Introduction
Calcium pyrophosphate deposition disease (CPPD) was first discovered in 1842 and first observed on radiographs in 1922.1 The clinical presentation can range from asymptomatic to chronic inflammatory arthritis.2 The clinical presentation in this case report is likely consistent with chronic CPPD in a patient suffering from knee pain beginning in 1985. Though not a case study, a report published in November of 2020 showed possible therapeutic value in the treatment of CPPD with extracorporeal shock wave therapy (ESWT).3 Despite concluding that more research needed to be done on the effects of ESWT, the initial results displayed a potential slowing or modification of disease progression in osteoarthritis (OA) and other “gout-like” arthritis to a modest degree.
The pathogenesis of CPPD remains unclear but the formation of the calcium pyrophosphate (CPP) crystals within the cartilage matrix occurs in the initial stage of the disease process.4 Deposition likely results from an imbalance of production between pyrophosphate and the levels of pyrophosphatases in cartilage.2 There are several co-morbidities correlated with CPPD development, including hyperparathyroidism, gout, OA, rheumatoid arthritis (RA), hemochromatosis, osteoporosis, hypomagnesemia, chronic kidney disease, and calcium supplementation.2
Current treatment for calcium pyrophosphate deposition disease primarily focuses on symptom management rather than disease modification. Studies suggest that optimal treatment requires both non-pharmacological and pharmacological treatments.5 No therapies currently exist that directly remove calcium pyrophosphate crystals or prevent their deposition within joint cartilage.6 As a result, treatment strategies are directed toward reducing inflammation and managing acute or chronic symptoms. Common approaches include nonsteroidal anti-inflammatory drugs (NSAIDs), colchicine, and corticosteroids administered either orally or via intra-articular injection. Joint aspiration and intra-articular glucocorticoid injection are frequently recommended for acute mono-articular flares, while low-dose colchicine may be used prophylactically against recurrent attacks. Non-pharmacologic measures, such as rest, cryotherapy, and management of underlying metabolic disorders, are also commonly employed. Despite widespread clinical use, many of these approaches are supported by limited randomized control trial evidence and are often extrapolated from treatment strategies used in gout.
Extracorporeal shockwave therapy (ESWT) was initially developed in the early 1980’s for the non-invasive treatment of nephrolithiasis through extracorporeal lithotripsy. Over time, the technology has been adapted for use in musculoskeletal medicine due to its ability to deliver focused acoustic waves that interact with biological tissues. In orthopedic and sports medicine applications, ESWT has been shown to stimulate biological responses, including neovascularization, modulation of inflammatory mediators, and stimulation of tissue regeneration. These mechanisms have led to ESWT emerging as an acceptable and popular non-invasive management option for conditions such as plantar fasciitis, calcific tendinopathy of the shoulder, and osteoarthritis.7 More recently, investigators have begun exploring the potential role of ESWT in crystal arthropathies, including CPPD, where mechanical and biological effects of acoustic waves may influence crystal deposition, inflammation, and local tissue healing. The proposed mechanisms of action include mechanical fragmentation of calcific deposits, stimulation of angiogenesis through up-regulation of vascular endothelial growth factor (VEGF), and modulation of inflammatory pathways. Experimental and clinical studies have also suggested that ESWT may promote cartilage repair and reduce inflammatory cytokine expression within joint tissues. These effects provide a theoretical rationale for the use of ESWT in degenerative and crystal induced arthropathies such as CPPD.
The literature supporting ESWT in musculoskeletal disorders is substantial; however, evidence specific to CPPD remains limited and existing studies evaluating ESWT use for CPPD and OA are promising. The purpose of this report is to further explore the benefits of ESWT for CPPD arthritis, lending additional insight to the treatment of gout-like arthritis with this therapeutic modality.
