Introduction
This case report describes the case management of a patient who experienced a primary spontaneous pneumothorax (PSP) as an adverse event of high-velocity, low-amplitude spinal manipulative therapy (HVLA-SMT). It explores the management of the PSP condition from diagnosis to return to activity and illustrates the importance of proper screening and evaluation prior to the application of SMT.
Case Report
A 25-year old male experienced sudden onset of chest, ribcage, and thoracic spine pain after receiving thoracic SMT two days earlier.
He stated that 3 days prior to his presentation, he had woken with left-sided neck pain. He sought no treatment at the time, as he attributed it to how he had slept the night before. The following day, he received thoracic spine SMT via a knee chest technique and had an adverse response, experiencing slight pain in the upper left side of his chest. The next morning, he was riding his bike and hit a large bump, causing sudden sharp chest pain in the same upper left side as the day before. He also began having difficulty breathing.
The student was an established patient at our office and sought out examination for the concerning findings. He had previously reported that he was a former tobacco and marijuana smoker. At the time of his initial visit, he was experiencing both chest and neck pain, with radiation from the upper left side of his chest around his ribcage to the inferior border of his left scapula. The chest pain occurred anytime he would lean his torso to the left, inhale deeply, or lay down. He had no pain with exhalation. In addition, he reported that he was still having difficulty taking a deep breath and was feeling a “clicking sensation” in his chest whenever he would inhale.
A full examination was performed, including vitals, general observation, palpation, range of motion, motor and sensory testing, and orthopedic exam of the chest, thoracic, and cervical regions. He was a tall, thin male who stood 75 inches inches tall and weighed 180 pounds with a body mass index of 22.5. All of his vital signs were within normal limits and consistent with previous examinations.
Cervical examination suggested that his neck pain was mechanical in nature, with local, left-sided neck pain being reproduced by left lateral flexion, right rotation, and left foraminal compression and alleviated by cervical distraction. No sensory, motor, or reflex abnormalities were present in the cervical spine.
No bruising or deformity was present on his thoracic spine or chest. There was no palpable tenderness along the chest, ribcage, or thoracic spine. Sensory examination showed no abnormalities. Auscultation of the lungs revealed normal breath sounds. No tactile fremitus was present and percussion of the chest was resonant. Both left lateral flexion and left rotation of