Introduction
The American Public Health Association (APHA) is composed of a diverse group of public health stakeholders, including healthcare providers, researchers, and policymakers. Since 1872, the APHA has served as a leading voice in public health advocacy in the United States.1 Chiropractors have been formally engaged with the APHA since 1983, following the creation of the Special Primary Interest Group, “The Chiropractic Forum.”2 In 2025, the Chiropractic Health Care (CHC) Section celebrated its 30th anniversary as a Member Section.3
Each year, APHA Member Sections develop and propose policy statements addressing timely and relevant public health issues.4 These statements are reviewed and voted on by the Governing Council and, if adopted, become official APHA policy. The policy statements include action steps describing implementation strategies to directly influence a problem at hand, structured in a way which follows a specific, measurable, achievable, and time sensitive approach.5 Once adopted, they serve as guiding documents to inform public health regulation, policy, and legislation at local, national, and global levels. Adopted policy statements are available in a public-facing, online database that is hosted on the APHA’s website.6
Chiropractic medicine aligns closely with public health priorities in the realms of prevention, functional improvement, and conservative care. The American Chiropractic Association (ACA) defines chiropractic as “a health care profession that focuses on disorders of the musculoskeletal system and the nervous system, and the effects of these disorders on general health. Doctors of Chiropractic (DCs) practice a conservative approach to health care that includes patient examination, diagnosis and treatment. DCs have broad diagnostic skills and are also trained to recommend therapeutic and rehabilitative exercises, as well as to provide nutritional, lifestyle and dietary counseling.”7 From a global perspective, the World Federation of Chiropractic (WFC) defines the profession as “a health profession concerned with the diagnosis, treatment and prevention of mechanical disorders of the musculoskeletal system, and the effects of these disorders on the function of the nervous system and general health”8 Together, these definitions reflect the profession’s broad potential for engagement in public health, both in the United States (US) and internationally.
A wide range of public health issues intersect with chiropractic medicine. For example, accreditation standards for chiropractic education in the US include meta-competencies in health promotion and disease prevention.9 Additionally, leaders in the profession have identified several public health topics of importance to chiropractors, including injury prevention, occupational health, chronic disease prevention, and physical fitness.10–12 More recently, Madigan and colleagues published a comprehensive summary of public health competencies for chiropractors.13 These competencies emphasize the recognition of musculoskeletal disorders as significant public health issues, their association with other noncommunicable diseases such as obesity, and their economic impact (Table 1).13
The objective of this study was to review the APHA policy statement database for policies relevant to the chiropractic profession. To our knowledge, there is only 1 previous study analyzing the APHA policy database and this study was limited to policies related to maternal and child health.4 An assessment of which APHA public health policies in alignment with chiropractic scope of practice which the profession may assist in enacting has yet to be conducted.