Case Report
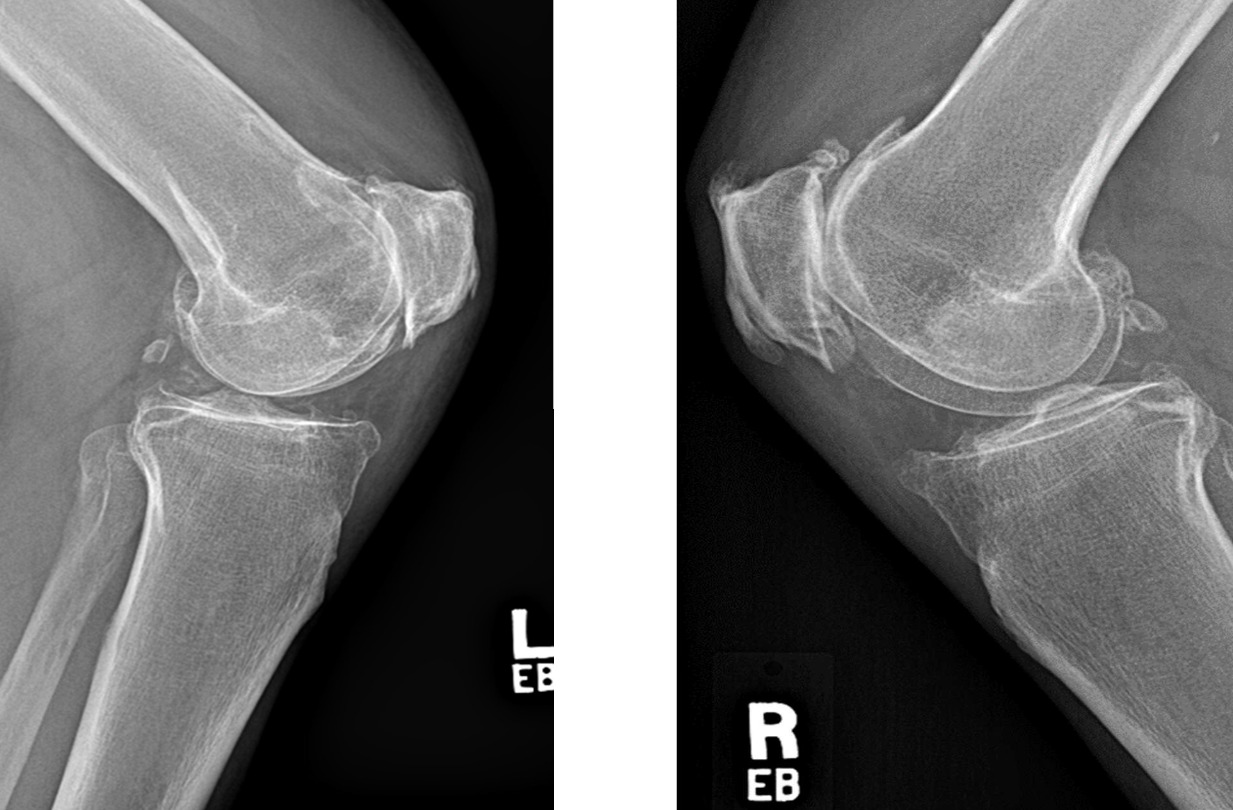
A 59-year-old male patient sought care for bilateral knee pain. which he reported started around 1985. The left knee pain was rated at 4/10 at rest and 7/10 during activity, and the right knee pain was rated at 2/10 at rest and 6/10 during activity on the visual analog scale (VAS). The pain was described as sharp and constant in both knees. Activities of daily living (ADLs) were impacted, including walking, sit to stand, standing, any contraction of the quadriceps, and working in the yard. Several pertinent exam findings were noted, including edema around the patellae bilaterally. In addition, the patient’s range of motion (ROM) was measured in both knees. In the left knee, flexion was measured at 87 degrees and extension deficit of 25 degrees. In the right knee, flexion was measured at 91 degrees and extension deficit of 36 degrees. The patellar ballottment test was performed, in which the examiner stabilizes just above the knee and presses down on the patella with the other hand. It was positive for local pain at the patella in both knees, further confirming our clinical suspicion for bilateral joint effusion. In addition, the patient had pain with valgus and varus stress tests, bilaterally, suggesting pain with manipulation of the medial and lateral collateral ligaments. Pre-treatment LEFS scores were 17/80 for the left knee and 28/80 for the right knee, indicating poor function bilaterally. LEFS scores functional limitations as follows: 0-20 severe, 21-40 moderate, 40-60 mild to moderate, 61-80 minimal or normal. Radiographs confirmed the diagnosis of bilateral knee CPPD (Figure 1).
_and_right_knee_(right_panel)_demonstrate.png)
Management and Outcome
The patient received an initial treatment of low-level laser therapy (LLL), interferential current (IFC), and therapeutic ultrasound (TU) with minimal to no improvement of the initial presentation. He then underwent a series of weekly ESWT treatments over a span of 8 weeks, for a total of 8 treatments. Each ESWT session was characterized by parameters including maximal positive pressure of 1.0 bar, 800 pulses per treatment, and a frequency of 14 hertz, in accordance with the treatment plan parameters established in a previous study.1 In addition to ESWT, the treatment included chiropractic adjustments targeting the thoracic and lumbar regions. However, these adjustments, serving as ancillary interventions, were unlikely the primary drivers of his observed symptom regression.
