
Introduction
Neuropathy, as defined by the Oxford Dictionary, is “disease or dysfunction of one or more peripheral nerves, typically causing numbness or weakness”. While there are many causes, this paper examines a trauma-induced case. A 26-year old Caucasian man was referred for electrodiagnostic evaluation of arm pain approximately 2 months after being bitten by a lemur. Based on Seddon’s classification of peripheral nerve injury, there are 3 types that can occur: neuropraxia (Type 1), axonotmesis (Type 2), and neurotmesis (Type 3). The hallmarks of neurotmetic disease include damage to all of the layers of the nerve, including the axons, endoneurium, perineurium, and epineurium.1,2 Additionally, EMG examination of patients with this classification of neuronal injury shows acute denervation, with nerve deficits that may remain for a year or more. Regeneration of neurotmetic damage may occur in a disorganized fashion and requires surgical repair.3
While there are many cases of general neuropathy in the literature, this case demonstrates an interesting pathogenesis of the condition while highlighting how such a condition is objectively diagnosed.
Case Report
History
A 26-year-old man was referred to a chiropractic neurologist by his attending orthopedic surgeon for electrodiagnostic studies to evaluate a suspected peripheral neuropathy following a lemur bite, as well to determine the etiology of his complaints. The studies referenced in here were performed 2 months after the traumatic incident occurred at an animal sanctuary. The patient’s chief complaint was pain and paresthesia of the right upper extremity. The pain began at the right distal anterolateral aspect of the arm and had a “scraping and burning” quality. It was constantly present and varied between 1-6/10 in severity. There was radiation extending into the lateral forearm and dorsal aspects of the 1st and 2nd digits of the hand. Paresthesia was also identified along the same distribution. Heat and sunlight increased symptoms and nothing seemed to help it get better.
Since we had a working diagnosis of traumatic peripheral neuropathy, we performed nerve conduction studies with needle electromyography to identify the suspected pathology.

Physical Examination
Peripheral sensitivity testing, utilizing a Wartenburg pinwheel, was graded as equal in character bilaterally throughout the C5-T1 and L1-S1 dermatomes of the upper and lower extremities, with the exception of altered sensation noted on the right upper extremity resulting in sustained objective paresthesia overlying the right lateral antebrachial cutaneous and superficial radial nerve distributions. The upper and lower limbs showed normal sharp vs. dull, distinction between hot and cold, vibratory perception, joint position and graphesthesia. There was no astereognosis of the hands.
Visual inspection of the hands was negative for gross atrophy of the thenar eminences, bilaterally. Two-point discrimination remained intact both statically and with motion using a 7mm setting on an aesthesiometer. Light touch/pressure was intact utilizing a 5.07 (10g) Semmes-Weinstein monofilament. Phalen’s Test, Tinel’s Tap Test and Wrist Flexion with manual Median Nerve compression were all negative bilaterally for Median, Ulnar, and Superficial Radial Nerve neuropathies. Manual muscle testing of the right Abductor Pollicus and Opponens Pollicis muscles, which are innervated by the median nerve, was performed, and were graded at a 5/5.