Methods
The study design was guided by a similar cross-sectional study published in 2022 reviewing policies relevant to the APHA Maternal and Child Health (MCH) section.3 One of 5 investigators identified the policies to be included. The other 4 investigators served as secondary reviewers or tie breakers. Policies were coded as either having a primary or secondary focus on MCH and then grouped into qualitative themes.3
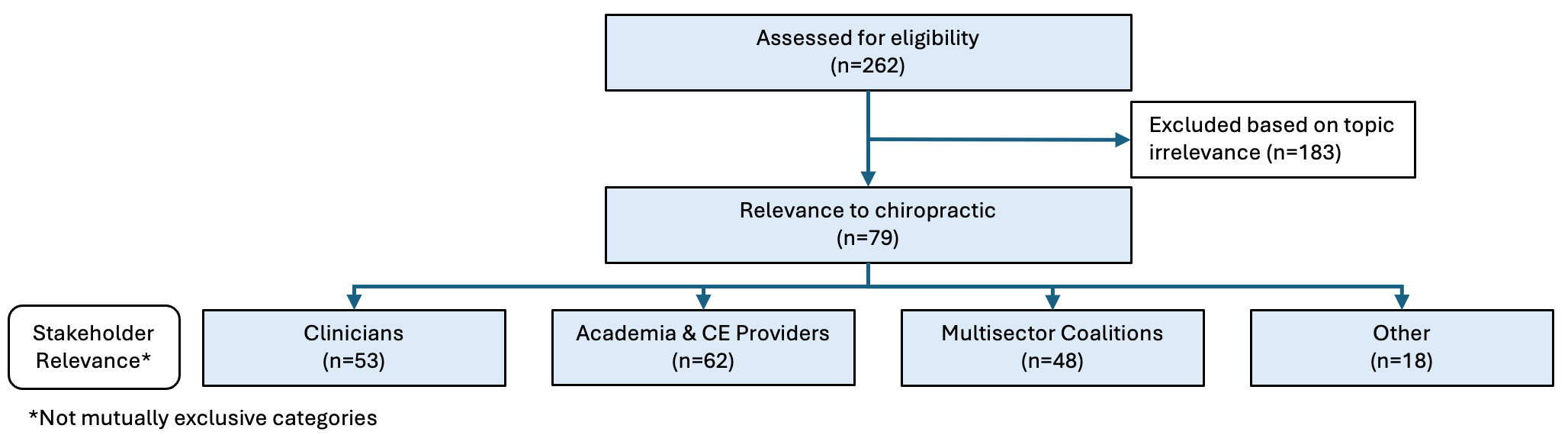
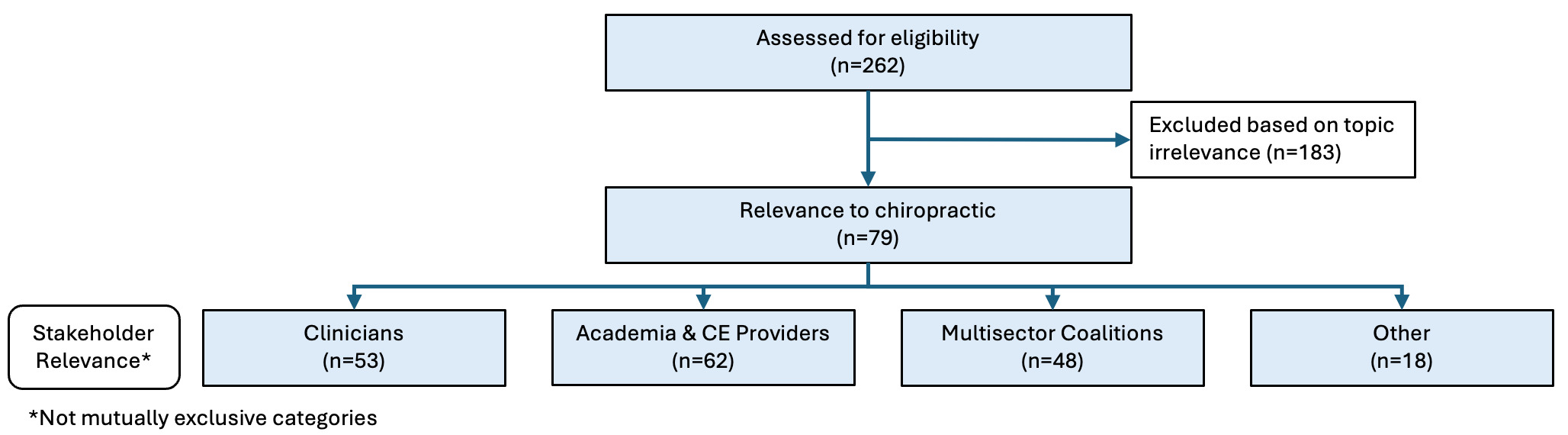
Policy statements for this current study were similarly sourced from the publicly available APHA policy statement database.6 At the time this study began, in January 2024, all APHA policies adopted in 2003 and before were archived. Policies adopted between 2004 and 2013 were scheduled to be archived in 20 years and those adopted in or after 2014 were scheduled to be archived in 10 years. Policies were therefore deemed eligible for inclusion if they were active and not scheduled to be archived in 2024 (i.e. those adopted between 2005 and 2013 and between 2015 and 2023) and had full-text availability confirmed (Figure 1). Titles from all included policies (n=262) were copied from the APHA website into a Microsoft Excel sheet (Supplementary File).
