Introduction
Solon Massey Langworthy, one of the earliest graduates under the tutelage of Daniel David Palmer, is known to students of chiropractic history as an important player in the formative years of the profession.
Langworthy was an exceptional figure in early chiropractic, generally overlooked by the profession’s first historians and generally defamed by modern historians. His impact was to be significant, however. A veritable dynamo of intellectual and practical energy, some have consigned him as but an early opportunist in the wake of the Palmers. Yet enduring evidence presents a more fully and positive conclusion about his brief, yet considerable career.
Solon Massey Langworthy was a man with many gifts. He had a beautiful singing voice, and his services as a vocal soloist were sought by his church and many civic groups in Cedar Rapids.1 Langworthy was also an excellent clinician and combined with his business acumen built a large and profitable practice in a short period of time, earning the equivalent in today’s currency of nearly a quarter million dollars annually.1 With an inquisitive mind and the skill to turn ideas into tangible devices, he would soon become an inventor of instruments designed to aid in the treatment of his patients. Langworthy would then make these inventions available for purchase by the ever-growing number of chiropractors hungry for new technologies to aid in their mission to reduce spinal subluxations.1
Langworthy the businessman had a natural talent for turning any opportunity into a way to produce income.
DISCUSSION
Origins of the Langworthy Adjusting Table
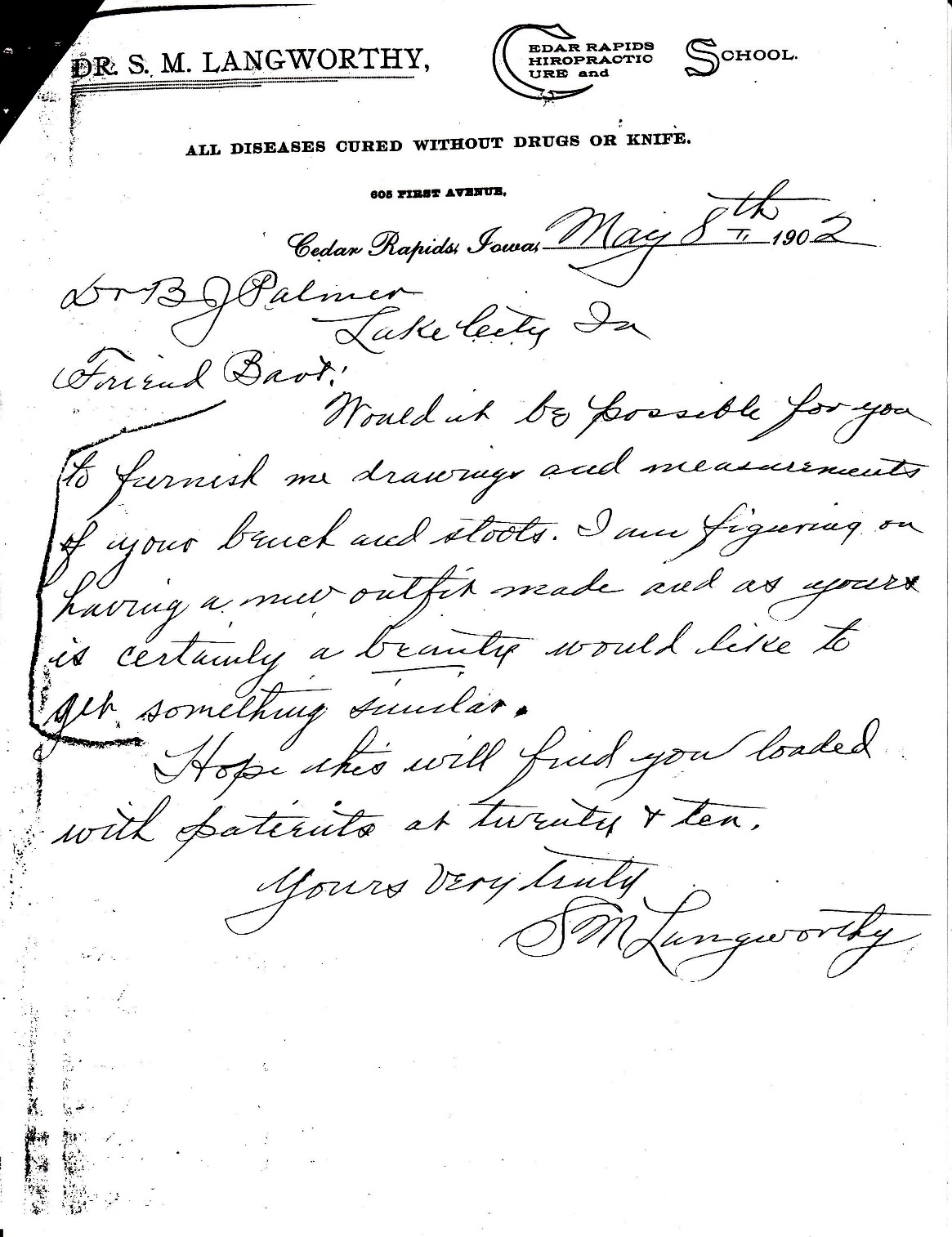
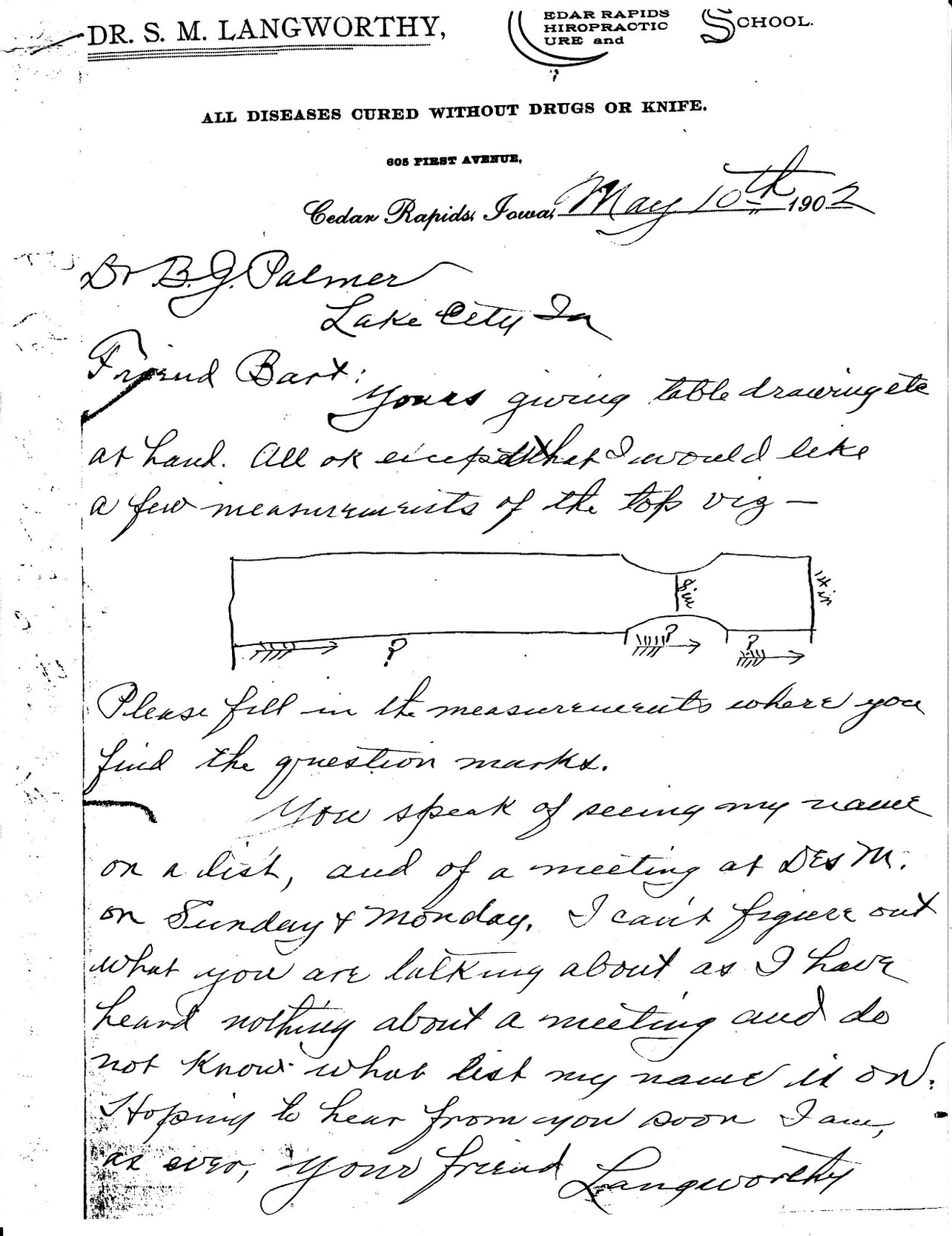
As he applied his manual skills to the many suffering patients that presented to his ever-growing practice, Langworthy saw the need to improve the equipment on which he exercised those skills. In some of his earliest correspondence with B.J. Palmer, Langworthy sought his input regarding the dimensions of adjusting tables (See Figures 1 and 2). Langworthy would find the Palmer tables inadequate for his specific applications.
It appears there are a number of likely reasons why Langworthy would find the Palmer adjusting tables insufficient for his specific needs: First, it should be remembered that Langworthy possessed a degree in osteopathy prior to studying under Old Dad Chiro.1 Certainly this prior education gave him a different perspective from that of the Palmers, as osteopathic methods involved the use of techniques that applied forces in ways that were unlike the high velocity short amplitude thrust of chiropractic methods. These osteopathic moves have been called “muscle energy techniques” or “post isometric relaxation techniques” or “proprioceptive neuromuscular facilitation techniques” that involve practitioner stretching with the patient actively providing resistance by contracting the involved muscles.
Second, he would collaborate with Oakley Smith. Smith was an 1899 graduate under D.D. Palmer in Davenport. Smith would conclude that he did not know enough about anatomy and physiology after completing his education at the Palmer School. Smith would go on to study anatomy and physiology at a number of medical education institutes that would lead him to perform detailed anatomical investigations of the spine’s connective tissues and the contents of the intervertebral foramen.2 Smith’s understanding of the spinal connective tissues would influence his understanding of how to apply forces to the spine to achieve subluxation corrections. It would be unlikely that Smith’s understanding would not be passed to Langworthy as they worked together to improve chiropractic education and collaborated on the first textbooks for teaching chiropractic to students.3,4