the torso caused sharp chest pain with radiation along the left ribcage. Thoracic expansion assessment revealed symmetrical movement of the ribcage but reproduced the patient’s chest pain. Rib compression was negative in the seated position but positive for chest and rib pain at levels T3 to T5 in the supine position. Sternal compression was positive for increased chest pain. Due to the symptoms, examination findings, and mechanism of injury, x-rays were ordered to rule out fracture of the left rib.
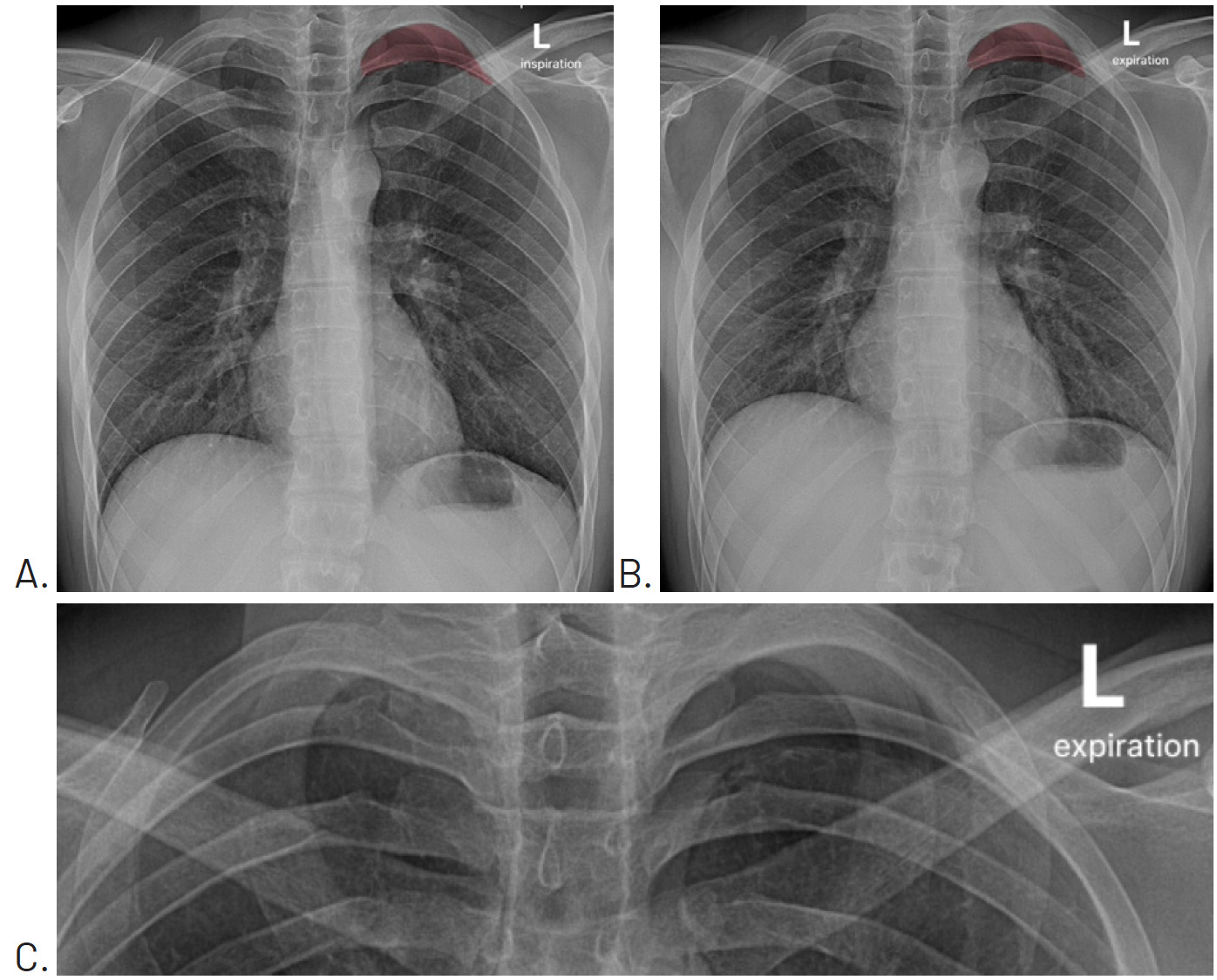
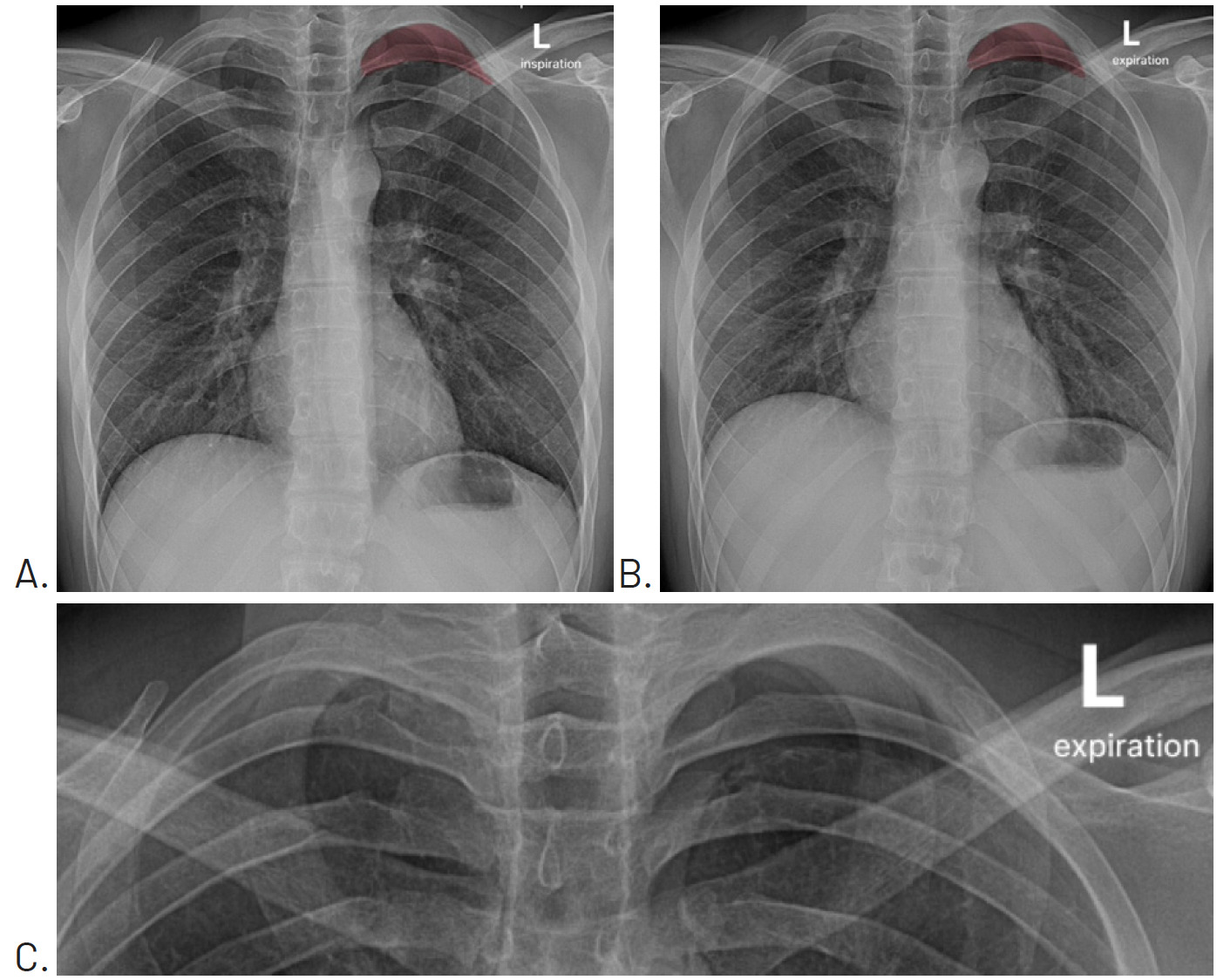
A posterior to anterior chest, posterior to anterior left rib, and left oblique rib were performed the day after examination. No fracture was evident. However, the chest image included what appeared to be a small pneumothorax at the apex of the left lung field. The attending radiologist asked that the chest x-ray be repeated with both inspiration (Figure 1A) and expiration (Figure 1B). These views confirmed the presence of a small pneumothorax at the apex of the left lung.
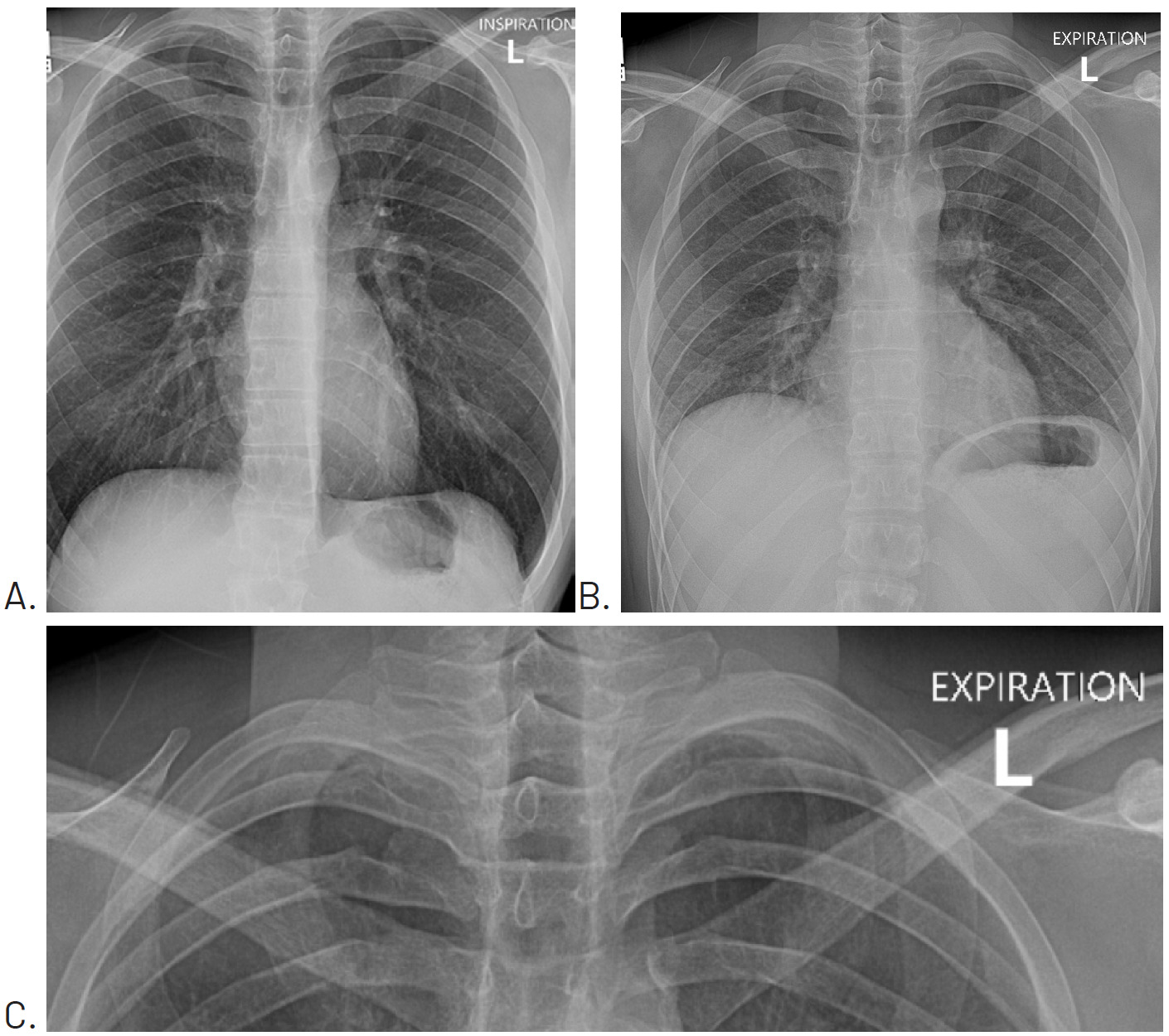
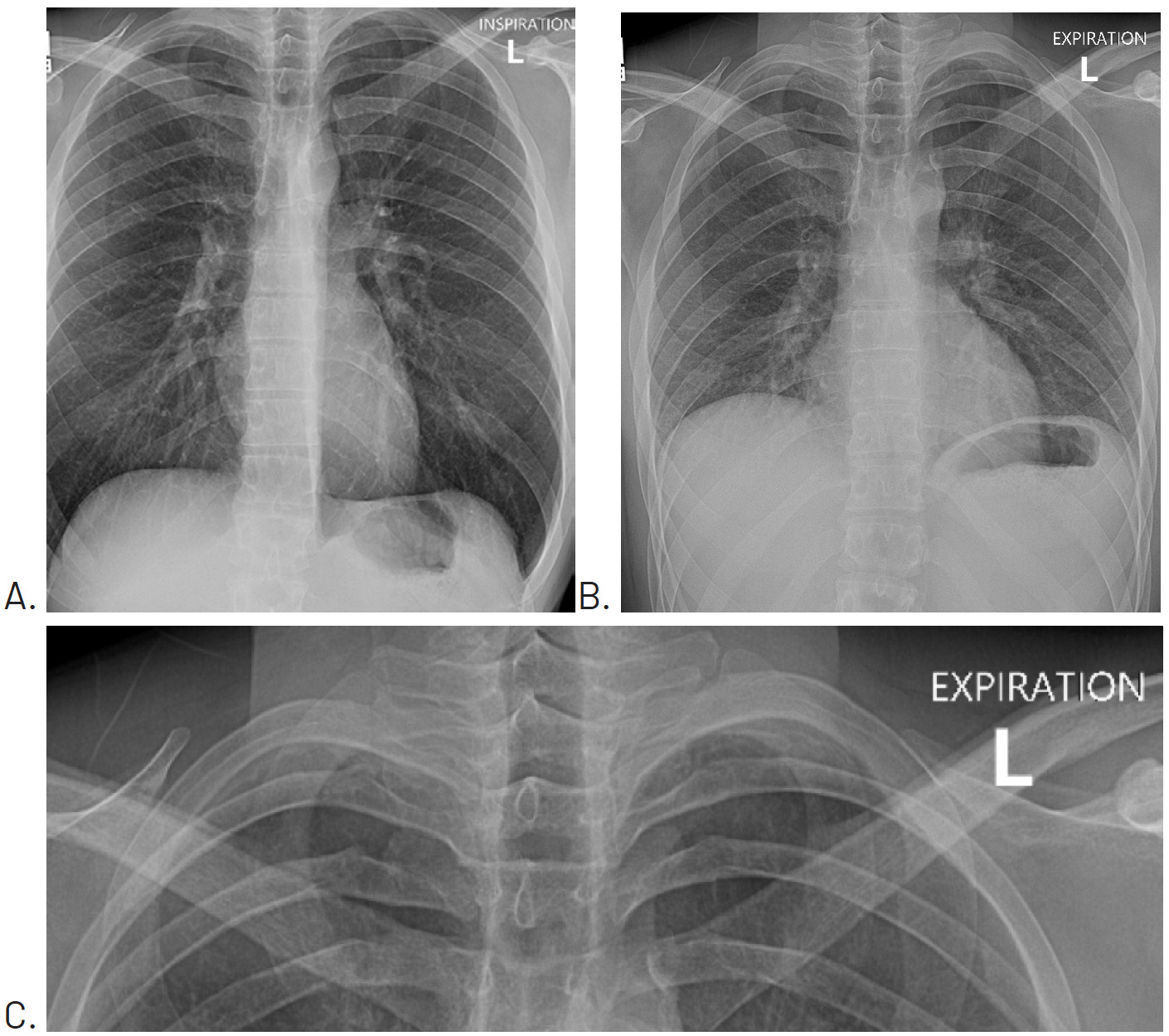
Since the patient was not currently experiencing respiratory distress, he was told to monitor his symptoms over the weekend, and that should any worsening occur in his pain or ability to breathe to seek emergency medical care. Four days later, a repeat chest x-ray with inspiration (Figure 2A) and expiration (Figure 2B) views was performed and showed that the pneumothorax had resolved.
