

INTRODUCTION
The normal cervical lordosis has been shown to have significant clinical importance, as its loss or reversal is associated with altered spinal coupling and flexibility,1–5 pain,6–8 neurological sequelae,9–11 as well as degenerative changes.12–15
Contemporary cervical spine fusion surgery recommendations are to re-establish and preserve the lordosis16,17 and minimize anterior cervical sagittal vertical axis (SVA) displacement/forward head posture (FHP)15–18 in order to prevent adjacent segmental disk disease.13–15 In 1 systematic literature review of 138 articles, for example, Ling et al.18 included the top 20 articles detailing the most relevant sagittal cervical alignment variables for patient outcomes. They found that C7/T1 sagittal plane slope, anterior cervical SVA, the spine cranial angle, and the relationship between C7/T1 slope vs. the cervical lordosis were the most important radiographic alignment variables that correlate to a ‘good clinical outcome.’18
As often as the standard neutral lateral cervical spine view is used to screen for ‘red flag’ pathology (i.e. breaks, fractures, dislocations, etc.), it is just as often used for biomechanical assessment and treatment, particularly by spine surgeons,16–18 specialty trained chiropractors,19–22 and other manual therapists.23–26
Radiology reports are a standard and required companion to imaging studies. The radiology report as taught throughout healthcare disciplines (i.e. medical radiologist, dentist or chiropractor) has the basic ‘ABC’s’ structure so as no information is overlooked for a thorough evaluation of potential pathology (i.e. Alignment, Bone, Cartilage, and Soft tissue).27–31 Spinal alignment (the ‘A’) is one of the anchors for mention and discussion on the radiology report.
The purpose of this study is to compare medical radiologists’ subjective qualitative commentary on cervical sagittal spine alignment to the x-ray images’ actual quantitative and objective mensuration.
METHODS
One of us (LJS) worked in a spine clinic (Aurora, Ontario, Canada) where patient imaging was referred out to a local medical imaging facility. One hundred and eight consecutive patients, spanning the years 2010-2012, receiving lateral cervical radiological images were reviewed for mention on the corresponding radiology reports regarding cervical sagittal spine alignment.
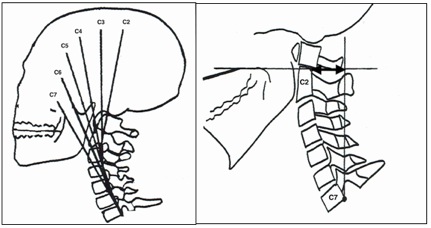
X-ray image digitization and analysis was performed by one of the authors (PAO) using the PostureRay® system (PostureCo Inc., Trinity, FL, USA) (Figure 1). This system incorporates the Harrison posterior tangent method.32 This method measures the intersegmental relative rotation angles (RRAs) between each pair of vertebrae from C2-3 to C6-7 as well as a global lordosis, the absolute rotation angle (ARA) between C2-C7 using lines drawn contiguous to the posterior vertebral body margins. It also quantifies the SVA horizontal offset measured as the anterior to posterior translation of C2 relative to C7, the horizontal distance from the posterior-superior body corner of C2 as compared to a line drawn vertically from the posterior-inferior body corner of C7 (Figure 1).

To compare quantitative measurements to subjective commentary, we devised definitive clear-cut endpoint classifications corresponding to different lordosis measurements based on previous work by Harrison et al.8 Building on the circular geometric ideal normal model of the upright static sagittal cervical spine alignment,33,34 Harrison et al.8 demonstrated statistical differences between pain subjects and pain-free subjects based on cervical alignment. Specifically, asymptomatic subjects, acute neck pain subjects, and chronic neck pain subjects had mean global lordosis angles (ARA C2-C7) corresponding to -34.5°, -28.6°, and -22° (negative indicating extension).