To understand the Langworthy perspective, an analysis of the differences between the Palmer and the Smith/Langworthy views must be undertaken.


The Langworthy Rationale
Langworthy referred to his method of patient care as, “Modernized Chiropractic.”5 When studying the works he put forth it becomes apparent that he viewed vertebral subluxations much differently than either DD or BJ Palmer. The classic Palmerian subluxation has been described as a single vertebral phenomenon while Smith/Langworthy proposed vertebral subluxation as more of a combination of segmental and global or postural phenomena. Consider, for example the Palmerian definition proposed in Stephenson’s Chiropractic Text Book6 published by the Palmer School:
“A subluxation is the condition of a vertebra that has lost its proper juxtaposition with the one above or the one below, or both; to an extent less than a luxation; which impinges nerves and interferes with the transmission of mental impulses.”
In contrast, now consider the definition of subluxation as professed by Smith, Langworthy, and Paxson in the Langworthy published text Modernized Chiropractic3:
"A simple subluxation is a condition in which the exact relation between the articulating surfaces of bones has been altered from normal, the articulating surfaces still remaining in partial contact. It is a term that has long been used in a very vague and indefinite way when one considers it from the view point of science in perfect simplicity.
In all books and articles heretofore written wherein vertebral subluxations have been regarded as important causative factors in disease, a subluxated vertebra is spoken of as one would speak of an indented, protruding or slanting brick in a solid brick wall. Likewise, the reduction of a subluxated vertebra has been talked of as one would talk of lining up the displaced brick and pushing or pulling it into a fixed or permanent position.
When one stops to consider the latitude of motion in each of the 24 true vertebrae it becomes apparent that those who have done the most talking about ‘lining up the spine’ have had little conception of the work attempted.
In case of a simple vertebral subluxation, the vertebra is not lodged in a fixed and permanent abnormal position like the displaced brick in the wall; to consider it so is preposterous for it is a movable bone in a flexible and movable column. A simple subluxated vertebra differs from a normal vertebra only in its field of motion and the center of its field of motion, but because of its being subluxated, its various positions of rest are differently located than when it was a normal vertebra.
A vertebra, because of its peculiar shape, because of its articular cartilages, the intervertebral cartilage above and below it and the muscles and ligaments attached to it, is capable of certain circumscribed movements, and it must, therefore have a certain definite center of movement just as a wheel has a hub. It is therefore, obvious that when a change takes place in the bone itself or when any of the attached muscles, ligaments, or cartilages are changed from normal tonicity, consistency, or tension, the center and also the field of motion of the bone is changed. Like a wheel with its hub off center, its field of motion may be too great in some directions and too small in others.