Electrodiagnostic Studies
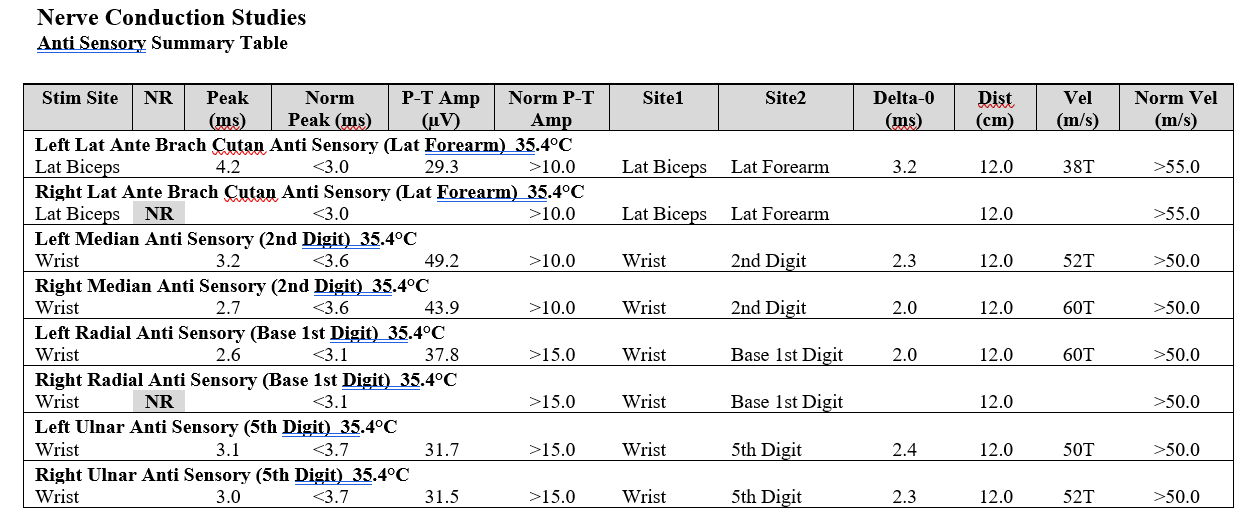
Conventional motor and sensory nerve conduction studies with late responses were performed in order to evaluate for peripheral neuropathy. Needle EMG examination of selected upper limb muscles was performed to evaluate for denervation secondary to radiculopathy. All procedures were performed using a Cadwell Sierra Summit electromyographic instrument. The needle examination was performed using 28-gauge disposable monopolar needle electrode. The relevant EMG findings are included in Table 1.

Interventions and Outcomes
The chiropractic physician conducting the electrodiagnostic studies in this case was not a direct part of the patient’s treatment team. This draws attention to the fact that specialists conducting diagnostic testing may not have the opportunity to follow-up with the patient or become directly involved in the treatment plan and/or case management. While we do not know the specific outcomes for this patient, standard interventions for neurotmetic injury have been included as a reference for readers that may have the opportunity to manage these types of injury within their practice.
DISCUSSION
While there is a plethora of information on peripheral nerve injury, treatments that ensure full recovery are limited.4 This may be due to both the varied fiber types and somatotopic organization within each peripheral nerve fascicle.5 Unfortunately, sudden recovery of functional deficits is unlikely without surgical involvement.6 As an objective measure of motor axon loss, needle electromyography has the highest sensitivity.
Needle electromyography (EMG) is a diagnostic procedure that assesses the health and integrity of motor units: the motor neurons and the muscle fibers it innervates. A needle is inserted into the muscle belly and the electrical signals are analyzed both during contraction and at rest. Assessment is imperative to confirm or exclude other differential diagnoses, defining the pathophysiology, and characterizing severity and prognosis. All examined muscles showed no evidence of electrical instability. These findings confirmed that the patient’s injury was superficial, affecting only sensory nerves.
Current research indicates that sharp nerve transections usually undergo surgical repair within 3 days.5,7 Although the patient here delayed care, it is important to note that the speed at which the severity of the lesion can be assessed is important in ensuring the best possible prognosis.
This report details a unique case of a superficial injury causing persistent neurological deficits 2 months after the initial presentation.
Since the patient came solely for electrodiagnostic workup, the results were forwarded to the referring orthopedic surgeon for final diagnosis, factoring in the clinical correlations. The objective findings provided by the electrodiagnostic studies indicate a diagnosis of neurotmetic injury of both the right lateral antebrachial cutaneous and superficial radial nerves.
Limitations
As this is a case study, the individual findings of this case may not be able to be generalized to other patients and/or clinical situations.
CONCLUSION
This case suggests that although traumas may appear to be healing superficially, there may be long-term neurological consequences and/or sequela of animal bite injury. Clinicians that may encounter similar case presentations within their practices as well as their patients may benefit from electrodiagnostic testing to determine the exact etiology of the remaining symptoms. Timing is crucial in regard to surgical repair of injuries of this type. To prevent nerve degeneration, the transected endoneuria tubes must regain contact with the newly generated axonal tissue withing a year and a half to 2 years post-injury.6
Funding Sources and Conflicts of Interest
No funding sources or conflicts of interest were reported for this study.