to specific rehab techniques that may appreciably reduce injury rates.
The Connection Between Turf Toe, Flat Feet, and Functional Hallux Limitus
In a 2023 review updated review of treatment options for managing turf toe, Gupta et al.5 list “increased foot pronation” as a risk factor for developing turf toe injury. This statement is supported by Rodeo,2 who point out that among the 30 NFL players evaluated in their study following turf toe injury, nearly 75% of them possessed flat feet, which is much greater than what is typically found in the general population. There are several biomechanical reasons that people with low arches are more likely to develop turf toe. Firstly, as demonstrated by Hillstrom et al,6 excessive pronation causes the medial displacement of the talus relative to the calcaneus, which causes a medial displacement of ground reactive forces that greatly increases pressure centered beneath the hallux during propulsion. The medial displacement of force in people with low arches creates an environment in which ground reactive forces elevate the first metatarsal head relative to the second metatarsal head, engaging a bony locking mechanism that limits MTP motion. This bony locking mechanism is referred to as functional hallux limitus (Fig. 2).
Originally described in 1972 by Laird7 and popularized by Dananberg,8 functional hallux limitus specifically refers to a condition in which the first MTP possesses an adequate range of motion off-weight bearing, but a limited range of motion while weight bearing as ground reactive forces maintain the first metatarsal in an elevated position. While there are conflicting ranges cited in the literature, Halstead et al9 claim that functional hallux limitus is present when there is greater than 50° first MTP dorsiflexion off-weight bearing, and less than 40° of first MTP dorsiflexion while weight bearing. Functional hallux limitus is especially common in individuals with hypermobile first rays, and this anatomical variant is frequently seen in low arched individuals.
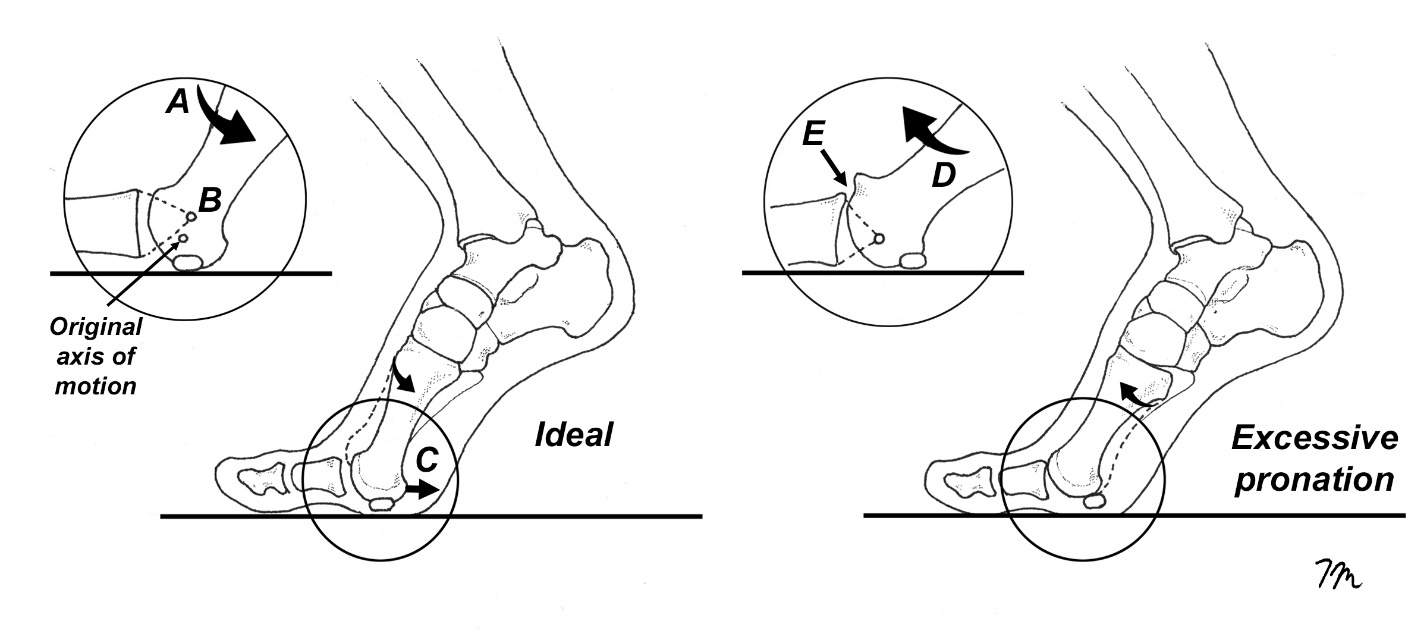
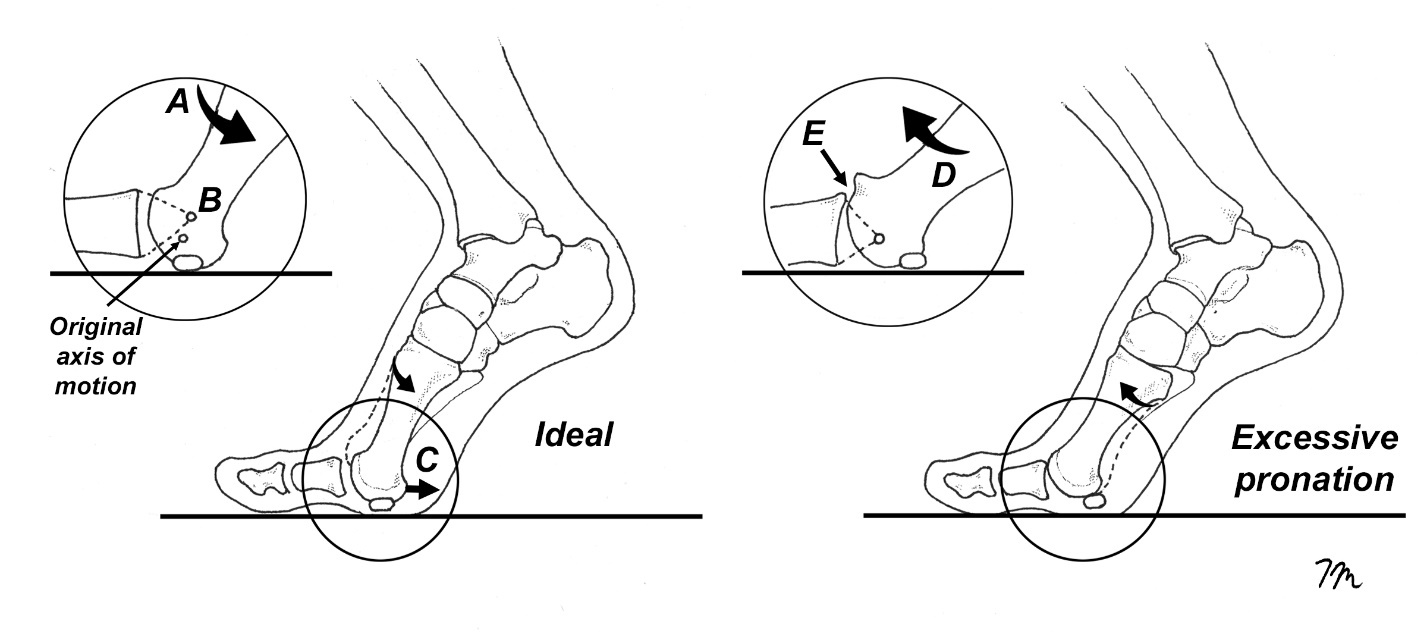
As an individual with functional hallux limitus accelerates during propulsion, the first MTP dorsiflexes until the proximal phalanx collides with the dorsal aspect of the first metatarsal head. When this occurs, there is a superior shift in the instantaneous axis of rotation that causes the first MTP to gap open on its inferior surface (Fig. 3). Because the elevated forces placed on the first MTP are so extreme during turf toe injury, this sudden gapping creates tensile strains capable of tearing the restraining tendons, ligaments, and other soft tissues responsible for limiting movement. The abrupt restriction in first MTP dorsiflexion associated with the shifting axis is referred to as a “sagittal plane blockade,” and is supported by several cadaveric studies showing that people with hallux limitus, which is extremely common in pronated foot types, have altered motion in the first MTP with dorsiflexion. Shereff et al.10 note that when hallux limitus is present, rather than smoothly gliding up the first metatarsal head, the proximal phalanx moves upward with a “distinctive pattern of distraction and jamming” that compresses the superior aspect of the first metatarsal head until no further motion is possible. Limited flexibility in the plantar fascia, flexor hallucis longus (FHL), and/or flexor hallucis brevis (FHB) play a key role in the development of functional hallux limitus.