By positions of rest we mean the positions assumed by bones while the body maintains certain poses. If by subluxation, the center of motion and the field of motion are changed it follows that the positions of rest will also be changed from the normal in case of subluxations." (Authors’ emphasis)
Although the Palmerian definition has, as its essential elements- vertebral misalignment causing nerve interference- the Smith/Langworthy/Paxson (SLP) definition is more complex mechanically reflecting the relationship between spinal structure and spinal function. Additionally, the SLP definition introduces the notion that the “positions of rest” of the bones of the spine may be reflected in the “poses” or postures of the subject afflicted with vertebral subluxation. This suggests that a person’s posture could be an important indicator of the presence or absence of vertebral subluxation in the SLP paradigm. This notion is further advanced in other articles written by Langworthy when he discusses the relationship between gravity, erect human posture, the intervertebral foramina and discs, and the aging process.6–8 In these articles he proposes that as individuals age, the intervertebral discs narrow as a result of constant exposure to gravitational pressure. This disc narrowing Langworthy referred to as “vertical subluxation.” He further states that these vertical subluxations would lead to altered posture and narrowing of the intervertebral foramina. The only logical means by which to reverse this condition, Langworthy reasoned, was by the application of specific sustained forces applied to the spine through the use of mechanical devices.
Further, Langworthy proposed that vertebral subluxations could occur—not only as individual displacements—but also as groups of vertebrae that must all be addressed simultaneously, both by hand adjustment and with traction (sustained) forces to affect a more permanent correction. In regards to the genesis of mechanical methods to achieve reduction or correction of spinal subluxations, Langworthy5 states:
“My inventions, the CHIROPRACTIC TREATING TABLE, with anatomical and physiological adjusters, and the LANGWORTHY TRACTION TABLE, were brought out in crude form and finally perfected, simply because ‘necessity is the mother of invention.’ In many cases I felt positive of what should be done to remove the cause of disease, but with my hands alone I could not do it . . . Mechanical Traction and Mechanical anatomical and physiological adjustment are, without doubt, indispensable factors in the removal of the cause of many diseases.” (Author’s emphasis)
The Langworthy Adjusting Table
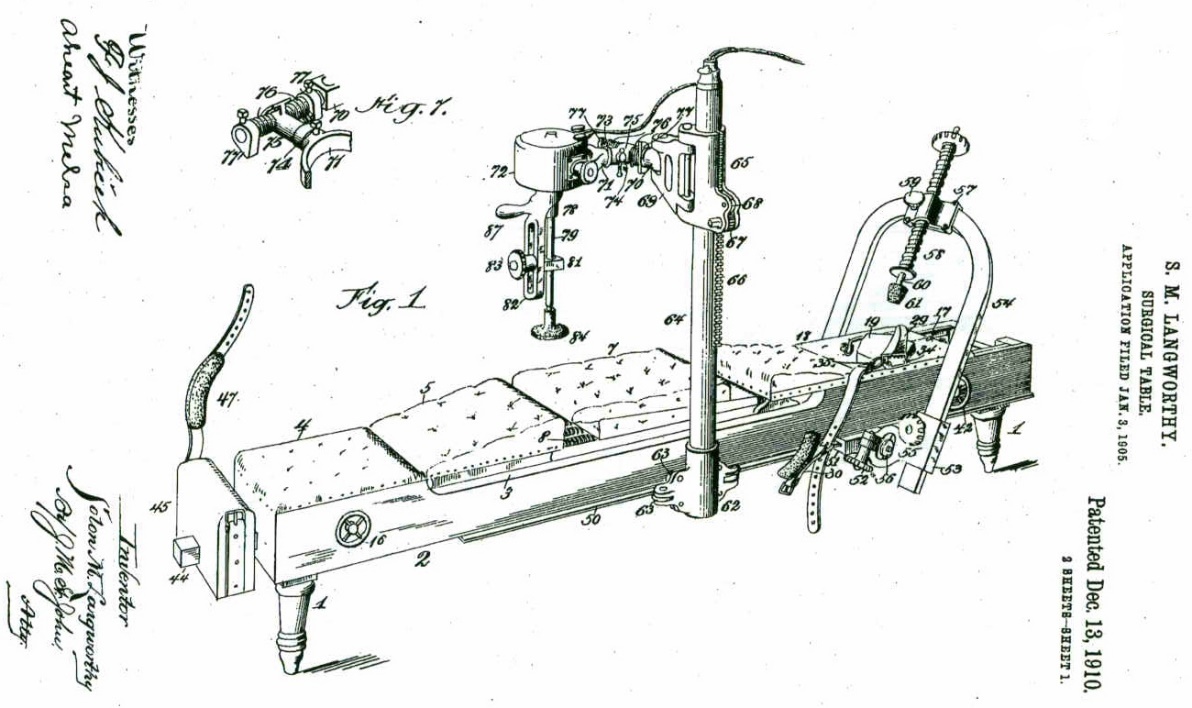
Figure 3 is a drawing from the patent application9 submitted 3 January 1905 for what Langworthy titled a “Surgical Table.” It would take almost 6 full years before the patent was finally issued for the device.

The Langworthy Adjusting Table had a variety of revolutionary features. First, the table-top was upholstered with cushions having coiled springs with varying degrees of elasticity. This innovation was said to provide greater comfort for the patient while at the same time making the corrective thrust more effective.4
In addition to the upholstered cushions, the table had specially designed head, chest, and hip carriages that would allow generalized traction or only localized traction to a specific area of the spine (cervical, thoracic, or lumbar)4:
"The traction idea and the spring idea are in one respect similar. Both make it possible for the adjustment by hand to be more easily secured. The slight tension that is put upon the spine when correction is about to be made under traction appears to relax the muscles, discourage resistance, and stretch the peri-articular structures to just such a degree as to make the movement of the vertebrae by the Thrust more easily secured." (Author’s emphasis)
The specially designed head carriage would also allow the operator to stabilize the head in various positions of lateral flexion. Langworthy considered body position during the adjustment procedure critically important in securing subluxation correction4:
"The position of the patient’s body has considerable bearing upon the nature of the adjustment secured by a given Thrust. The following is one of many illustrations. A Thrust given vertically downward upon a cervical spinous process would produce a different character of movement in the cervical vertebra if the head were rotated to the left than it would if the head were rotated to the right.
