


INTRODUCTION
Migraines are one of the leading disabling neurological conditions in the world, impacting over one billion individuals per year.1 Migraines can be characterized by recurrent, episodic attacks accompanied by moderate to severe head pain, often unilateral and pulsating in quality. Symptoms such as sensitivity to light (photophobia), sensitivity to sound (phonophobia), nausea, and worsening discomfort with routine physical activity can also affect those who suffer from migraines.1 In addition, migraine disorders may also have nausea and vomiting, abdominal cramps, benign paroxysmal vertigo, benign paroxysmal torticollis, and episodes of confusion. Migraines can have distinct phases, including prodrome, aura, headache, and postdrome. They can be categorized into resistant and refractory migraines, which have significant differences in treatment response.2 Migraines are common among young adults during prime years of education and career development; thus, they can affect a person socially and economically.1
Migraines are commonly managed with medication. Nonsteroidal anti-inflammatory drugs (NSAIDs), triptans, and antiemetics, may be used during a migraine. They aim to relieve pain and associated symptoms. Preventive medications include beta-blockers, anticonvulsants, antidepressants, and calcitonin gene-related peptide (CGRP) inhibitors. These may be prescribed to decrease the frequency and severity of a migraine. In addition, patients are often encouraged to make lifestyle changes such as maintaining regular sleep schedules, controlling stress, and identifying any other triggers. Migraines are a multifactorial neurological condition that can be associated with various risk factors and comorbid conditions; therefore, researchers stress the importance of a comprehensive and multidisciplinary management approach to improve long-term outcomes.3
Although pharmacological therapies are a popular migraine treatment, many patients experience incomplete relief, side effects, or concerns regarding medication overuse.4 Because of these issues, some patients seek complementary approaches such as chiropractic care, inlcuding upper cervical care, which focuses on the alignment and function of the first vertebrae of the neck and its relationship to the nervous system. The upper cervical spine surrounds the brainstem and plays a role in neurological communication and blood flow between the brain and body. Misalignment in this region may contribute to irritation of the surrounding nerves and muscles that can affect an individual’s headaches. Upper cervical chiropractic techniques aim to restore proper alignment and reduce mechanical stressors, potentially improving nervous system function and decreasing migraines. Some case reports and emerging research suggest that patients receiving upper cervical care experience reductions in migraine frequency, severity, or duration.5
Other treatment options for migraines are light therapy and therapeutic ultrasound. They have both been shown to be beneficial for managing migraines. Therapeutic ultrasound to the craniocervical and upper cervical regions in the pulsed form have been found to decrease how often migraines occur, lessen intensity, and reduce the level of disability.6 Additional studies reviewed by Ting-Wei Hou and colleagues report that controlled light therapy can reduce migraine frequency and severity. Further benefits such as improved sleep quality and decreased anxiety were also noted.7 These passive modalities may complement traditional migraine treatments by addressing the musculoskeletal component of a migraine. The goal of this case report is to describe the management of a patient with chronic migraines using upper cervical Toggle adjustments, ultrasound, and red-light therapy.
Case Report
History
A 24-year-old woman sought care for a primary complaint of constant headaches. The headaches were described as debilitating. They prevented her from driving, which caused her to move her college classes online. Associated symptoms included digestive disturbances, respiratory difficulty, numbness, and tingling in the left arm, and nightly sleep disturbances due to the pain. She was also diagnosed previously with psoriasis and vagal nerve dysfunction by her primary care physician. She was experiencing flare-ups that contributed to systemic inflammation. She also experienced lightheadedness, inflammation, fight or flight responses, body pain, breathing, and digestive issues. She previously visited the emergency department for these symptoms, and no cardiac pathology was identified. A nurse practitioner referred to her for upper cervical chiropractic care.
Her medical history included irritated bowel syndrome (IBS), psoriasis, anxiety, and depression which were all diagnosed by her primary care physician. She reported ongoing psychosocial stress related to school, work, and daily life. Previous medical evaluations attributed her migraines to anxiety and stress. Her doctors recommended NSAIDs for her migraines. She was, however, taking metoprolol for heart palpitations and fluoxetine for anxiety, with plans to discontinue the latter and she didn’t want to take any additional medications than necessary.