To be conservative in our classifications, we used the pain group averages from the Harrison study8 as clear-cut endpoints for our hypothetical categories. The upper end of ‘normal’ we considered as -42°, the ‘ideal’ from Harrison et al.34 Hyperlordosis was considered >42°. The lower end of the ‘normal’ range was considered -29°, just greater than the acute pain group average of -28.6°. The acute pain group range was -23° to -28°, -23° being just above the chronic pain group average of -22°. The chronic pain group range was set at -7° to -22°, the lower endpoint of the chronic pain group was simply one standard deviation (15°) from the Harrison study chronic pain group average (22-15=7°). This point to 0° was classed as a straight or ‘military neck’ (0 to -6°). Less than 0° was classed as kyphosis. Technically, all these values are extension positions, which should be negative (-), other than the kyphosis classification; for ease of discussion herein, we will ignore the negative sign (-).
Our cervical spine classification groupings and the corresponding degree ranges are shown in Table 1: hyperlordosis >42°, normal = 29°-42°, acute pain tendency group = 23°-28°, chronic pain tendency group = 7°-22°, military neck = 0°-6°, and kyphotic neck <0°. We also investigated the number of cases having anterior cervical SVA/FHP, considering >15mm abnormal; and normal head position < 16mm as these numbers are the mean values reported for asymptomatic subjects in the 1996 study by Harrison et al.33 We defined categories of FHP corresponding to mild (16-25mm), moderate (26-40mm), and severe (>40mm). We also assessed for the presence of any functional spinal units (FSU) in a kyphotic position (segmental RRAs >0°).
All findings were categorized into 3 groups based on the radiologist’s commentary referring to: 1. “Normal” alignment; 2. “No comment” on alignment; 3. “Abnormal” alignment.
RESULTS
Of 108 consecutively reviewed radiology reports, 8 were removed for various reasons: C7 not visible,3 head in unnatural excessive flexion1 or extension,2 image unable to open,1 and image inappropriately cropped.1 Of the 100 included images, there were 10 different radiologists who produced the corresponding radiology reports.
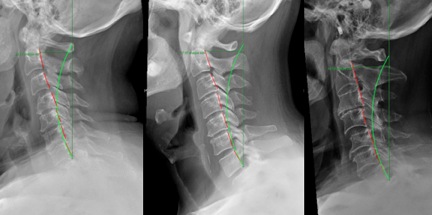
Of the 100 images included for evaluation (Table 1), 55 images were seen as ‘normal’ (Figure 2), 20 had ‘no comment’ (Figure 3), and 25 reports mentioned some sort of ‘abnormal’ alignment (Figure 4).



Using our x-ray software to quantify alignment, 51% of the sample were categorized into the chronic pain tendency group (7-22°), 17% in the normal group (29-42°), 15% in the military neck group (0-6°), 14% in the acute pain tendency group (23-28°), 2% in the hyperlordosis group (>42°), and 1% in the kyphosis group (<0°).
According to the PostureRay software measurements, 70% of the sample had anterior cervical SVA/FHP greater than 15mm. Specifically, 38%, 28%, and 4% of the sample had FHP values corresponding to mild (16-25mm), moderate (26-39mm), and severe (>40mm) ranges; thus, 32% of the whole sample had FHP greater than one inch (25mm). No radiology report mentioned FHP.
According to the PostureRay measurements, 82% of the sample had at least 1 FSU in a kyphotic orientation (>0°), whereas no medical radiology report mentioned this. Within the radiology reports’ ‘normal’ group, only 20% were actually within contemporary, conservative limits of normal, where 76% were classed in some category of hypolordotic/kyphotic alignment (<29°). Within the radiology reports’ ‘abnormal’ group, PostureRay measurements identified that all were categorized in either chronic pain tendency or military neck (Table 1). Only 30% of the radiology reports in the ‘no comment’ group had a true PostureRay measured lordosis within a normal range. Within all radiology reports’ comment groups (normal, no comment, or abnormal alignment), all groups had the majority of cases fall within the chronic pain tendency range (7-22°).
DISCUSSION
We compared medical radiologist’s commentary about sagittal cervical spine alignment as found in 100 consecutive radiology reports from a medical imaging center with 10 separate practicing radiologists to the actual mensuration of the corresponding images using a professional radiographic digitization program.