Orthotic Intervention
Theoretically, the biomechanical locking associated with an excessively pronated foot could be prevented if the first metatarsal was able to plantarflex. In 2006, I published a paper in JMPT with Deb Nawoczenski showing that it is possible to increase first metatarsal plantarflexion during the propulsive period using a semiflexible orthotic possessing varus posts in the rearfoot and forefoot.12 In our case study, 3D movement analysis showed the posted orthotic increased first metatarsal plantarflexion by 6° and reduced first MTP dorsiflexion by 5° while walking. Nawoczenski and Ludewig13 had previously shown that orthotics possessing varus posts in the rearfoot and/or forefoot could increase first metatarsal plantarflexion during propulsion by an average of 3°.9 Although one of the orthotics used in this study was posted only in the rearfoot, recent research shows that in order to control pronation during the propulsive period, which is when turf toe occurs, the best biomechanical outcomes typically occur when the orthotic is posted both in the rearfoot and forefoot, as conventional rearfoot posts alone and/or arch supports are unable to modify motion during the pushoff phase of gait.14
An alternate technique for modifying first MTP dorsiflexion during propulsion is to make a custom orthotic from a non-weight-bearing plaster cast taken with the first MTP fully dorsiflexed. Casting in this position causes the proximal phalanx to plantarflex the first metatarsal head, creating a positive model possessing an exaggerated decline angle to the first metatarsal. Researchers from Spain15 used this casting technique and molded a series of 3 mm polypropylene orthotics that were made with EVA extensions beneath the forefoot with cutouts beneath the first metatarsal heads. Subsequent three-dimensional motion analysis confirmed that compared to the control group not wearing orthotics, there was nearly a 3° increase in first metatarsal plantarflexion during propulsion in subjects wearing the orthotics, which the authors claim can increase the ability of peroneus longus to stabilize the medial forefoot during propulsion. Interestingly, a prior study using this exact casting technique found that in addition to increasing first MTP motion during static stance, the individuals treated with these orthotics had significant reductions in ground reactive forces centered beneath the first metatarsal head and hallux.16 Although these researchers did not measure MTP motion while walking or running, the redistribution of force centered beneath the medial forefoot could play an important role in decreasing the frequency of turf toe injuries.
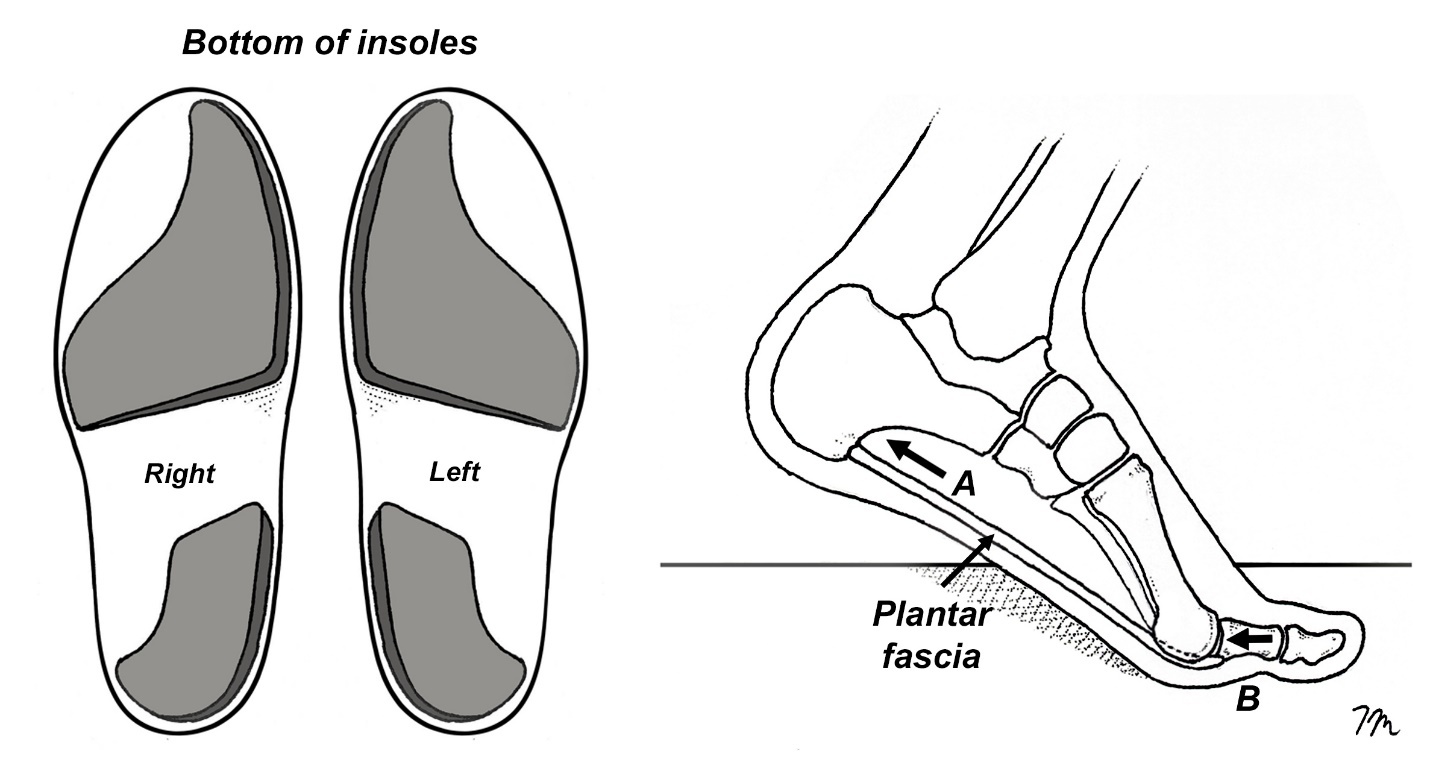
A final consideration when using orthotics to treat/prevent turf toe injury is to bypass the orthotic shell completely and attach two-piece varus posts directly beneath the shoe’s insoles. Researchers from Thailand demonstrate the simple addition of varus wedges placed beneath the heel and forefoot of an insole significantly reduces tension in the plantar fascia during the propulsive phase of gait.17 (Fig. 4) Because increased tension in the plantar fascia during propulsion is a driving agent for the development of functional hallux limitus as it increases compression of the proximal phalanx into the first metatarsal head, it is reasonable to assume the two-piece varus posts could reduce the potential for turf toe injury by lessening strain in the plantar fascia. In addition to lessening plantar fascial strain, these inexpensive posts reduce the overall range of rearfoot eversion and produce significant reductions in the peak range of first MTP dorsiflexion during pushoff.17 Both factors could contribute to reducing the risk of turf toe injuries.