In the dorsal and especially the lumbar region the placing of the patient’s body in the proper position on the table has a great deal to do not only with the ease with which the adjustment is secured, but may determine to a large extent whether such adjustment is secured at all. A slight swerve of the patient’s body as he lies on the adjusting table may make all the difference in the world in the effect the Thrust may have upon some vertebrae, especially if the direction of the Thrust is an oblique lateral. Body position as related to the patient is a field which heretofore has received comparatively little attention but which we believe is of sufficient importance to receive the most careful attention." (Author’s emphasis)
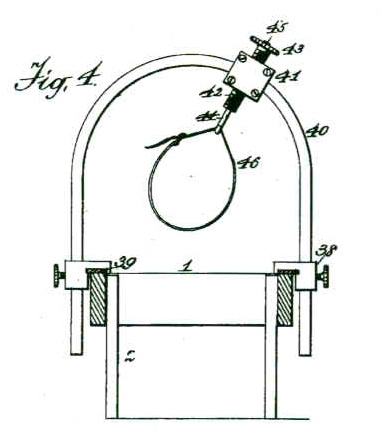
Langworthy also incorporated some additional innovations into his adjusting table. A vibrating electric motor was mounted to an arm and counter balanced so that the applicator arm of the motor could be easily applied to the patient’s body with little or no fatigue for the operator. (Figure 4)

A semi-circular yoke was also found in the design of the Langworthy Adjusting Table, too. This semi-circular yoke was fitted with a tubular screw that had a rubber tipped applicator or “anatomical adjustor” at its terminal end that contacted the patient’s spine. This device was used to apply steady force to the spine at any angle of application. Additionally, it could be argued that this device was the first patented “instrument adjusting” device used in the profession. From the patent application, Langworthy states9:
“The lateral tension device is accordingly set so that the applicator will bear on the part in question, and at precisely the right angle. Then by slow pressure, as by turning the screw, or a sudden thrust, as by striking the applicator rod with a rubber mallet, the faulty member is forced to a proper position.”
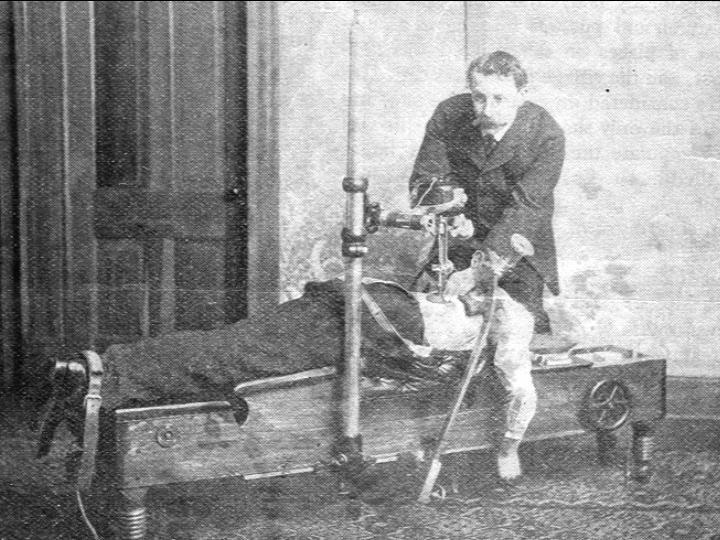
Figure 5 demonstrates Dr. Langworthy using the “lateral tension device” or “anatomical adjustor” on a patient.

Traction Devices
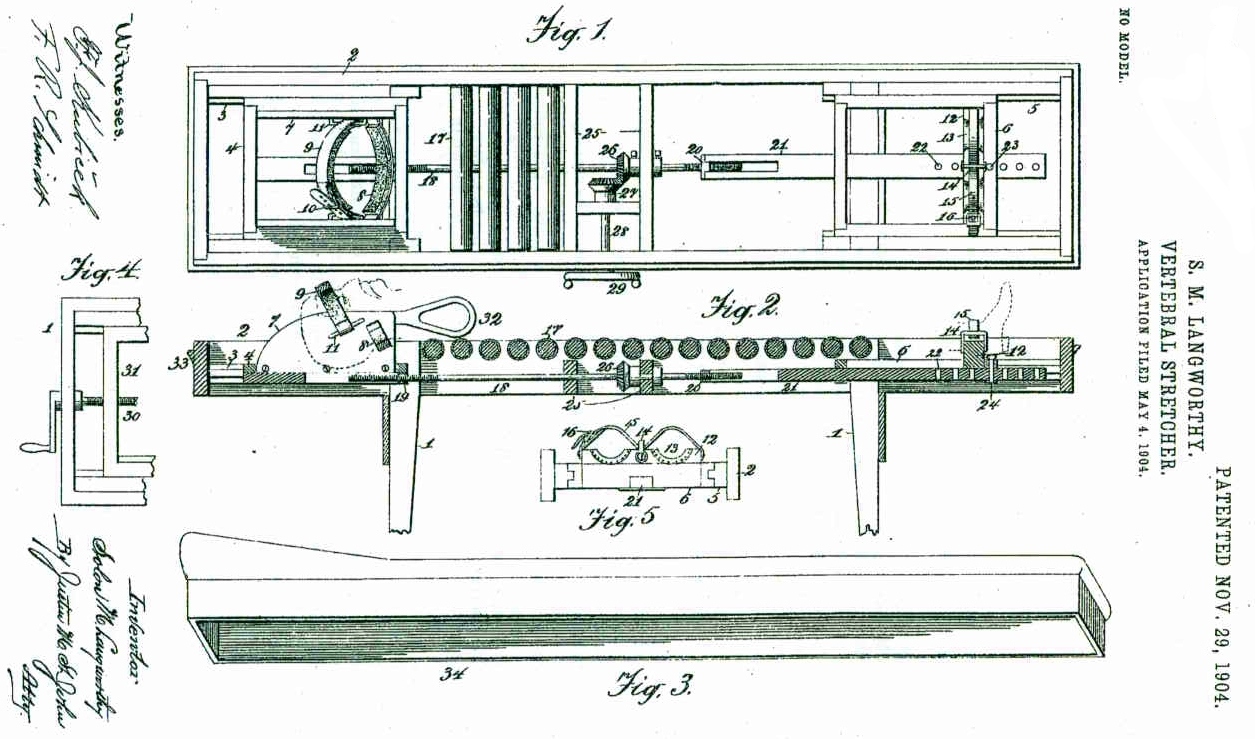
On 4 May 1904 Langworthy submitted papers to the United States Patent Office requesting a patent on his Vertebral Stretcher.10 He received the patent on 29 November 1904. The device is depicted in Figure 6. In the patent application Langworthy explains the use of the device:
"This invention relates to the treatment of the vertebral column for affections peculiar to it, and more particularly distortions or compression of the intervertebral cartilages.
The object of the invention is to provide simple, convenient, and easily-operated mechanism whereby the vertebral column may be stretched or extended and kept in that position so long as circumstances may require with a view to relieving pathological conditions due to abnormal or natural compression of the cartilages and the possible restoration of the subject to health and strength."