Physical Examination
Vital signs were within normal limits: blood pressure 97/64 mmHg, pulse 65 bpm, oxygen saturation 99%, weight 138 pounds, height 5’6, and BMI 22.3. Jackson’s foraminal compression, maximal foraminal compression, cervical distraction, Bikele’s test, Bakody’s test, Valsalva’s, and shoulder depression tests were all negative. Muscle strength testing C5-C8 scored 5/5. Deep tendon reflexes C5-C8 scored 2/4.
There were no significant diagnostic challenges. Differential considerations included tension-type headache, cervicogenic migraine, and cervico-cranio syndrome (upper cervical subluxation/instability). The presence of cervical and neurological signs, autonomic symptoms, and family history of migraines supported a working diagnosis of cervicogenic migraine, with upper cervical dysfunction as a likely contributing factor, guiding the initiation of chiropractic care.
Standardized outcome tools were used at each re-exam to track the patient’s progress. The Visual Analog Scale (VAS) was employed to quantify pain intensity; she originally scored a 9/10. The Neck Disability Index (NDI) was used to evaluate functional impact which she scored 34/50 initially.
Chiropractic Examination
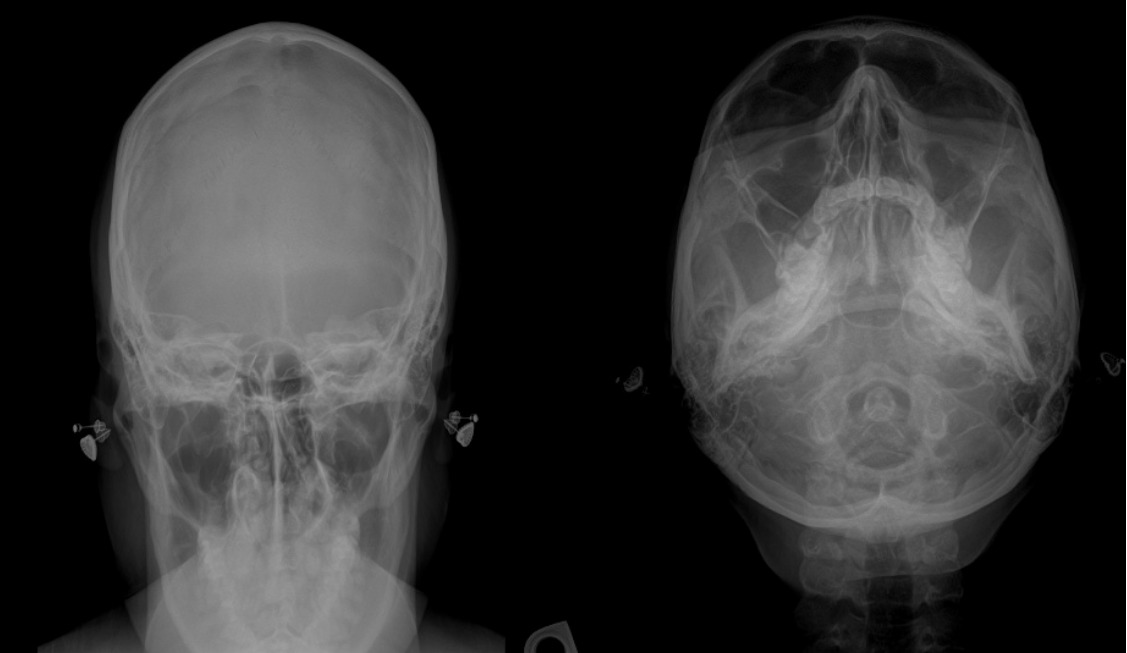