During his follow-up visit the next day, now 1 week since the initial onset and 1 day since x-rays showed resolution, the patient noted that his chest was still bothering him slightly and that he was struggling to get a deep breath during strenuous activity. A rehabilitation program was developed in order to gradually increase his tolerance to cardiovascular activity.
The rehabilitation program was developed in 3 phases, with increasing cardiovascular demand across each phase. In order to appropriately prescribe the intensity of work for the patient, a combination of Rating of Perceived Exertion (RPE) and Talk Test was used as a proxy for exercise intensity. The details of each phase can be found in Table 1.
He made gradual progress over the course of the next 8 weeks. The chest and thoracic spine pain at rest resolved within the first week alongside the resolution of the pneumothorax. He still reported some chest pain with exertion over the first 3 weeks, but it reduced as time went on. After 8 weeks of rehabilitation, he felt completely better and was released from care.
Discussion
PSP is defined as the presence of air in the pleural space without a known traumatic event or underlying lung disease. This contrasts with secondary spontaneous pneumothorax (SSP), which occurs in the presence of underlying lung disease, such as COPD or emphysema. Spontaneous pneumothoraces show a bimodal age distribution, with PSP most commonly affecting young adults, and in particular, young men, while SSP primarily affects older individuals.1,2
A Danish study reported an annual incidence rate of 12.3 per 100,000 men under 40 years of age and 2.2 per 100,000 women, suggesting that PSP occurs 5.9 times more often in young men than young women. Furthermore, the peak age range for PSP in men was between 16 and 25 years of age with an incidence rate of 24.7 to 28.1 per 100,000 men, while women showed a more even distribution of occurrence, with a peak incidence rate of 4.2 between the ages of 31 and 35.1
The clinical presentation often includes sharp, unilateral chest pain and shortness of breath. The onset is typically at rest and not during physical activity.3,4 Small PSPs may present with a normal physical examination, while larger PSPs may show decreased breath sounds and tactile fremitus with hyperresonant chest percussion. In rare cases, tension pneumothorax may occur and clinicians should be aware of signs such as hypotension, tachycardia, tachypnea, and cyanosis.3 Musculoskeletal symptoms have also been shown to include pain in the thoracolumbar spine, rib cage, and shoulder.4,5 This is especially relevant to the chiropractor as these are conditions that routinely present to the chiropractic office.