The first phase of the study was conducted by 3 investigators (MRP, SMS, KLW) with 28 years of combined experience in clinical practice, education, and research. The investigators screened the action steps of the included policies for relevance to the chiropractic profession. To ensure the reliability of the screening process, a sample of policies from 2004 and 2015 (n=29) were reviewed by the 3 investigators previously mentioned. Each investigator marked in their own independent Excel Sheet whether or not at least 1 action step for each policy statement was directly relevant to the chiropractic profession. The investigators chose the 2005 and 2015 policies to review first as these were set to be archived in 2025. The 3 Excel sheets were compared and disagreements were discussed. The screening team clarified that relevance included situational relevance to chiropractors in clinical practice and chiropractic-invested stakeholders (such as academics and advocacy groups). This process was repeated with a sample of policies from 2006 and 2016 (n=29). After reliability (>75% average agreement) was established, the 3 investigators double checked their reliability on 6 policies from 2013 and then divided the remaining policies (198) equally for independent review.
To further evaluate policy relevance to the chiropractic profession, a secondary phase was conducted to compare the action items from policies identified in Phase 1 as being relevant with chiropractic education public health competencies9 and the ACA’s definition of chiropractic. The second phase of the study was performed by MRP, KLW, VAB, and ZES (with similar experience in clinical practice, education, and research as phase 1 investigators). The ACA definition was chosen instead of the WFC definition since this study was focused on policies developed in the US. Reviewers independently determined if the ACA definition was met with each policy statement and then met to compare reliability, similar to phase 1. Additionally, each policy statement was evaluated to determine whether its action steps addressed 2 or more of the Madigan et al. competencies (Table 1 and 2).13 A minimum of 2 competencies was selected to reflect a broader scope of public health engagement and professional development. Lastly, the analysis aimed to identify the most appropriate stakeholder groups within the chiropractic profession for addressing the relevant action steps. Groupings of situational relevance that emerged from the Phase 1 data analysis were refined in Phase 2 to include 1) Clinicians (focusing on contributions to preventive screening, community outreach, and patient care); 2) Academic Institutions and Continuing Education Providers (relevant to institutions and educators offering additional public health training for chiropractic professionals); 3) Multi-Sector Coalitions (emphasizing collaboration between chiropractic professionals and other sectors to advocate for public health initiatives); and 4) Other (policies not fitting within the predefined categories but still relevant to chiropractic public health interests).
Descriptive statistics were used to summarize the data, including frequencies of policy statements meeting the ACA definition and Madigan et al. competencies13 and the distribution of policies across chiropractic stakeholder groups.
Results
At the time of data retrieval, a total of 262 active policy statements were identified from the APHA policy statement database with full-text availability. For phase 1, screening process, the average agreement for 3 pairs of investigators regarding the chiropractic relevance of APHA policy statement action steps was 68% for the first 29 policies reviewed, 79% for the second group of 29 policies reviewed, and 78% for the third group of policies reviewed (n=6). Of the 262 active policy statements, 79 policies (31%) were determined by the screening team to include at least 1 action step directly relevant to chiropractic practice, academic institutions, or advocacy organizations.