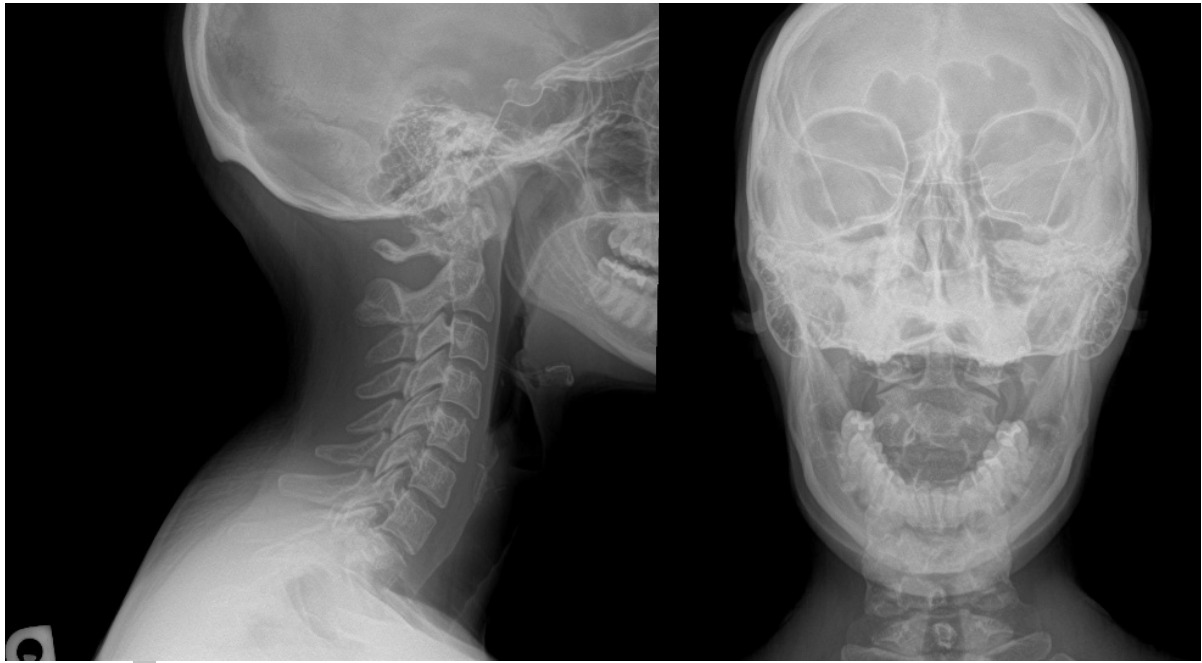
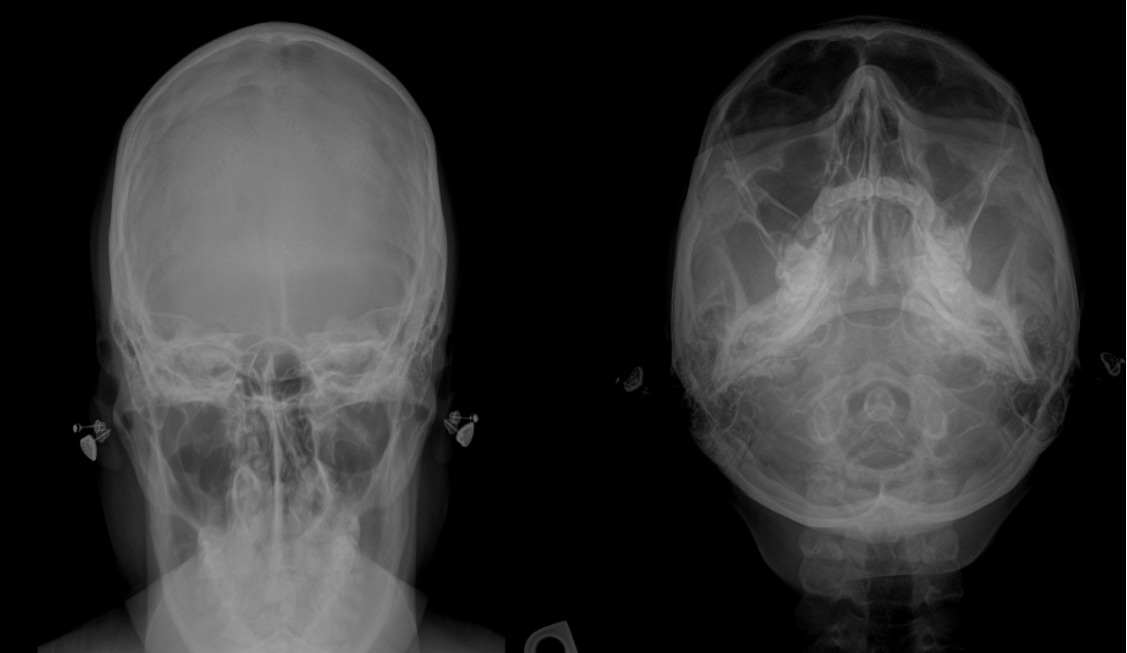
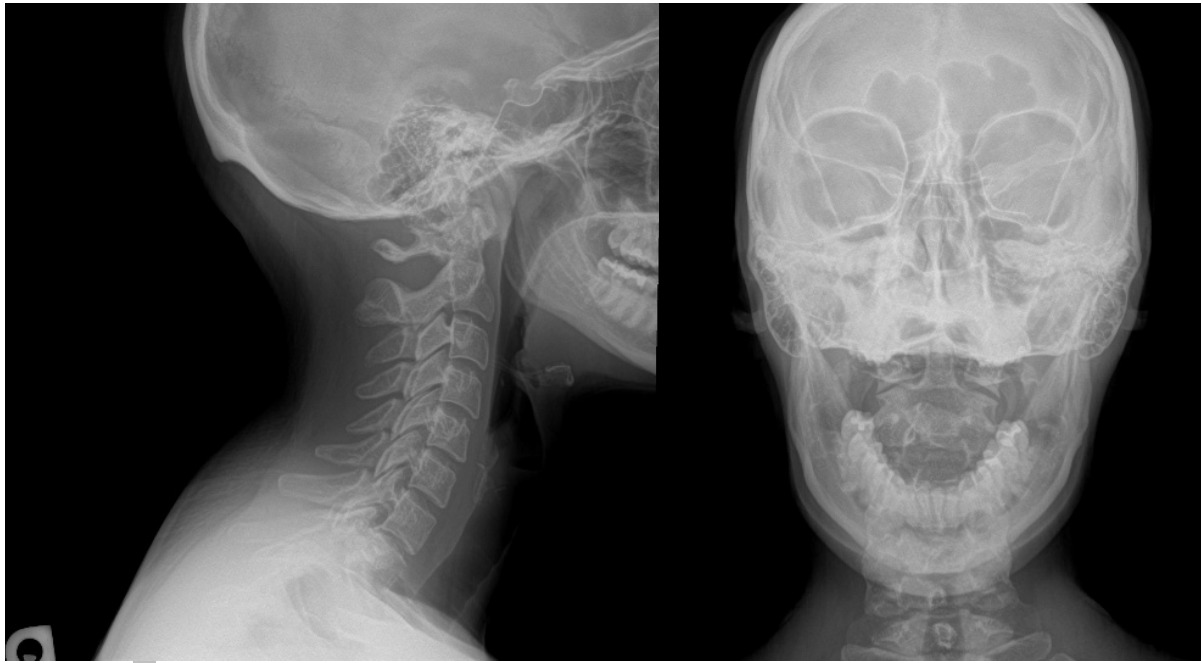
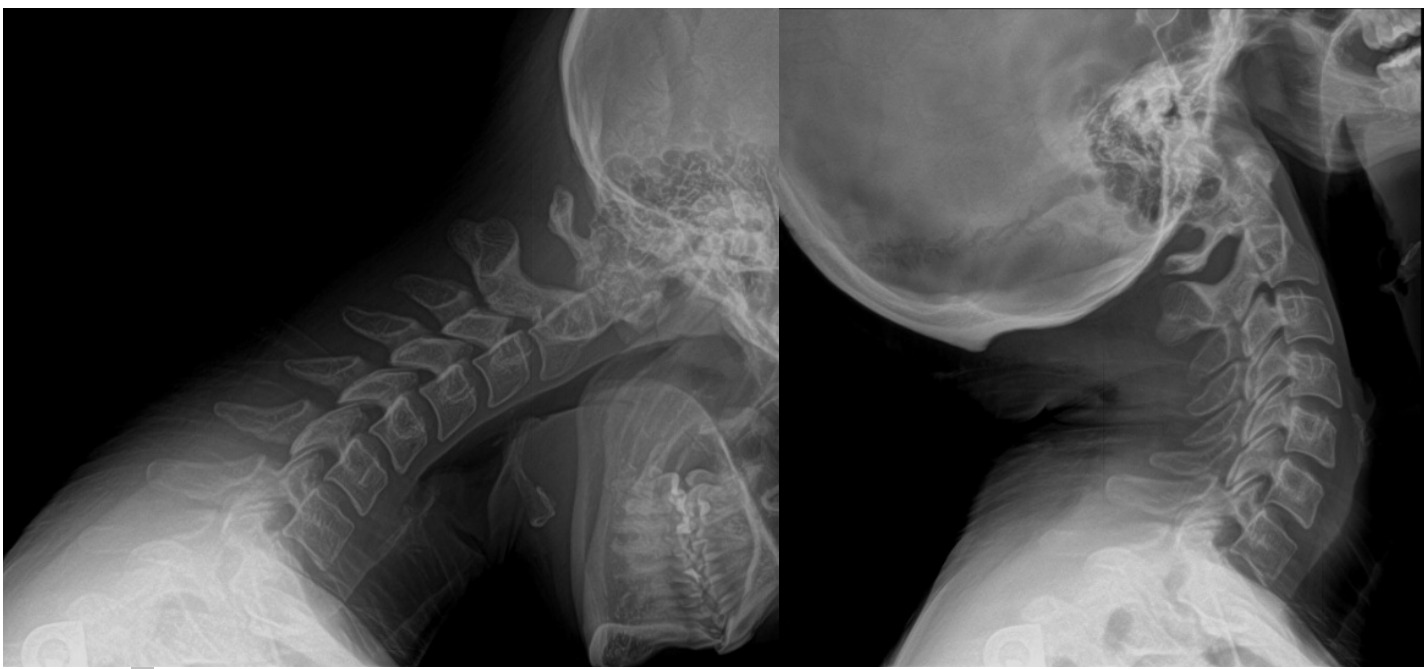
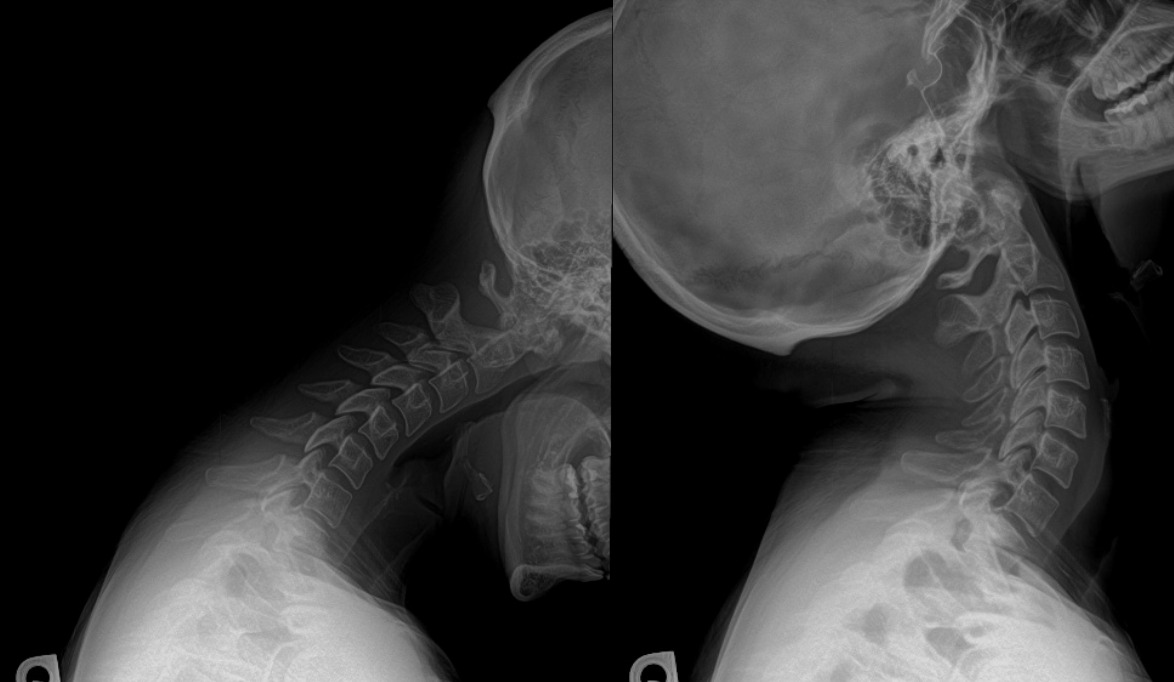
She had decreased active range of motion in her cervical spine in all planes of motion. Flexion was measured at 38 degrees, extension was 48 degrees, left rotation was 68 degrees, right rotation 62 degrees, left lateral bending was 32 degrees, and right lateral bending was 29 degrees. Static palpation revealed tight upper trapezius and suboccipital muscles. Upper cervical radiographs were taken to derive a listing for her Toggle adjustment. (Figures 1-3) Chiropractic radiographic analysis revealed that her atlas vertebra was fixated anterior, superior, and to the left in relationship to the occiput. A Tytron thermography scanner was used to determine areas of abnormal temperature fluctuation which could be an indicator of nervous system dysfunction.8 This instrument detects changes in temperature. Supine leg checks were also utilized.
Management