PSP is a serious medical condition that must be recognized and managed appropriately. For small PSPs without significant breathlessness, guidelines recommend observation and repeat chest radiographs to monitor for resolution. Those who have large PSPs, show significant difficulty breathing, or have underlying lung disease should be referred for urgent medical treatment.2,6 Given that most cases of PSP occur at rest, patients should not be discouraged from partaking in physical activity to prevent recurrence.3,4 Rather, once patients have a normal chest x-ray, they should start a progression of activity beginning with low to moderate intensity aerobic exercise and building to higher aerobic stress, guided by symptom response and the patient’s personal goals and physical demands.7 It is important that providers can recognize the signs, symptoms, and risk factors for PSP and manage appropriately.
Thoracic SMT is generally considered a safe and effective intervention for neck, back, and shoulder pain. Providers often feel more comfortable applying SMT to this area of the spine, and data shows it is the most commonly manipulated spinal region.8,9 However, side effects are common and adverse events, while rare, do occur.10 Yet, this region has received significantly less attention in regards to safety, guidelines, red flags, and adverse events.9
The literature detailing adverse events from thoracic SMT is limited and based on systematic reviews of case series and case reports. To evaluate the literature in this area PubMed, Google Scholar, EBSCOhost, and the Index to Chiropractic Literature were searched up to April 2025 for the search terms “spinal manipulation” AND “adverse events” AND “thoracic”. Abstracts were then screened for relevant studies detailing adverse events following thoracic SMT.
To date, 2 systematic reviews detailing thoracic adverse events currently exist.8,9 The first outlined 10 cases in which adverse events occurred after thoracic SMT directly. The most common adverse event was spinal cord injury (n = 7), followed by hemothorax and pneumothorax (n = 2), and finally, dural sleeve injury causing cerebrospinal fluid leak (n = 1).9 The second review was more broad and encompassed thoracic adverse events following SMT applied to any spinal region. Similar to the earlier review, the adverse events reported were spinal cord injury (n = 13), fracture (n = 3), hemothorax and pneumothorax (n = 3), esophageal rupture (n = 1), thoracic aorta rupture (n = 1), and partial pancreatic transection (n = 1).8 In addition to these reviews, a survey of physiotherapists from 20 countries reported 100 responses of adverse events due to thoracic manipulation, including fracture (n = 43), spinal cord symptoms (n = 6), and disc prolapse (n = 4).11 Finally, a recent case series that was not included in the latest systematic review detailed 3 incidents of rib fracture following thoracic SMT.12 The reporting of adverse events following spinal manipulation is poor and not consistent with established standards.13 The 21 unique cases of adverse events from the 2 systematic reviews when compared to the reports from practicing clinicians highlights that the adverse event data in regards to thoracic manipulation is limited and likely under-reported.
The cases of pneumothorax and hemothorax are most relevant to the current report. The lone case of pneumothorax occurred in a 20-year-old woman who received a “bear hug” maneuver from her boyfriend to “crack her back” and relieve her back pain. She was described as a slender woman who smoked a half a pack of cigarettes daily for the previous four years. She reported to the emergency department complaining of thoracic back pain and vague chest pain that was worse on inspiration.14 The second case described a 17-year-old male who experienced a large hemothorax after receiving osteopathic manipulation to the thoracic spine via the Bauerngriff maneuver, a technique in which the patient is seated with his or her arms in front of them and the clinician positioned behind. The clinician then applies an impulse to the patient’s thoracic spine by lifting them upwards during maximal expiration. The patient was described as a “slender patient with a good state of health.” His symptoms after manipulation included dyspnea and dull pain in the mid region of the anterior and posterior left thorax.15 The final case described a 57-year-old male who was receiving daily manipulation-under-anesthesia as treatment for ankylosing spondylitis. He presented to his chiropractor for a routine follow up, where he was found to have reduced oxygen saturation and was referred to the emergency department, where he reported dyspnea, lightheadedness, and back pain. He was diagnosed with a left hemothorax and complex fracture of the T8 and T9 vertebral bodies.8,16
To my knowledge, this is the first published case detailing pneumothorax as an adverse event following HVLA thoracic manipulation with a technique taught in professional chiropractic programs. It highlights a need for proper screening and evaluation prior to the application of thoracic SMT.