An Alternate Cause Of Functional Hallux Limitus: Restricted Gliding of the Flexor Hallucis Longus Tendon in the Retrotalar Pulley
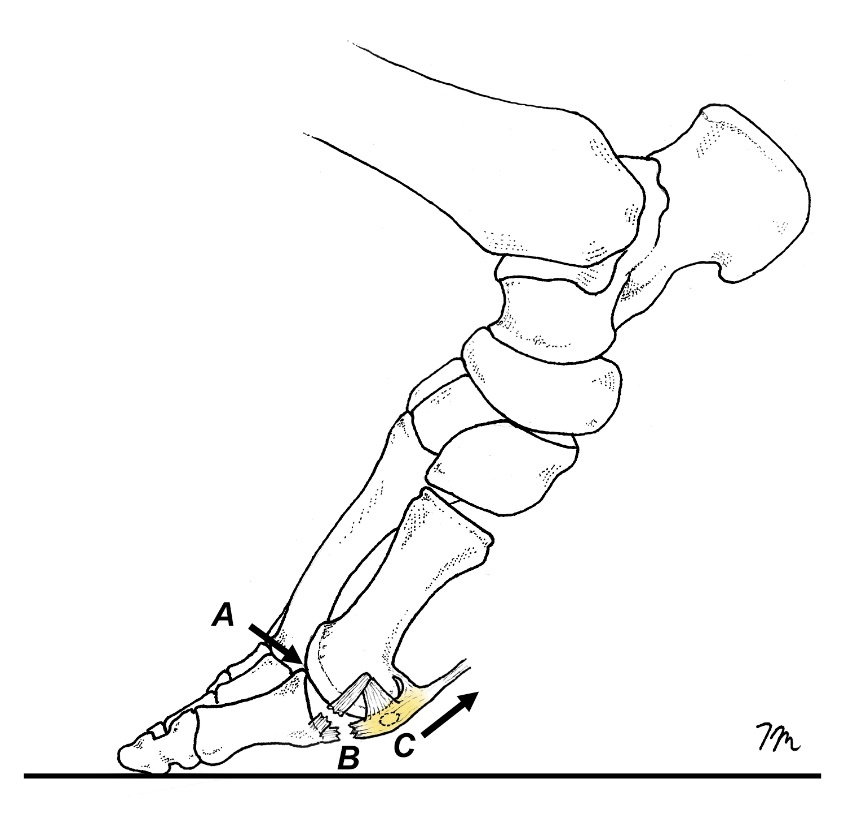
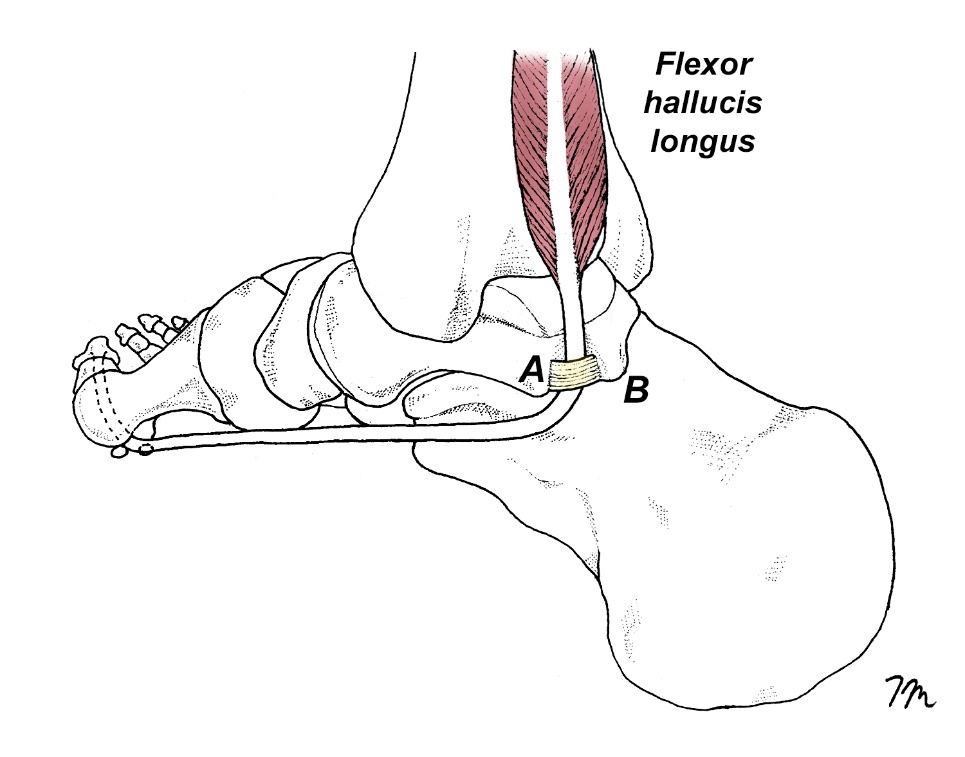
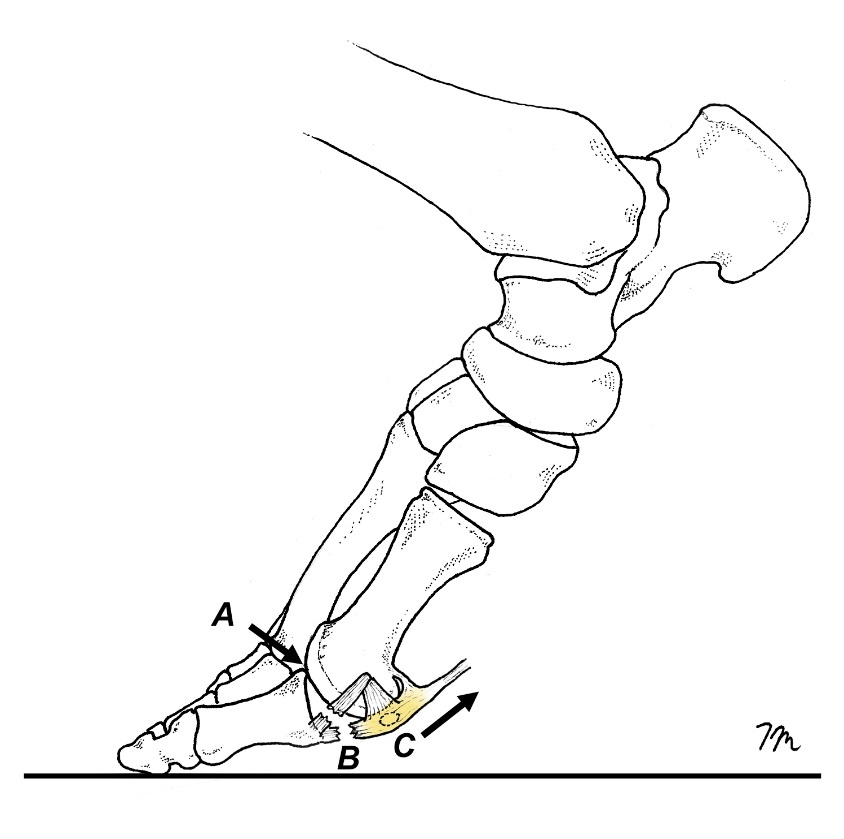
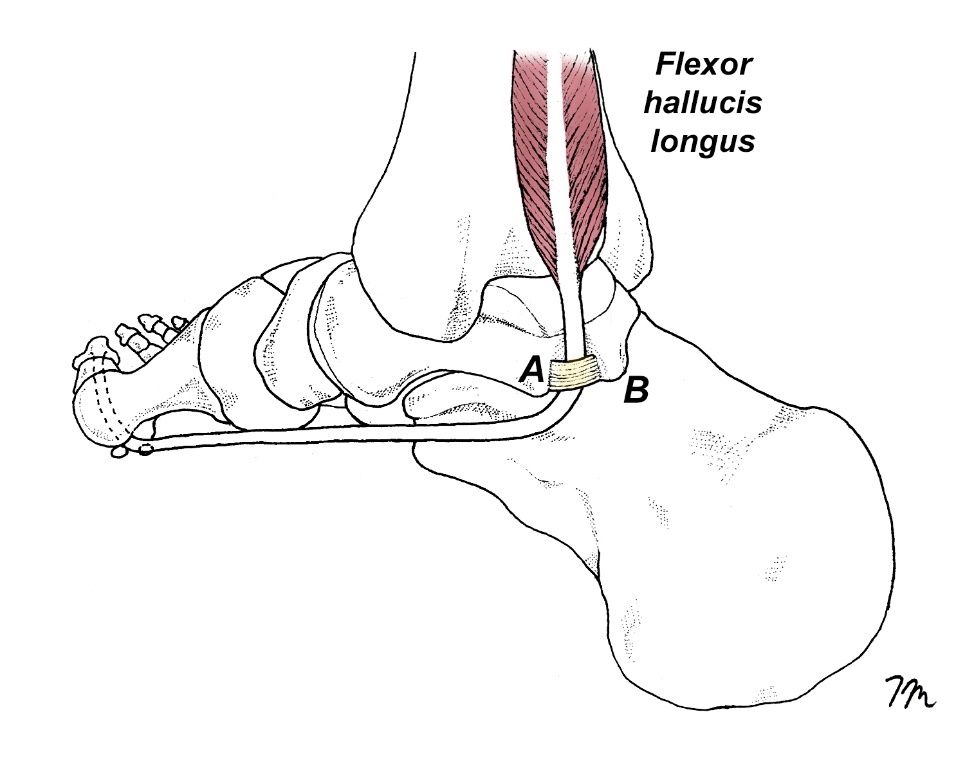
A frequently overlooked cause of functional hallux limitus occurs when the flexor hallucis longus tendon gets trapped in the retrotalar pulley located behind the medial malleolus.18 (Fig. 5) This entrapment limits excursion of the distal flexor hallucis longus tendon, which creates a compressive force on the plantar aspect of the proximal phalanx capable of blocking first MTP motion. Restricted excursion of the FHL may also explain the unusual connection between turf toe injury and excessive ankle dorsiflexion. Originally noted by Rodeo et al.,2 athletes presenting with turf toe injury have significantly greater ranges of ankle dorsiflexion than non-injured athletes (13.3° versus 7.9°, respectively), which the authors were unable to adequately explain. It is possible that athletes with increased ankle dorsiflexion put greater tension on their FHL tendon prior to initiating pushoff, creating a compressive force along the base of the proximal phalanx capable of engaging the first MTP locking mechanism. The rapid restriction and first MTP dorsiflexion may alter the first MTP’s axis of motion, significantly increasing the risk of turf toe injury. Athletes with low arches and limited FHL excursion are especially prone to turf toe injury because of the excessive forces centered beneath the hallux in flat-footed individuals.