Following the first treatment, he reported significant improvement, describing the knees as feeling “almost normal” with only mild pain when stomping on the ground. He was also able to jump up and down, which he reported not being able to do in years.
Throughout the duration of the 8-week treatment plan he reported multiple improvements in addition to a notable reduction in pain when seated, standing, and transitioning from seated to standing. For example, he had improvements in his ADLs, characterized by several anecdotes including being able to hop down from a truck and step out of a car. He also felt steadier on his feet and the time required to pick items off the ground decreased from 15 seconds pre-treatment to 6 seconds post-treatment.
He returned for a post-care evaluation after the 8-week ESWT treatment plan. His left knee pain decreased from 4/10 at rest and 7/10 with activity to 0/10 at rest and 3/10 with activity. His right knee pain decreased from 2/10 at rest and 6/10 with activity to 0/10 at rest and 3/10. Since pain was the primary goal for our treatment, pain scores were evaluated for statistical significance. Although statistical testing is not typically emphasized in single-patient case reports, pain scores before and after treatment are presented descriptively to illustrate the magnitude of change. He also reported a decrease in pain frequency from constant pain pre-treatment to pain about 50% of the day post-treatment. His pain quality was described as sharp both pre- and post-treatment. His range of motion improved bilaterally. His left knee post-treatment achieved 167 degrees of extension, a 12-degree improvement, and 84 degrees of flexion, a 3-degree improvement. His right knee post-treatment achieved 173 degrees of extension, a 29-degree improvement, and 82 degrees of flexion, a 9-degree improvement. Clinical exam revealed no edema around either knee. Valgus and varus stress tests were still positive for mild pain bilaterally. Patellar ballottment was positive only in the left knee, suggesting some residual edema. The LEFS scores were 31/80 for the left knee, a 14-point improvement, and 38/80 for the right knee, a 10-point improvement. LEFS score improvement were in the affected ADLs of walking, sit to stand, standing, any contraction of the quadriceps, and working in the yard. Post-treatment knee radiographs did not show any observable changes to bony structures with treatment.
Discussion
This paper describes the use of extracorporeal shockwave therapy in a 59-year-old male patient with chronic bilateral CPPD affecting the knees. Written and verbal informed consent was obtained from the patient prior to treatment as well as written and verbal consent to his case being used for the purpose of this report. Following an 8-week treatment course, he demonstrated clinically meaningful improvements in pain levels, functional capacity, and joint range of motion. Improvements were observed in both subjective patient-reported outcomes and objective clinical measurements, including LEFS scores and physical examination findings.
The potential mechanism through which ESWT may benefit patients with CPPD remains speculative but is supported by emerging evidence from musculoskeletal research. Shock waves generate localized mechanical stress that can stimulate cellular signaling pathways associated with tissue repair. Experimental studies suggest that ESWT may promote angiogenesis, increase local blood flow, and stimulate the release of growth factors involved in tissue regeneration. In addition, ESWT has been shown to modulate inflammatory responses by reducing pro-inflammatory cytokine activity while enhancing anti-inflammatory signaling pathways.
Another possible mechanism involves the mechanical disruption of calcific deposits. In other calcific conditions, such as calcific tendinopathy, ESWT was shown to fragment calcium deposits and facilitate resorption by surrounding tissues. A similar process may theoretically occur with calcium pyrophosphate crystals within joint cartilage or periarticular structures, potentially reducing the mechanical and inflammatory burden associated with CPPD. While demonstrated in calcific tendinopathy, whether similar fragmentation occurs in CPPD remains unclear.
Although radiographic findings in this case did not demonstrate structural changes following treatment, the absence of radiographic progression alongside meaningful clinical improvement may still represent a favorable outcome. Future studies incorporating advanced imaging modalities such as ultrasound or magnetic resonance imaging could provide additional insight into structural changes following ESWT.
Conclusion
Extracorporeal shockwave therapy may represent a promising adjunctive treatment option for patients with symptomatic CPPD who do not respond to conventional therapies. In this case, ESWT was associated with reductions in pain and improvements in functional ability over an eight-week treatment period. While the precise mechanisms underlying these improvements remain unclear, current evidence suggests that ESWT may influence inflammatory pathways and tissue healing, with a theoretical role in calcific deposition processes. Given the limitations of a single case report, further controlled studies are necessary to evaluate efficacy, mechanisms, and optimal treatment protocols.
Acknowledgements
We acknowledge the help of Kaitlyn Boykin, BS, DC.
Disclaimers
Written and verbal informed consent was obtained from the patient prior to treatment. This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.