Yet, there is currently a gap in the literature regarding examination and screening procedures for the thoracic spine prior to SMT.8 Clinical practice guidelines exist for chiropractic management of patients with both lower back pain17 and neck pain,18 but not for thoracic spine pain. One clinical prediction rule for the use of thoracic SMT has been published to aid providers in determining which patients with mechanical neck pain would benefit from thoracic SMT,19 but it was unable to be validated in a follow-up study.20 Two cross-sectional surveys have examined how physiotherapists approach the management of thoracic spine pain in clinical practice.11,21
This leaves providers in a position where they may extrapolate information from other resources to make up for the lack of direct data available. While certain contraindications, such as osteoporosis, malignancy, fracture, infection, and progressive neurological deficits can be taken from guidelines in other regions and extrapolated well,17,18,22 pulmonary complications are more specific to the thoracic region and may warrant more specific screening. Suggested history and evaluation items for patients with thoracic spine pain are listed in Table 2 to aid providers in screening for current PSP or those patients who may be at risk of developing PSP as an adverse event of thoracic SMT.2,23,24
Risk factors for PSP include male sex, being a current or former smoker, and having a tall, thin body type. Smoking status is of particular importance as the risk of developing PSP in men who smoke is 12%, while for non-smokers, the risk is only 0.1%.2 Smoking cessation is of particular importance in reducing recurrence. Those who cease smoking significantly reduced the odds of recurrence than those who do not, with an odds ratio of 0.26.25 Yet, 84% of patients of young adults continue to smoke after their first pneumothorax.26 The effect of smoking is not just isolated to tobacco. Research into the association between cannabis smoking and PSP occurrence revealed that daily tobacco smoking increased the risk of PSP with an OR of 4.85, but combined cannabis and tobacco smoking increased risk with an OR of 8.74. This effect was isolated to men, and the OR of cannabis in isolation was not significant.27 Relative to height, patients with PSP tend to be taller than their healthy counterparts. The apices of the lungs in taller individuals are subjected to higher distending pressures and may predispose to the formation of subpleural blebs.2
While PSP has traditionally been described as occurring in the absence of lung disease, evidence suggests that the lungs of PSP patients are often not “normal.” Thoracoscopy has found increased porosity, distal airway inflammation, and emphysema-like changes (ELC) in the lungs of PSP patients.28 Computed tomography and histopathologic examination have identified similar findings, with higher incidence in smokers, strengthening the relationship between smoking and PSP risk.23
Recurrence rates are high, often being described between 20% and 50% within the first year.4,23,25 Given these high rates and previous adverse reactions being listed as a relative precaution for future SMT,9 providers should be very cautious in applying thoracic SMT to patients who have experienced PSP before or as an adverse event of spinal manipulation.
Conclusion
This case report explored the diagnosis and management of a patient with PSP following HVLA manipulation of the thoracic spine. Based on the details of this report and others before it, it is recommended that providers consider pneumothorax as a differential diagnosis in patients who report chest pain or difficulty breathing after receiving SMT. Extra caution should be taken with those patients who demonstrate risk factors for PSP, especially smoking status or pre-existing lung disease. The prototypical profile of a patient who may be at risk of PSP is a tall, thin, young adult male who is a current or previous smoker, although females should not be excluded.1,2,23 Through proper history and evaluation, providers may identify patients who are at higher risk of adverse events and weigh the benefit of SMT versus possibly safer alternatives. Future research should investigate the incidence of adverse events of thoracic SMT and deliver guidelines for providers to develop a framework for pre-SMT examination.
Consent
Written informed consent was obtained from the patient for publication of this case report and any accompanying images.