The care plan was created to follow a 12-week program of upper cervical chiropractic management using the Toggle technique along with ultrasound and red-light therapy after the adjustments. During the initial 2 weeks, she was seen 3 times per week, followed by twice weekly for 2 weeks, weekly visits for 4 weeks, and every other week for the final 4 weeks. A re-examination with repeat cervical radiographs was performed at the 4-week mark to monitor structural and functional progress, providing objective feedback to guide continued care. This multifaceted approach was intended to address not only musculoskeletal dysfunction but also neurovascular and autonomic contributors to the patient’s migraine presentation. Table 1 shows the patients’ progression through care.
The patient received the Toggle technique as an adjustment treatment plan. She received a side-lying high-velocity low-amplitude adjustment on the lateral aspect of the atlas transverse with a headpiece that had a drop when the thrust was applied (see figure 4). The thrust is described as a quick set and release adjustment with a recoil. The goal of using this specific upper cervical technique was to help correct cervical joint dysfunction and reduce nociceptive input.8 No other adjustments to her spine or extremities were made during her visits. She received an adjustment if her Tytron reading showed that she was not adapting and therefore could benefit from an adjustment. On the visits where she was adapting according to the Tytron scan, she received the red-light therapy or ultrasound treatments.

Passive care was also incorporated at each visit; therapeutic ultrasound of the paraspinal and suboccipital musculature for 7 minutes at 2 W/cm2 to decrease soft tissue irritation and red-light therapy for 7 minutes in the upper thoracic and cervical spine to promote local circulation and tissue repair. The patient was instructed to do 3 cervical neck exercises known as “slow motion head rotation,” “Forward Head Jaunt,” and lateral bending stretches. These were introduced at the 4-week mark and were done by the patient at home for 3 sets each for 30 seconds.
Outcomes
At the halfway point of care at 6 weeks, outcome measures and functional assessments demonstrated meaningful improvement. The patient’s VAS scores decreased from 9/10 to 5/10. The NDI improved from 34/50 to 22/50. Migraine frequency was reduced from 3 times a week to 2 times a month. Cervical range of motion testing showed measurable gains range of motion in the neck. Flexion was measured at 42 degrees, extension was 50 degrees, left rotation was 71 degrees, right rotation 67 degrees, left lateral bending was 35 degrees, and right lateral bending was 33 degrees which showed improvement in ranges of motion from her initial assessment. Muscle palpation revealed decreased hypertonicity in the suboccipital and trapezius regions. These improvements supported the working diagnosis of migraine with a cervicogenic component and indicated that the treatment plan was working well. A final reassessment at twelve weeks further reinforced this trajectory, with VAS scores reduced to 3/10, NDI decreased to 10/50, and migraine frequency limited to one episode per month. The patient stated that she no longer had IBS symptoms or autoimmune flares. Because of her improvements, the frequency of her visits were stretched out to once a month. Questionnaires showed secondary improvements in musculoskeletal comfort as well. She also reported better sleep quality. Together, these outcome measures provided both subjective and objective evidence of clinically significant gains, further reinforcing the role of upper cervical chiropractic care along with red light therapy and ultrasound in reducing migraine burden and improving overall function. Table 2 shows the patients’ outcomes at various time points.