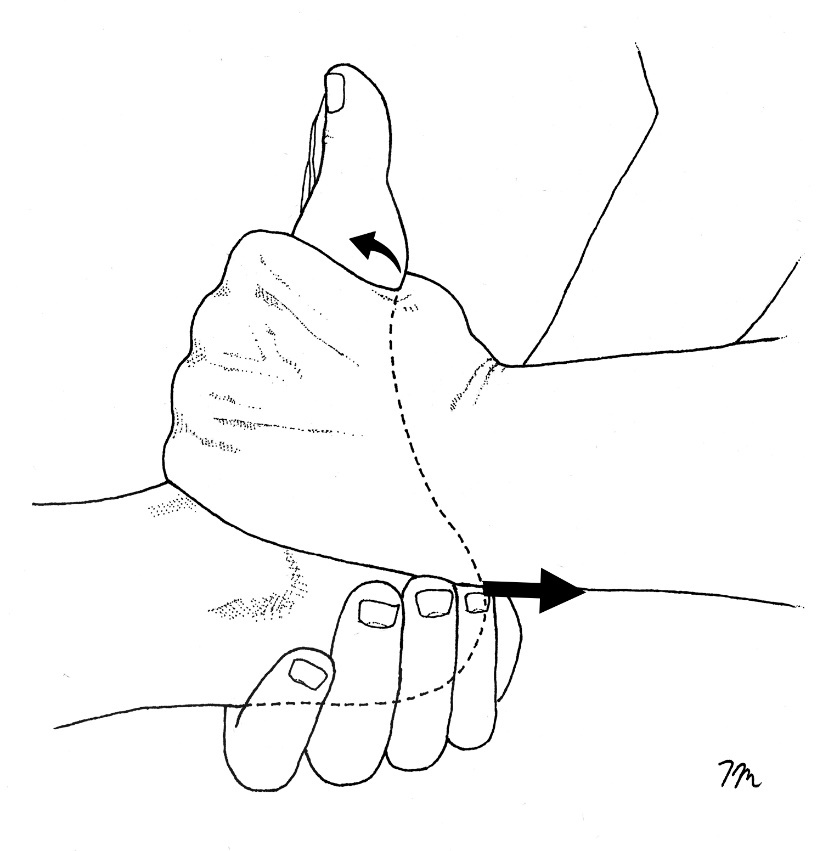
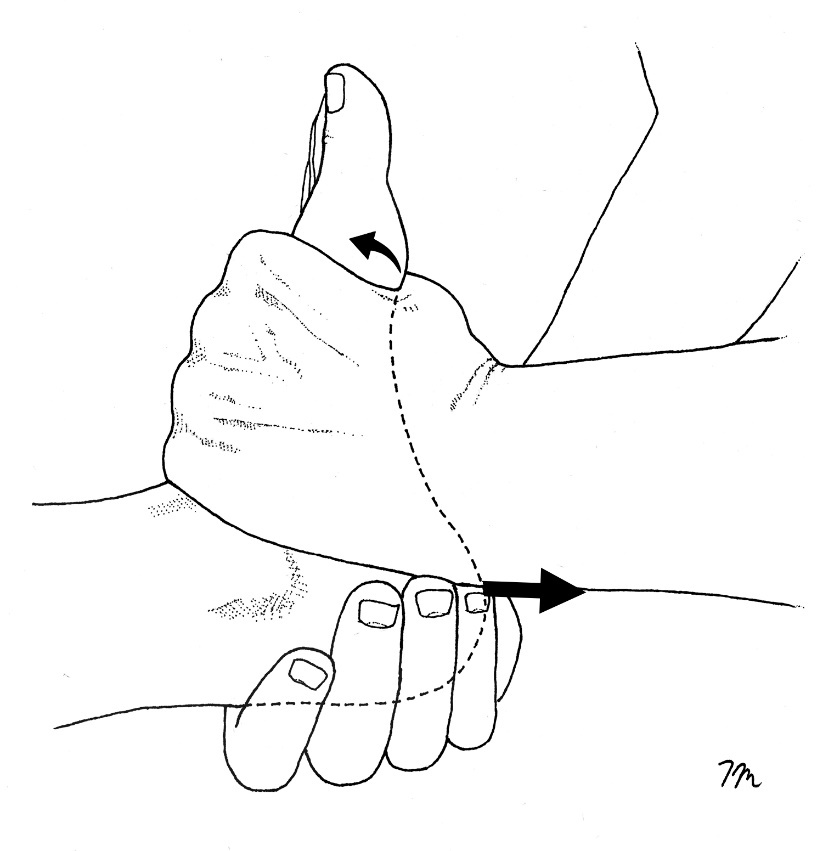
Fortunately, excursion of the FHL tendon is easily diagnosed by performing the FHL stretch test.20 This test is performed by measuring first MTP dorsiflexion with the ankle plantarflexed slightly, and then again with the ankle fully dorsiflexed. The test is positive when first MTP dorsiflexion is significantly limited when measured with the ankle fully dorsiflexed. Researchers from Switzerland note that it is possible to correct limited excursion of the FHL tendon with a simple manual technique known as the Hoover Cord Maneuver.21 This maneuver is performed by grasping the heel with one hand while simultaneously dorsiflexing the forefoot with the other (Fig. 6). The hand grasping the heel creates a firm distraction force while gently rocking the calcaneus from full inversion to full eversion. According to the authors, this maneuver almost always allows for the full restoration of first MTP dorsiflexion, which is immediately apparent to the patient, “who is often surprised to see the recovery of the great toe’s range of motion after the manipulation.” The authors performed this mobilization on 16 participants and noted immediate increases in first MTP motion in every subject. To prevent continued entrapment of the flexor hallucis longus tendon in the retrotalar pulley, bent knee calf stretches performed with a towel beneath the hallux should be performed daily.