This device was unique in its design in that generalized distracting forces could be applied to the entire spine or only to a given area. The application of localized traction was facilitated by stabilizers that could be attached at the shoulders to allow traction to be applied only to the neck (head and shoulders stabilized) or only to the dorsolumbar spine (shoulders and feet stabilized).

Additionally, the crank-wheel that increased or decreased the traction force was placed in reach of the patient. This allowed the patient to be able to control the magnitude of the force applied to his own tolerance.
The “Amplia Thrill”
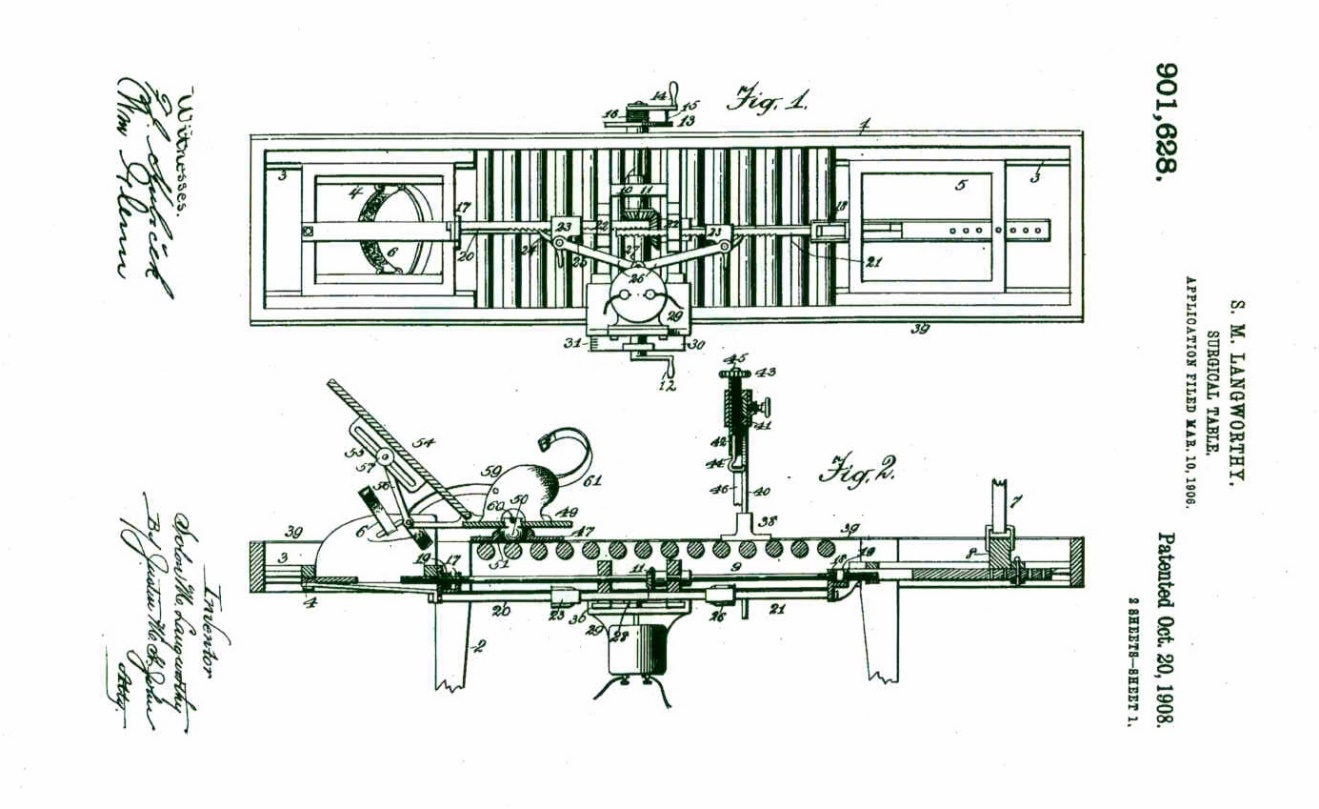
After using his original traction device for a time, Langworthy began to understand that his new invention would not allow the multitude of varying directions of force that he wished to apply to his patient’s spines. He recognized that his patient’s spines could subluxate anteriorly, posteriorly, and laterally as well as vertically. To accommodate these additional directions that he wished to push and pull the spine, he needed to modify his original design. This led to the invention of what came to be known as the “Amplia Thrill” traction device.
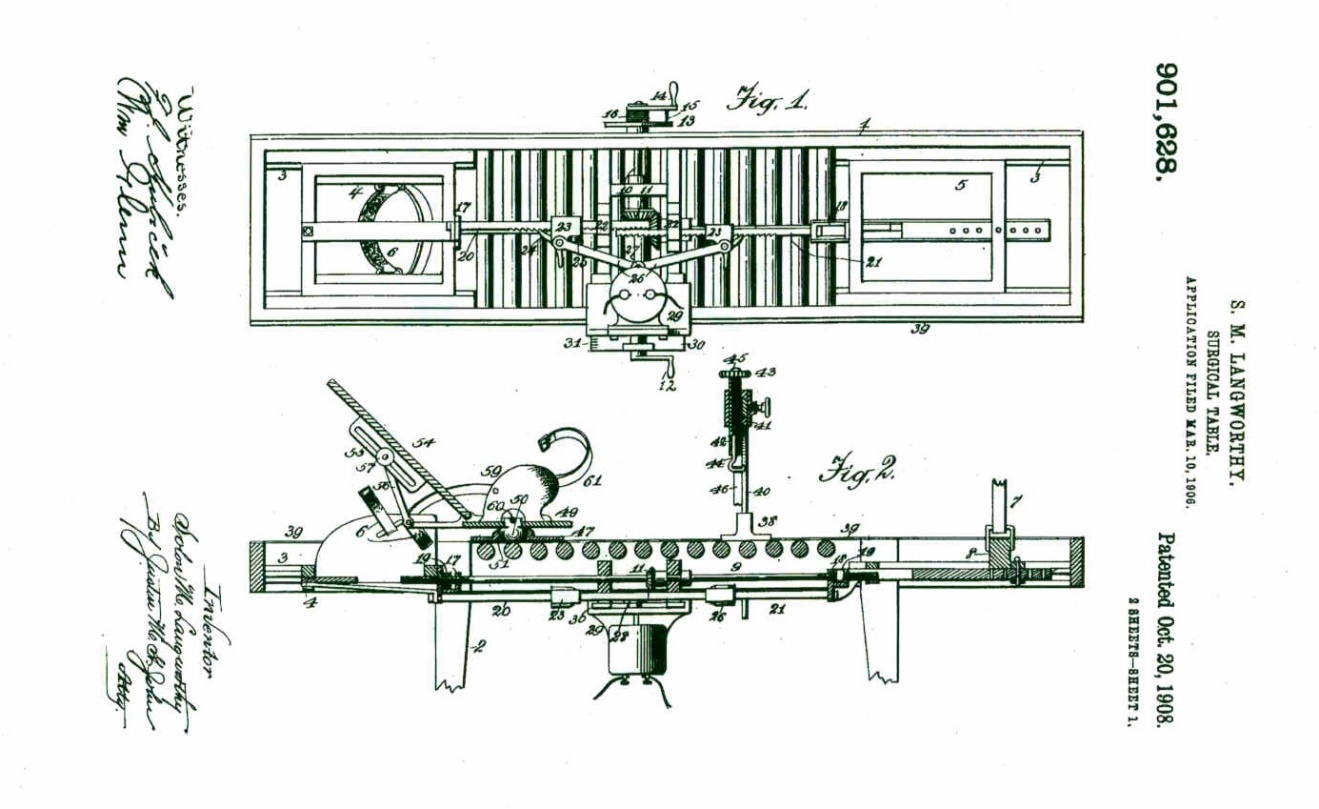
He modified his design substantially and submitted an application to the United States Patent Office on 10 March 1906. The patent was granted on 20 October of 1908.11
This new design (Figure 7) had several unique features not available on his original traction table. For instance, the head carriage would allow for movement in both directions along the long axis of the body to permit distraction and compression of the spine. Additionally, the unique harness that held the head would allow extension positioning of the skull. These were unique features that permitted the operator of the device a method by which to reduce a variety of group subluxations for which no manual method existed.