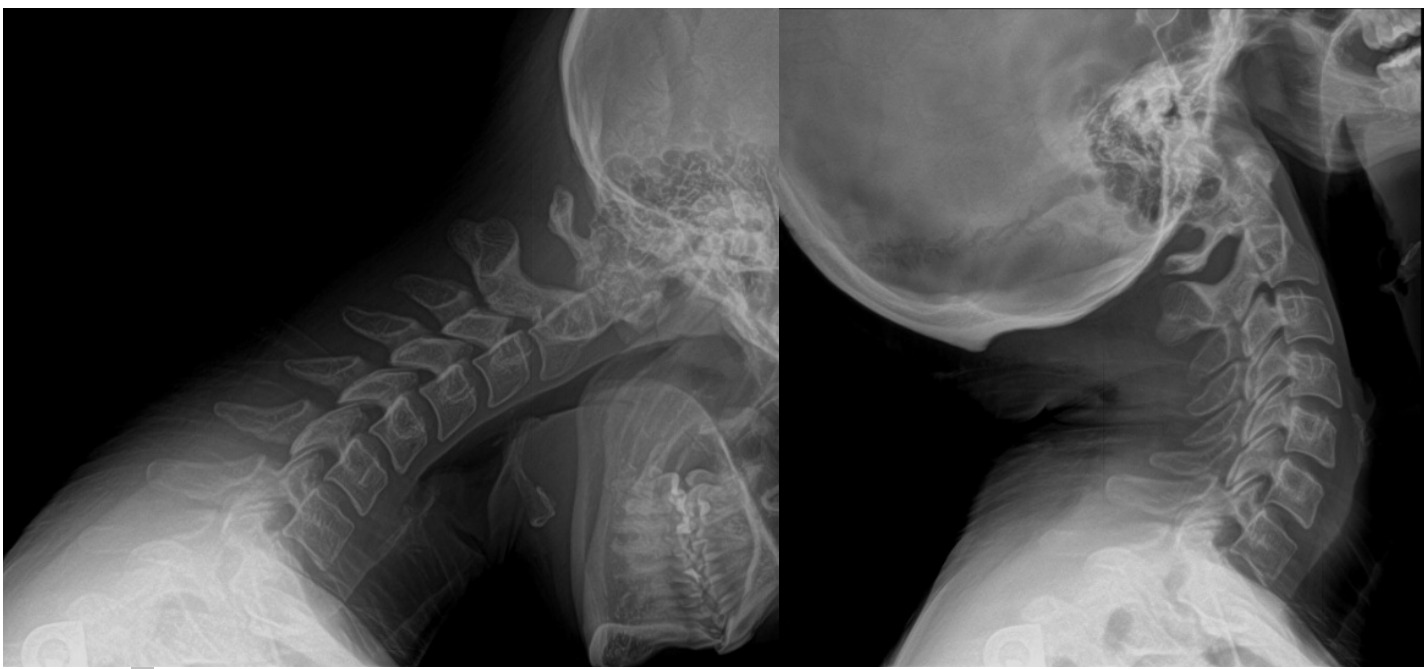
Additionally, she showed improved segmental alignment through increased cervical lordosis and confirmed progress toward her therapeutic goals (figures 5 and 6).