Among the 79 policy statements selected in phase 1, 19 (24%) were identified in the second analysis phase as aligning with the ACA definition of chiropractic practice, while the remaining 60 policies (76%) did not meet ACA definition. Seventy-six policies (96%) addressed 2 or more of the Madigan et al. public health competencies,13 while only 3 policies (4%) did not meet this threshold. Fifty-five (70%) were identified as relevant to Clinicians, 64 (81%) to Academic Institutions and Continuing Education Providers, 49 (62%) to Multi-Sector Coalitions, and 18 (23%) to Other stakeholder groups (Supplementary file).
Some examples of action steps from these 19 policy statements that aligned with both the ACA definition and addressed 2 or more Madigan et al. public health competencies13 are: 1) forming partnerships with national and state organizations to disseminate and promote the National Physical Activity Plan, 2) implement Dietary Guidelines for Americans-based public education, nutrition standards, and approaches for policies, systems, and the environment that reflect the needs of diverse populations, 3) urging the development and dissemination of evidence-based guidelines for the prevention and management of musculoskeletal disorders, and 4) encouraging the prioritization and implementation of evidence-based community and provider training programs on mental health, nonpharmacological pain treatment alternatives, substance abuse and overdose prevention.
Discussion
Although chiropractors are primarily recognized for their role in the evaluation and management of musculoskeletal conditions, they are also well-positioned to support a wide range of public health initiatives. Findings from this analysis help to identify which policies may be most pertinent to a chiropractor’s scope of practice or may align with the interests of stakeholder groups within the chiropractic profession. Over 25% of policy statements adopted by the APHA since 2005 were found to be relevant to the chiropractic profession, with the majority meeting public health competencies in the chiropractic profession.13 These findings demonstrate a broad and consistent alignment between the APHA and the chiropractic profession’s public health priorities. Identification of these congruent policies has potential to promote collaborative efforts between stakeholders in the chiropractic profession and broader public health efforts by other healthcare disciplines.
Evidence supporting the potential of chiropractors to contribute to public health is also seen in recent practice trends, research, and accreditation guidelines. Increasingly, chiropractors are being integrated into large multidisciplinary systems such as US Department of Veterans Affairs, where they contribute as part of coordinated care teams in various service lines such as physical medicine and rehabilitation, pain management, Whole Health, and emergency medicine.14–19 Chiropractors in these systems serve not only as providers of manual and rehabilitation therapies but also as team members who may help identify health concerns, make appropriate referrals, connect patients with healthcare resources, and support facility-wide public health initiatives such as annual flu vaccination20 and implementation of national physical activity guidelines. These activities are increasingly critical as part of a comprehensive response to the challenges of a rapidly aging population.21 These examples highlight the adaptability and utility of the chiropractic profession in advancing public health objectives.
The programmatic accrediting agency for chiropractic degree programs and residencies in the US, the Council on Chiropractic Education, has expanded clinical education meta-competencies related to health promotion and disease prevention in recent accreditation standards, resembling the objectives of the Madigan et al. competencies.13 In 2018, the first objective under this meta-competency was to prepare students to “Identify appropriate hygiene in the clinical environment.”11 Eight years later, in 2025, the first objective offers a more robust and comprehensive approach to public health as students are prepared to “identify the importance of primary, secondary, and tertiary prevention in population health, including health promotion, disease prevention, and screening.”12 While this study focused on chiropractic professional standards and public health policies for the US, it is worth noting that on a global scale, the WFC already recognizes chiropractors’ potential to contribute to public health in areas such as healthy aging, opioid misuse, and women’s, children’s, and adolescents’ health.22 In collaboration with the World Health Organization, WFC promotes global public health campaigns including World Spine Day, the Bone and Joint Decade’s Action Week, tobacco cessation efforts, and the Global Strategy on Diet, Physical Activity and Health.22
Public Health Implications
These findings, combined with existing examples from clinical settings and global health efforts, highlight opportunities for chiropractic involvement in advancing the broader mission of public health efforts through their scope of practice.