Dr. Langworthy’s methods have been largely misunderstood by the Davenport Palmers and others. For example, the authors of a chiropractic technique text12 attempted to describe the Langworthy traction methods in regards to the cervical spine. They state:
“At the turn of the century (1900), a chiropractor by the name of Langworthy began to experiment with the application of traction. He used distraction type forces on a specifically designed table and would apply manual thrusts to areas of suspected misalignment. He used these maneuvers to treat what he called ‘general compression’ which he stated was caused by a luxated or dislocated segment. His approach was generally segmental in nature and he focused on removing compressive forces from single, solitary spinal segments. He termed his traction maneuvers as extension traction; however, careful scrutiny of his work shows that by extension he meant to elongate or distract longitudinally as opposed to the anatomical reference term of extension as in backward bending. He used distraction to assist in segmental manipulation. This type of traction was not revolutionary but it was probably the first application of distraction type traction used by a chiropractor.”
The above summary of the Langworthy method is, I believe, grossly incorrect. If a true analysis of the devices, techniques, and writings of Langworthy and his disciples had been undertaken, it would have become clear that the methods and devices employed by their inventor were not simply for “general compression”, but rather, for the reduction of a variety of individual and group subluxations (multiple vertebrae misaligned together, e.g. the case of hypolordosis or kyphosis of the secondary curves of the spine) as Langworthy described in his many writings. Contrary to the above assertions, Langworthy was performing extension traction as in “backward bending” of the head and neck. In regards to anterior subluxation of the upper cervical vertebrae, Modernized Chiropractic, Volume II b4 provides the following passage:
"Specially applied traction is the most efficacious method of correcting an anterior subluxation of the atlas. The patient should be placed on the traction table venter up, the strap which passes over the forehead should be adjusted so that the head will be thrown backward on the atlas. When the pull occurs on the head by means of this head strap and the one which passes beneath the occiput, the tendency is for the condyles on the occiput to move forward on the superior articular surfaces of the atlas. This is equivalent to the atlas moving backward on the occiput. The jaw prevents any of the manual contacts from coming in contact with the anterior part of the atlas, and for this reason a posterior thrust cannot be employed in the correction of an anterior subluxation of the atlas in the same way that an anterior thrust is used in the correction of posterior subluxation of the atlas.
The straps on the traction table which engage the head are adjustable so that the head may be placed at the desired angle with the neck. The following illustration is a practical example of a case in which this special form of traction brought about the necessary change in position of the bones of the upper cervical group after other methods had failed.