DISCUSSION
This case report highlights the potential benefit of upper cervical chiropractic care as part of a multidisciplinary approach to managing chronic migraines in a young adult. In working with the patients’ primary care physician (PCP). We gained insight into the patient’s history of psoriasis, tachycardia, arrhythmia, subclinical hypothyroidism (lab results indicated elevated TSH), and general anxiety/depressive disorder. These conditions may have also had an impact on her migraine intensity and frequency. The PCP also informed us that the patient was taking 12.5 mg/day dosage of Metoprolol succinate ER (extended release) for irregular heart rate and rhythm. This type of medication is known to cause headaches, dizziness, and fatigue as side-effects. Knowing this information and working closely with the patient’s PCP may help a chiropractor decide on the best course of action. Her PCP recommended treatment with upper cervical chiropractic care to manage her migraines. The literature suggests that interprofessional collaboration among providers can lead to better health outcomes. A systematic review of 36 studies demonstrated the importance of working with other health care professionals and revealed better care for the patient.9,10 The patient’s PCP and her chiropractor in our study worked closely together to help provide the best care for the patient.
Posazski et al conducted a systematic review to identify the effects of spinal manipulation on patients with migraines. Six studies met the inclusion criteria, with 645 patients total. The results showed that spinal manipulation reduced disability scores as well as the number of days with a migraine. The studies were small with limited follow-up but promising. Our study shows similar results to the current literature analyzed in the systematic review, because her disability scores went down significantly as did the frequency of her migraines.11
As a result of the complexity of migraines, collaborative care remains crucial for best practices and long-term management. Continued communication with the patient’s primary care physician helps ensure continuity of care, particularly regarding monitoring for comorbidities such as anxiety, depression, or hormonal influences. Collaborative strategies could include sharing progress notes and outcome measures with all providers on the patients’ healthcare team. Furthermore, co-developing a management plan that integrates conservative chiropractic care with medical oversight as well as providing ergonomic, lifestyle, and stress-management recommendations that complement the current treatment from the providers. The chiropractor’s role in this team setting is to optimize musculoskeletal and nervous system function, reduce triggers, and contribute ongoing objective outcome data. These measures can help to enhance the collective decision-making process, ensuring that care remains safe and patient centered.
A key strength of the case lies in its structured use of validated outcome measures, including the Visual Analog Scale (VAS) for pain intensity and the Neck Disability Index (NDI) for functional status. These tools provided a quantifiable means to track progress over time and demonstrated clinically meaningful improvements in both frequency and severity of migraines. Furthermore, the repeated objective reassessments, including cervical range of motion testing palpation of muscular tension, and structural improvements in lordosis on the x-ray further strengthen the validity of observed changes by correlating patient-reported outcomes from the VAS and NDI with physical examination findings.
Another strength of this study is the integration of both passive and active interventions. However, it is hard to say whether one intervention helped more than the other or if they had to be used in conjunction for the results the patient had. Future studies could investigate using just passive care modalities or just Toggle technique alone.
Furthermore, through addressing multiple areas of the patient’s health, the treatment plan allowed care to be comprehensive and individualized to get the maximum results.1 Furthermore, the absence of adverse events during care further supports the potential for chiropractic treatment to serve as a safe conservative option, provided appropriate screening and monitoring are in place. Ultimately, this case reinforces the value of outcome-based, patient-centered care and suggests that chiropractic interventions may play a supportive role in managing migraines, particularly when integrated with collaborative care with other health care providers.
The rationale for the conclusions drawn in this case relies on both clinical observation and existing evidence suggesting that cervical dysfunction and musculoskeletal tension can serve as migraine triggers.12 The patient’s significant reduction in headache frequency and disability, paired with improvements in cervical mobility and muscle tone, aligns with the hypothesis that addressing cervicogenic contributors may alleviate migraine burden.
Limitations
As a single case report, the findings cannot be generalized to all migraine patients, nor do they establish causation between chiropractic care and the observed improvements. Furthermore, the patient also received red light therapy, ultrasound, and active care stretches, so it is hard to say if one of these treatment approaches helped more than the others or if they are all required in conjunction.
CONCLUSION
Chiropractic care combining using the upper cervical Toggle adjustments, red light therapy, ultrasound, and at-home cervical neck exercises may reduce migraine frequency, disability and improve quality of life in those who suffer from migraines, especially when a cervicogenic component is suspected.
Consent
The patient provided written informed consent. IRB approval was also obtained from Palmer College of Chiropractic.
Acknowledgments
I would like to sincerely acknowledge Dr. Jared Wayland, DC for this patient referral.