Limitations
This study is limited by the subjective nature of manual policy review, which, despite iterative refinement, may have introduced variability in classification. The analysis was restricted to active APHA policies, potentially excluding archived statements still relevant to chiropractic practice. Additionally, policies unavailable in full-text format were excluded, which may have resulted in the omission of pertinent content.
Relevance determinations were made through expert consensus among investigators, but no external validation was performed, which may limit objectivity. The 3 specified stakeholder groups (Clinicians, Academic Institutions, Multi-sector coalitions) do not represent all possible stakeholders for health care professions.23 The classification of action steps as “actionable” also involved interpretive judgement, which could introduce bias despite the investigators applying dual coding for about ¼ of the policies (64/262) and using inter-coder reliability to “foster reflexivity and dialogue among the research team,” an important step in content analysis as described by O’Connor and Joffe.24 In addition, the investigators tried to reduce interpretive bias by using the ACA definition and at least 2 Madigan et al competencies in phase 2 of the study to confirm chiropractic relevance of each included policy statement. Relying on the ACA definition of chiropractic practice may limit the applicability of these findings to chiropractors practicing in the US. Lastly, variability in the structure, language, and specificity of the APHA policy statements may have affected consistency in policy review.
Conclusion
This analysis highlights the meaningful intersection between chiropractic practice and public health policy. A significant number of the APHA policy statements contain actionable steps that align with chiropractic competencies and practice models, particularly in areas such as chronic disease prevention, health promotion, and equitable care delivery. The overwhelming majority of policies reviewed addressed multiple public health competencies and were relevant to diverse stakeholder groups, including clinicians, academic institutions, and coalitions.
These findings reinforce the chiropractic profession’s role in interdisciplinary health systems and its alignment with national and global public health priorities. With their education, accessibility, and increasing integration into team-based care environments, chiropractors are well-positioned to contribute meaningfully to public health strategies and initiatives. This study serves to outline a road map of opportunities which individual practitioners alongside national and state chiropractic organizations can pursue in effort to advance public health and contribute to the collaborative efforts of our healthcare colleagues from other professions.
Funding Statement
There is no funding to declare.
Author Contribution Statement
MP, SS, and KW were responsible for conceptualization; MP, VB, SS, ZS, and KW were responsible for data curation; VB and KW were responsible for formal analysis; There was no funding. MP, VB, SS, and KW were responsible for methodology; MP was responsible for project administration; VB was responsible for resources and software; KW was responsible for supervision; MP, VB, SS, and KW were responsible for validation; All authors were responsible for writing, reviewing, and editing the manuscript.
Author Disclosure Statement
Morgan Price and Samuel Schut both serve on the Academy of Site Team Visitors for accreditation on the Council on Chiropractic Education. Morgan Price and Samuel Schut both received funding (from the Veterans Affairs Central Office and the Cleveland Clinic, respectively) to attend the 2025 Association of Chiropractic Colleges Research Agenda Conference. Samuel Schut is concurrently a participant in a funded research project through the Cleveland Clinic Philanthropy #CCG0399. Victoria Bensel is concurrently supported by a generous grant from the NCMIC Foundation (this funder had no role in the funding, provision of materials, or article processing charges. Victoria Bensel received payment or honoraria for 30 hours of lecture content from the Camara Institute for Chiropractic Sciences. Krista Ward is an employee of Life Chiropractic College West and some time on the study was done while at work with permission from her supervisor. Krista Ward was funded by Life Chiropractic College West to attend and present initial findings of this study at the 2025 American Public Health Association annual conference. Krista Ward also serves as a Section Councilor for the Chiropractic Health Care Section of the American Public Health Association. Zachary Scott had no disclosures.
Abbreviations and Acronyms
APHA – American Public Health Association
ACA – American Chiropractic Association
CHC – Chiropractic Health Care Section
MCH – Maternal Child Health
US – United States
WFC – World Federation of Chiropractic
WHO – World Health Organization