Case V. The left ear had been afflicted with a stopped-up feeling for some time, when the right ear began to be affected in quite the same way. The case was one of occlusion of the Eustacian tubes from local inflammation due, of course, to the nerve disturbance from the malposition of the upper cervical vertebrae. Two treatments of fifteen minutes each by neck traction with the head held well backward by the strap, cured the trouble entirely**.**" (Author’s emphasis)
The Amplia Thrill had several other features that made it unique. A vibrating motor was attached to the underside of the table that could apply rapid longitudinal vibration while the patient’s spine was under tension.This vibratory stimulation Langworthy referred to as “Thrill.” Langworthy reasoned that the combination of these forces would have the potential for stimulating growth in compressed and thinning intervertebral discs. Interestingly, Langworthy’s theory has been at least partially validated in animal models. A recent scientific study demonstrated disc growth when distracting forces are applied to the discs of the coccygeal segments of young rats.13
A special seat-like mechanism was also incorporated into the design of the Amplia Thrill with a special stabilization belt to hold the pelvis firmly in place. This allowed the chiropractor the opportunity to be able to reduce frank dislocations of the femur from the acetabulum of the pelvis.11
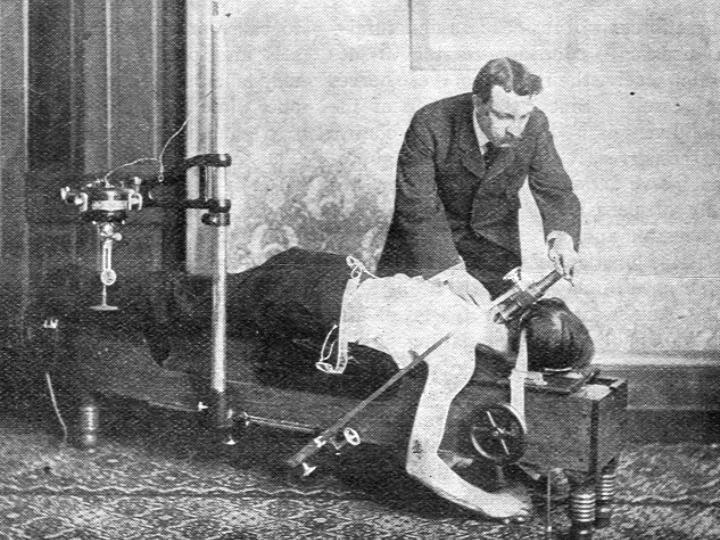
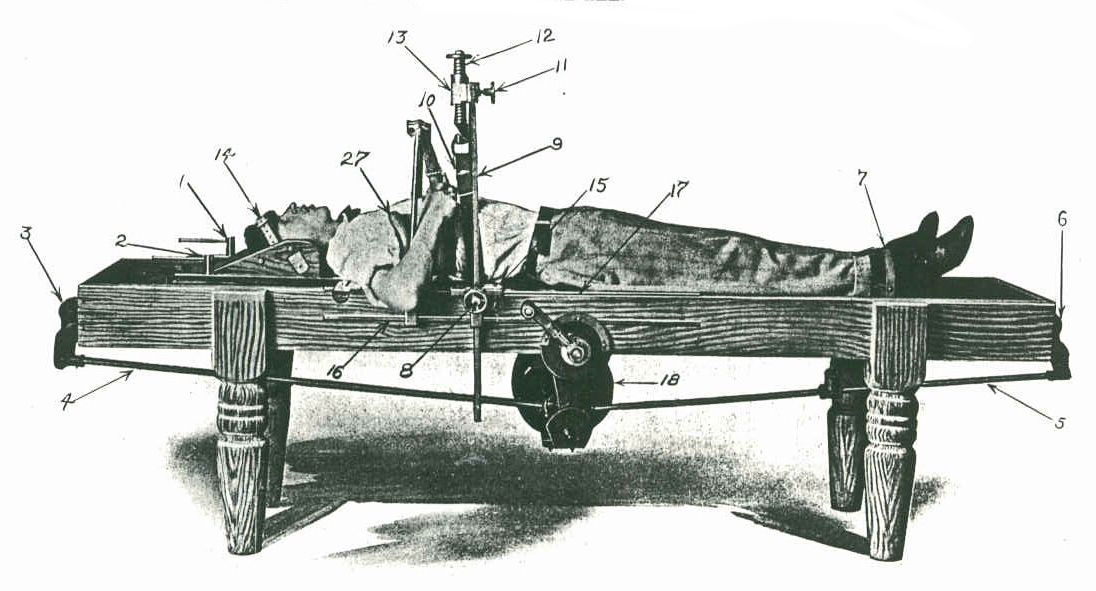
Finally, Figure 8 depicts one of the most interesting features of the Amplia Thrill traction table. A semi-circular yoke was attached to the table on tracks that would allow the yoke to move along the length of the table. The yoke could be locked into place anywhere along the table at the discretion of the operator. Attached to the semi-circular yoke was a moveable slide fitted with a large tubular screw. At the end of the screw, a leather strap was threaded through an opening to create a loop. This looped strap or girth could encircle the body anywhere along the length of the table due to the fact that the semi-circular yoke could be moved on the tracks attached along the side of the table. By turning the tubular screw, the thorax, lumbar spine, or pelvis could be pulled laterally or upward at any angle. This would allow a sustained force to be applied to reduce antalgic postures observed in acute low-back injuries or to apply extension (as in backward bending) traction forces to the lordotic curve of the lumbar spine, while simultaneously applying longitudinal traction. Figure 9 depicts the Amplia Thrill with a patient receiving this very type of thoracolumbar extension traction.


By 1909 Langworthy had established a new company to produce and sell his inventions to the chiropractic profession. This company was known as the Physicians Apparatus Company.14 The cover of the company’s catalog of products is shown in Figure 10.

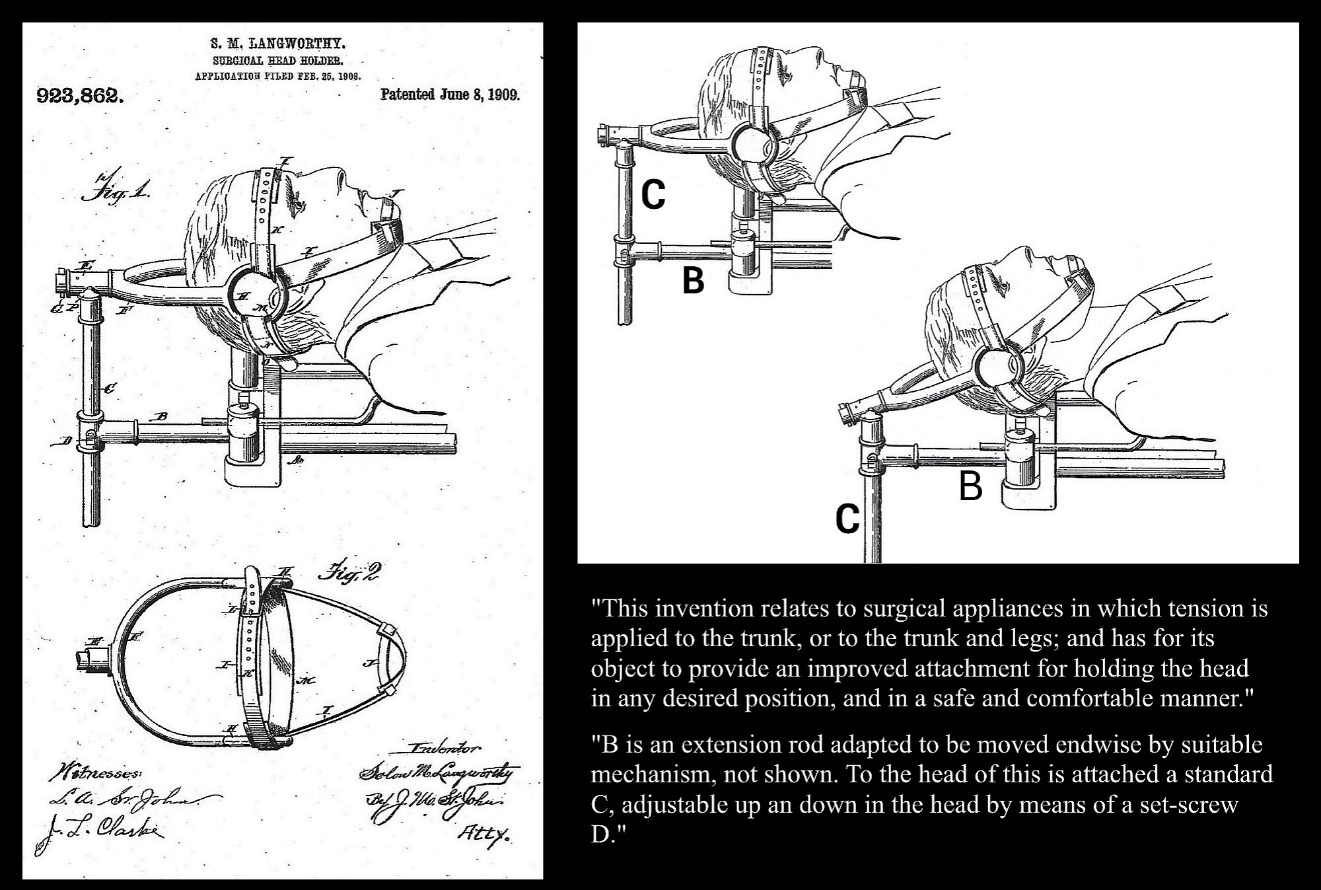
Langworthy continued to innovate and improve his adjusting tables and spinal traction devices. Figure 11 shows his 1909 patent for his “Surgical Head Holder.”15 This device was incorporated into many of his cervical traction tables and allowed for multiple positions to provide traction forces that could correct the many subluxation configurations Langworthy and his associates described in their writings.3,4 In the catalogue of his inventions,14 he states:
“The new head pull is a distinctive feature. It may be raised or lowered as desired. It may be rotated to either side and locked at any point or angle. The head harness is so arranged that the pull is divided equally between the three points, forehead, chin and occiput.”