The effect of Limited First MTP Motion Following Injury
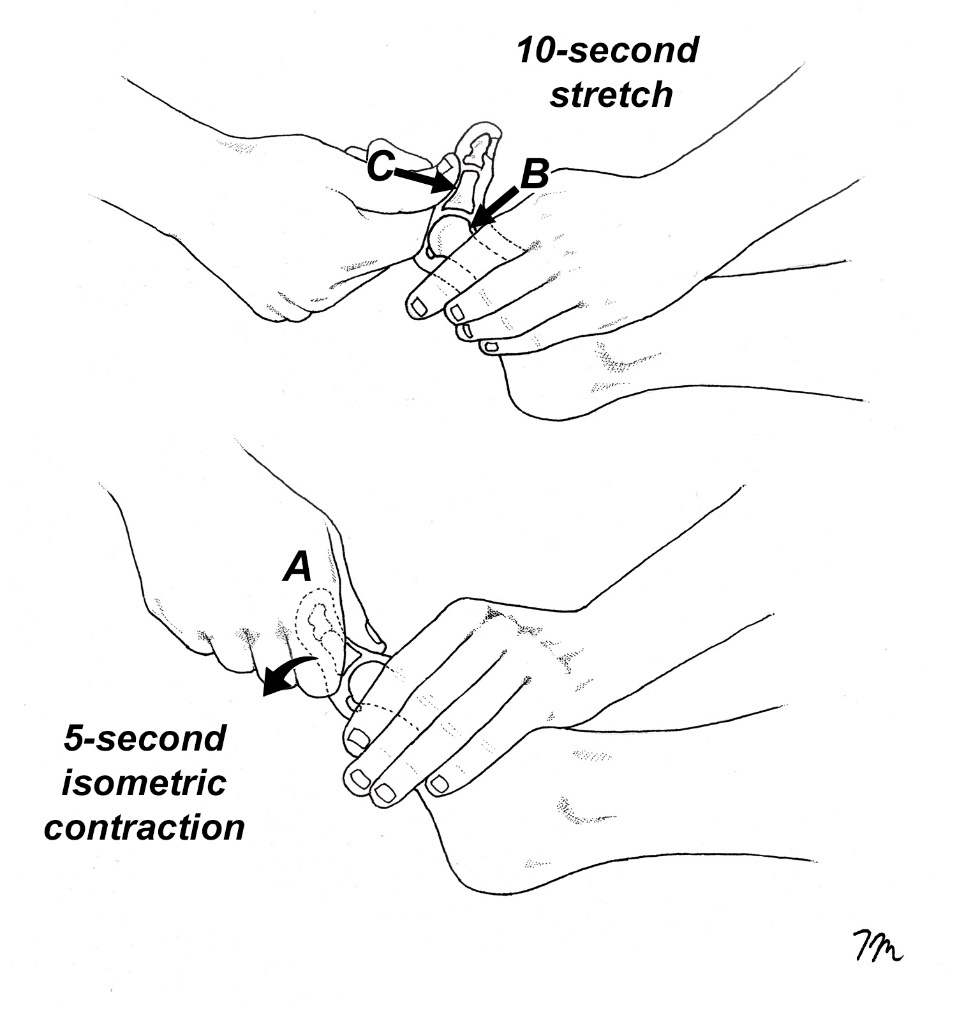
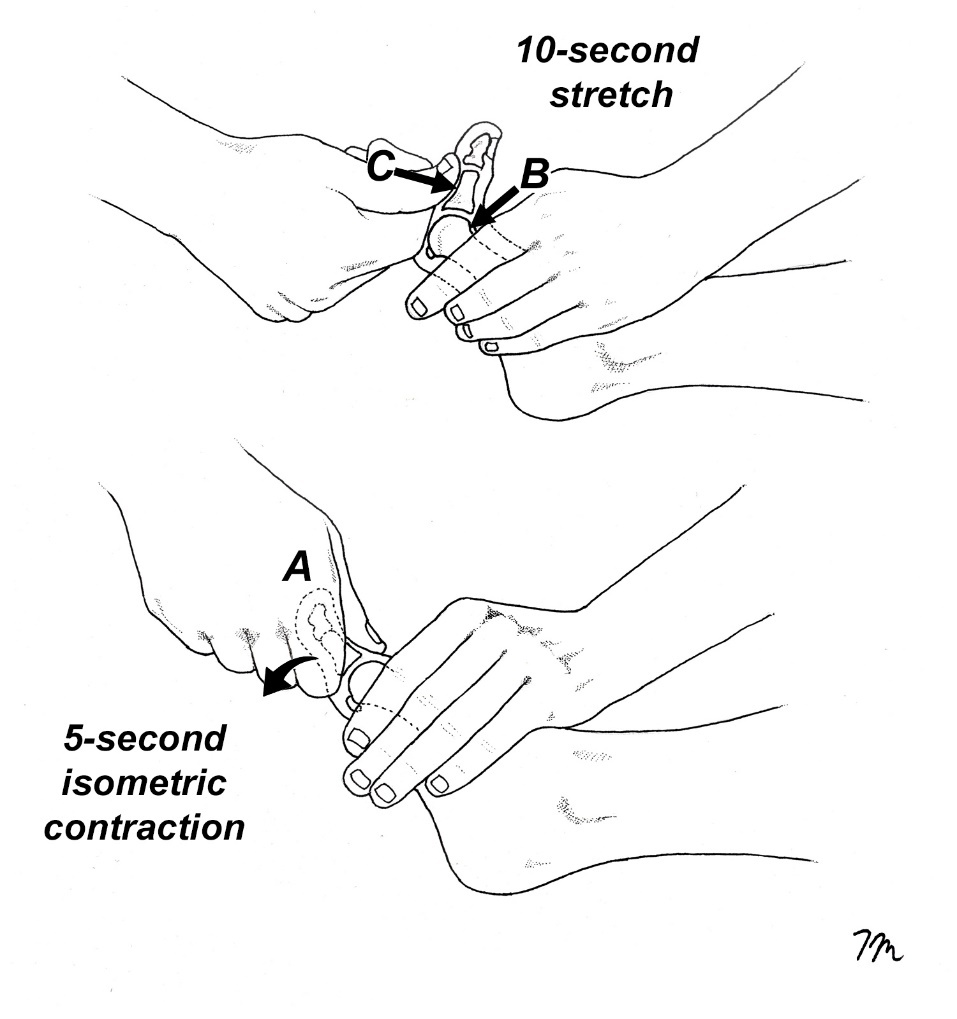
Regardless of whether prior injury was contact or noncontact related, prior injury is notorious for limiting first MTP motion. Brophy et al.22 showed that football players with a prior history of turf toe had an 8° reduction in first MTP dorsiflexion compared to uninjured athletes (40.6 versus 48.4°, respectively). This significant limitation of motion may predispose the restraining structures to tear should the MTP be forced to rapidly dorsiflex beyond the reduced range. While first MTP motion may be limited following injury because of plantar fascia and/or FHL contracture, one of the most common causes for limited MTP motion following a dorsiflexion injury is contracture of the FHB muscle. This is easily distinguished from impaired gliding of the FHL because with FHB contracture, first MTP motion is limited with the ankle in a neutral and a dorsiflexed position, while FHL contracture only limits MTP dorsiflexion with the ankle dorsiflexed. When FHB contracture is present, it is easy to restore dorsiflexion with the muscle energy stretch illustrated in Fig. 7. This muscle energy stretch is also used to determine if contracture in the plantar fascia is limiting first MTP motion, as the plantar fascia is naturally stiff and inflexible, it does not lengthen in response to gentle hold relax stretches. Although occasionally problematic, contracture of the plantar fascia in my opinion is a rare cause of post-traumatic limited MTP motion, as the overwhelming majority of people presenting with turf toe injuries have rapid restoration of motion with hold-relax stretching. Although some authorities advise that athletes not return to sport until off-weight-bearing dorsiflexion reaches 50 to 60°, evidence from a cadaveric study by Framenco et al.11 indicates that most turf toe injuries occur at angles below 78°. Consequently, it is recommended that the target for off-weight-bearing first MTP dorsiflexion on both the injured and uninjured sides be set at 75–80°. Of course, this target goal may not be possible for all athletes, but the mobilization illustrated in figure 7 produces surprisingly large increases in first MTP dorsiflexion.
The Overlooked Role of Strengthening Muscles and Tendons
In order to resist the extreme forces associated with turf toe injury, it is important that the muscles and tendons that limit first MTP motion be as strong as possible. A powerful FHL and FHB can protect against excessive sagittal plane motions, while abductor and adductor hallucis can stabilize the first MTP in the transverse plane. Although it has no direct attachment to the first MTP, peroneus longus is an especially important muscle because it is the most powerful stabilizer of the medial forefoot. As demonstrated by Brophy et al,22 athletes with prior turf toe injury generate significantly less pressure beneath their first metatarsal heads compared to uninjured athletes, making peroneus longus strengthening essential for the treatment and prevention of turf toe injuries.
Needless to say, for exercises to work well, they should boost both muscle activation and force production. Surprisingly, that doesn’t always happen. Osborne et al.23 recently assessed EMG activity and torque generated at the metatarsophalangeal joints with 16 commonly prescribed foot and ankle exercises. Their findings revealed an intriguing paradox: certain exercises elicited substantial muscle activation, yet these EMG increases did not correspond to greater force output beneath the forefoot. Specifically, the short foot, squat, and toe spread exercises, which are frequently prescribed when managing turf toe injuries, were particularly ineffective at increasing metatarsophalangeal joint torque. They state the mismatch between muscle activation and force output occurs because the muscles are exercised in their shortened positions, which greatly impairs force production. Following this logic, other commonly prescribed exercises for managing turf toe, such as towel curl and marble pickup exercises, would also produce negligible changes in force output toes and should therefore be avoided. Goldman24 showed that optimal effectiveness in strengthening the toe muscles is achieved when exercises are performed with toe muscles in their lengthened positions, resulting in strength gains that are four times greater than those observed with conventional exercise methods. In addition to strengthening muscles, tendons also respond well to being exercised in their lengthened positions, particularly with prolonged isometric contractions. Several studies have shown that performing as few as 4, 30-second isometric contractions with tendons maintained in their lengthened positions produces appreciable gains in tendon strength,25,26 which would allow them to tolerate greater force before failure.