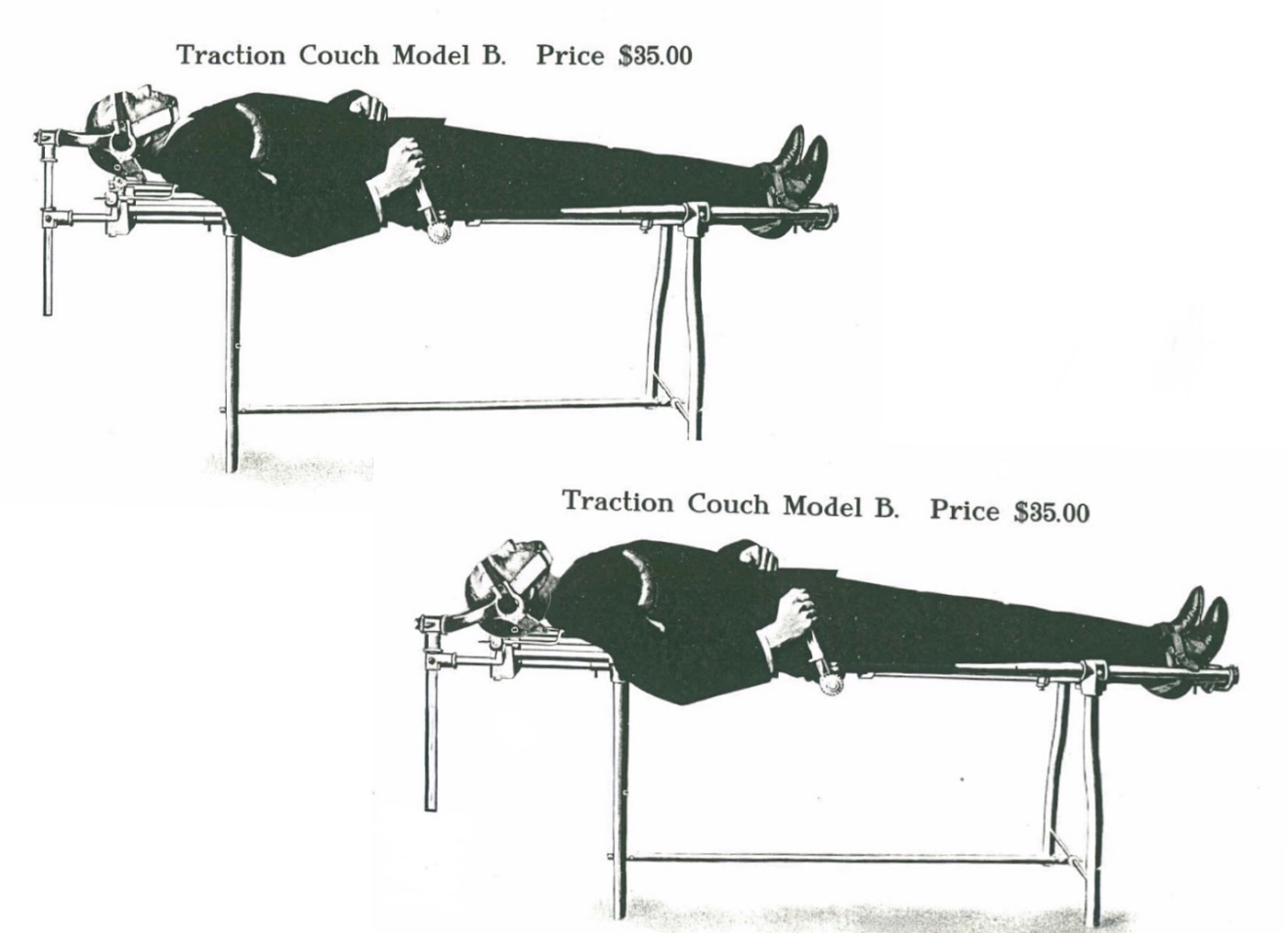
Figure 12 illustrates the Model B version of one of his traction devices in the neutral and extension positions. As described above, traction could also be accomplished in flexion and axial rotation positions, as well.

Conclusion
Solon Massey Langworthy occupies an important place in the early evolution of chiropractic technique and clinical instrumentation. His inventions reflected a sophisticated mechanical and biomechanical understanding of spinal function that differed substantially from the dominant chiropractic theories of the era. Through the development of traction systems, instrument-assisted adjusting methods and specialized treatment tables, Langworthy sought to expand the therapeutic possibilities available to the chiropractor beyond manual thrust procedures alone.
The concepts embodied in his devices, including sustained traction, multidirectional force application, patient positioning and vibratory stimulation, demonstrate an early appreciation for the complex mechanical behavior of the spine and its surrounding soft tissues. Many of these ideas share conceptual similarities with later developments in spinal rehabilitation and contemporary traction-based therapies.
Although Langworthy’s methods were controversial within the professional climate of early chiropractic, his inventive contributions represent a significant chapter in the technological history of the profession. Reexamination of his work provides a valuable historical insight into the diversity of thought that characterized chiropractic’s formative years and highlights the important role of innovation in the continuing evolution of spinal care.
Disclosure
Portions of this manuscript were edited with the assistance of ChatGPT (OpenAI), an AI language model. The tool was used for language refinement and organizational suggestions. All historical claims, interpretations and citations were researched, verified and authored by the human contributor, who retains full responsibility for the accuracy and scholarly integrity of the work.