Evidence-Based Exercise Prescription
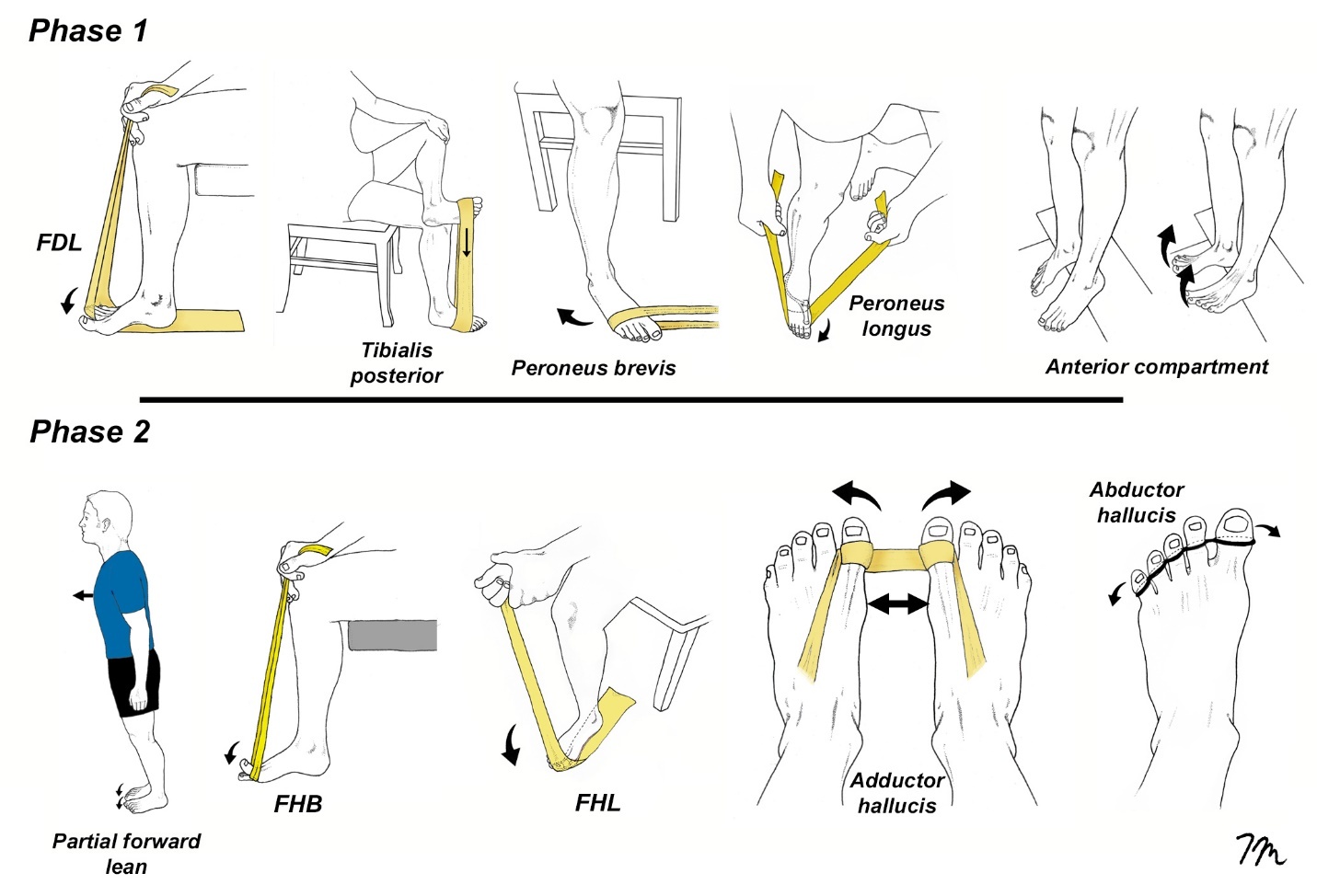
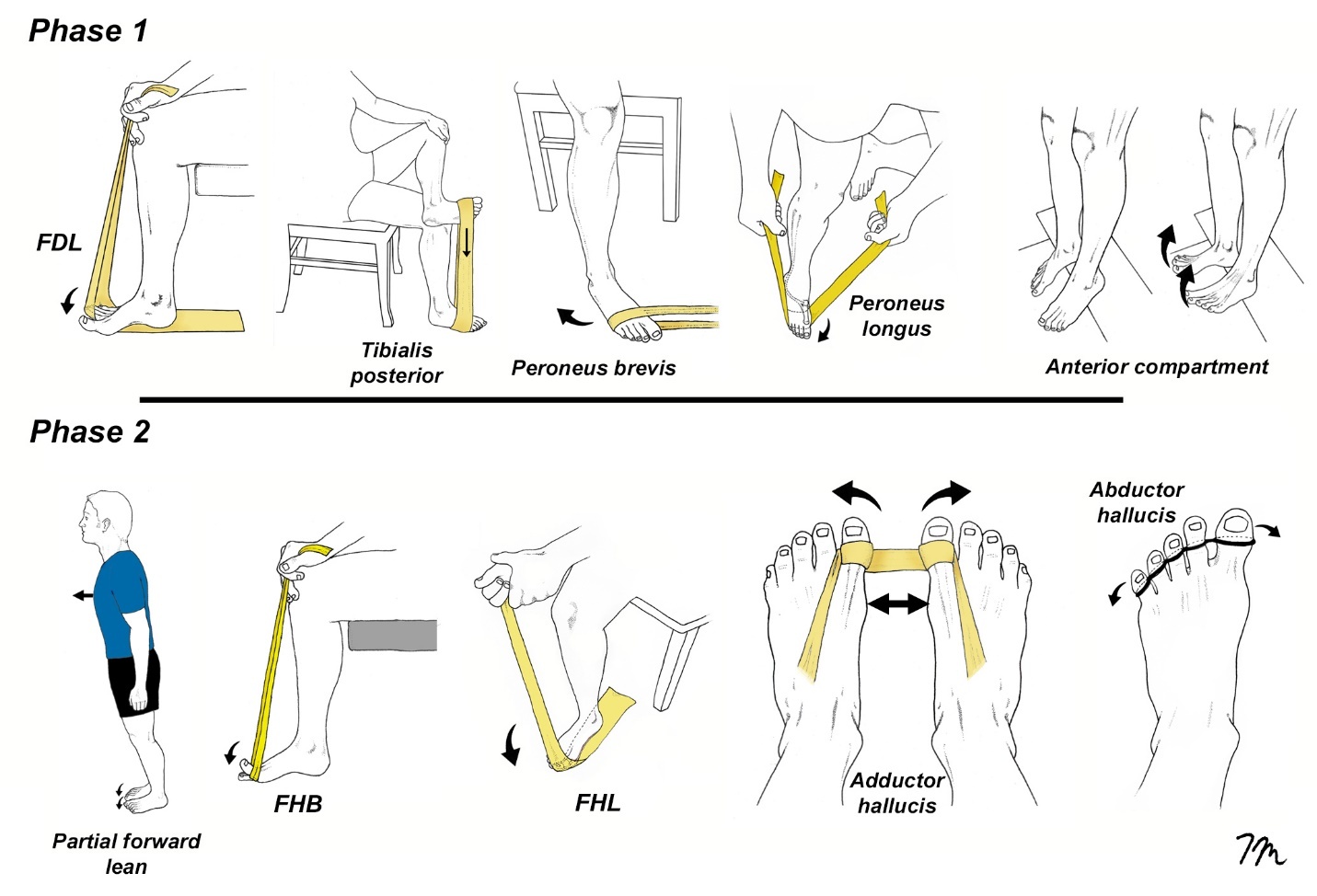
Turf toe rehabilitation is typically broken down into four stages depending upon the severity of injury. The primary goal of phase 1 exercises is to enhance foot strength and mobility without placing strain on the first metatarsophalangeal (MTP) joint (Fig. 8). In contrast, phase 2 exercises introduce controlled motion of the first MTP joint within a limited range, applying minimal force. Elastic bands are used for most phase 2 exercises, and the timing of movement is set to the beat of metronome, which has been proven to reduce intracortical inhibition and increase motor output following injury.27 For phase 1 and 2 exercises, a regimen consisting of four sets of 25 repetitions performed to fatigue is commonly recommended, as this protocol has been shown to promote significant muscle hypertrophy even with low resistance.28 After completing each set, athletes are instructed to perform a 30-second isometric contraction at 60 to 90% of maximal effort, maintaining the muscles in a lengthened position throughout. Perhaps the most important phase 2 exercise is the partial forward lean maneuver, as this simple exercise has been shown to increase force output at the metatarsophalangeal joint by 78%.23 Because the force centered beneath the hallux with this exercise is so high, early stages of this exercise are performed by leaning forward just a small amount, gradually increasing the degree of forward leaning as strength improves.
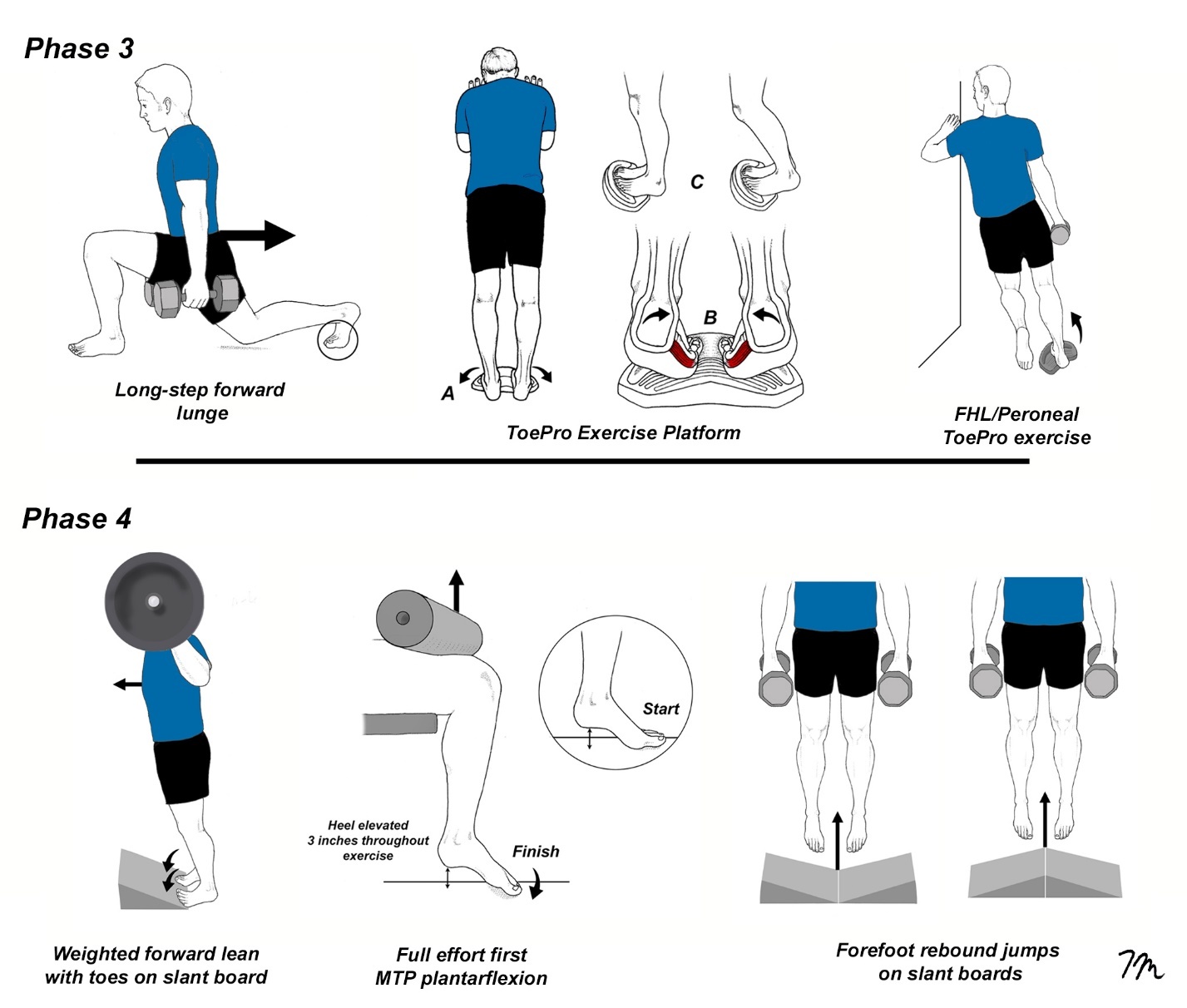
As athletes progress to phase 3 (Fig. 9), elastic band exercises are replaced with more aggressive weight-bearing exercises, which are performed with muscles in their lengthened positions. It is possible to determine if an athlete is ready to begin phase 3 exercises by measuring force generated beneath the hallux with a toe strength dynamometer. This device has excellent interrater reliability29 and athletes should be able to generate 10% body weight beneath their hallux before beginning these exercises. One of the most effective phase 3 exercise is the ToePro platform. A pilot study from Temple University30 demonstrated that performing ToePro exercises three times a week for six weeks led to a 35% increase in force generated beneath the hallux, with improvements in single-leg balance. The peroneal/FHL exercise ToePro exercise is particularly effective at increasing force output beneath the medial forefoot. The intensity of these exercises gradually increases and as strength increases, prolonged isometric contractions are added at the end of each set, which in addition to improving tendon strength, also act as a natural analgesic.31
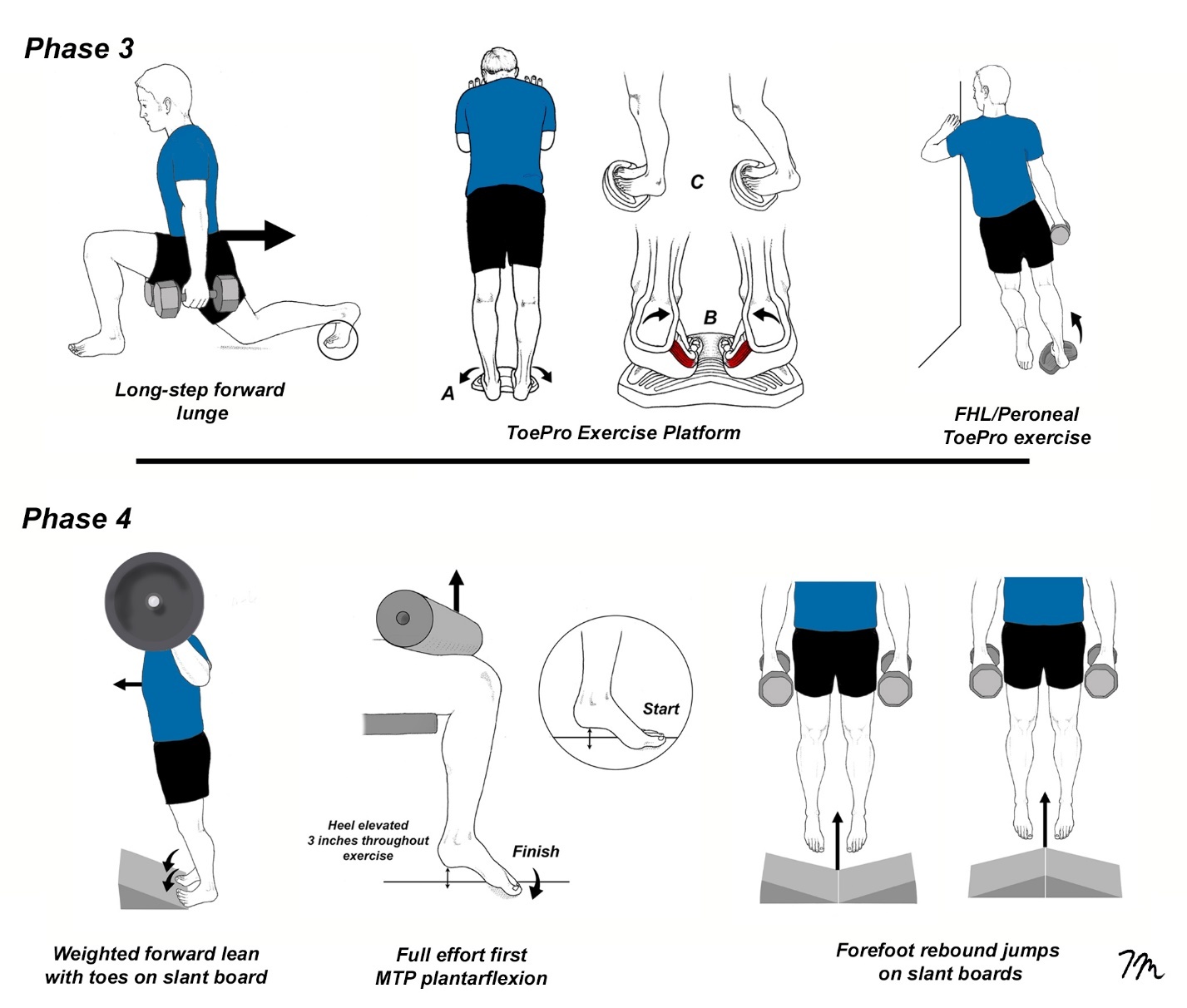
The phase 4 exercises make the transition away from low to moderate load/high repetition exercise routines towards heavy load/low repetition exercises. Many of the phase 4 exercises were adapted from an article by Tourillon et al.,32 who performed an 8-week strength training routine on 28 highly-trained athletes. They discovered that these exercises not only strengthened the muscles that stabilize the first MTP joint, which is crucial for preventing turf toe, they also improved athletic performance. Specifically, participants demonstrated enhanced cutting ability, better side-to-side force transfer, and greater vertical propulsion at top speeds. These benefits are valuable for athletes at any skill level. Although not illustrated, the final stage 4 exercises include various plyometric drills, such as single leg hops, aggressive sprinting with changes in direction, four-way hip strengthening, and a variety of core exercises. Because these drills are aggressive, athletes should be monitored closely.
Conclusion
Comparable to ACL injuries, turf toe should be classified as being either a contact or noncontact related injury. While contact related turf toe injuries may be managed with continued improvements in synthetic turf technology and changes in shoe gear, noncontact related injury should be managed with specific interventions that correct the faulty first MTP motions associated with functional hallux limitus; i.e., pronators should be treated with orthotics or insole modifications possessing varus posts in both the forefoot and the rearfoot, and individuals with either FHB or FHL contracture should be identified and treated with the appropriate manual techniques. Although there is no current research directly connecting functional hallux limitus to turf toe injury, the recommended interventions are safe with little potential to produce injury. Advanced strengthening exercises should be encouraged, as multiple studies have demonstrated that foot strengthening routines not only reduce the overall incidence of injuries among athletes,33 but also result in notable improvements in speed, jumping ability, and agility.24,32,34,35