In general, medical radiology reports typically include non-specific statements regarding the cervical lordosis, they often include inaccurate statements regarding sagittal alignment, and often omit alignment information altogether. For example, of the entire sample, only 17% had a lordosis in the normal range (29°-42°), therefore, 83% of the sample theoretically should have had a statement representative of cervical spine misalignment/subluxation of some kind, but only 25% of the radiology reports did. Our findings are troublesome given that the general rule of medical imaging reporting includes the ‘ABC’s’ outline where ‘A’ is spinal alignment and is 1 of the anchors for commentary on the radiology report.27–31
It is not surprising, however, that radiologists sometimes omit lordosis information and have been inconsistent in visually diagnosing misalignment of the spine, since it has been found that visually estimating the curve of the spine has poor reliability and validity. Both Frymoyer et al.35 and Tuck et al.36 found poor correlations between visual estimation of the lordosis compared to a measured quantification of actual lordosis for the lumbar spine. We could not locate any studies of a similar nature regarding the cervical spine. Visual curve assessment is so poor that Tuck and Peterson36 recommended all chiropractors (as their study included chiropractors and chiropractic students) to always measure the lateral lumbar curve and to not visually estimate it, as "using visual means is unacceptable and should be avoided."
The medical radiologists in this study did not provide information pertaining to anterior cervical SVA/FHP. Regarding FHP, we chose 15mm or less from C2-C7 as a ‘normal’ forward head position as suggested by Harrison et al.8,33 as this was the mean value identified in 400 asymptomatic subjects. For mild FHP we chose the range of 16-25mm as this is one standard deviation from the mean reported by Harrison et al.8,33; while for moderate FHP we chose the range 26-40mm as it is known that improved long-term outcomes are found in patients with post-surgical FHP less than 25mm.37 Lastly, for severe FHP, we chose FHP >40mm as this value is clearly established as the cut-point for radiographic cervical SVA offset that strongly correlates to post-surgical pain, impairment, and altered health status.16–18,37,38
According to the 15mm cut-point, 70% of our sample had FHP greater than this range (Table 1). Considering a moderate FHP cut-point of one inch (>25mm), this included 32% of the sample that we believe should have had a statement on the radiology report. Lastly, for severe FHP (>40mm), 4% of our sample fell into this category, and again we believe should have had a comment pertaining to the biomechanical abnormality. Regardless of the actual magnitude observed, however, none of the 100 radiology reports in our sample mentioned anything about the presence of anterior cervical SVA/FHP. This is surprising since other disciplines within medicine, i.e. orthopedic and neurosurgeons, put great value in quantifying radiographic sagittal cervical posture.9,11,13–18,37,38
Similar to the FHP variable, the medical radiologists in this study completely omitted information pertaining to the presence of intersegmental kyphosis. Regarding a segmental FSU having a kyphotic alignment, considering the normal cervical RRA values should be in the range of 6-8° of extension,8,33,34 the majority of our sample (82%) had at least 1 RRA in a kyphotic orientation (>0°). This is a substantial percentage, and no report had comments pertaining to this obvious abnormality. Again, this is surprising considering that the surgical literature has produced abundant evidence documenting better long-term patient outcomes with procedures that preserve the global and intersegmental cervical spine lordosis9,11,13–15; this also helps prevent adjacent disc disease.13–15
Herein, when comments were made as to a loss of the cervical lordosis, often the medical radiologist would include an explanation for the loss of lordosis, including muscle spasm, patient positioning, and/or degenerative changes (Fig. 4). Each of these 3 explanations of causing loss of lordosis have direct evidence to the contrary, so it is surprising that these long-held traditional views continue to persist.
Muscle spasms, for example, have for decades been claimed to cause a loss of cervical lordosis.31,39–42 Causative variables for loss of lordosis are highly relevant as treatment methodologies follow from initial diagnosis. If muscle spasms were a causative variable for hypolordosis or kyphosis, then simple treatments such as muscle relaxants, pain relievers, spinal manipulation, massage therapy, and cervical stretching would naturally be associated with improved lordosis; however, this is not the case. Harrison and colleagues,19,20,43 for example, clearly reviewed the available literature and pointed out the lack of data supporting the muscle spasm causation hypothesis. In fact, this claim was recently investigated by Fedorchuk et al.44 They evaluated 29 volunteers who contracted their cervical musculature in both resisted forward head flexion (n=14) and resisted forward head translation (n=15) while simultaneously taking a lateral cervical radiograph. In comparing these images to the patient’s pre-trial baseline images, they determined that contraction of the anterior cervical muscles whether by forward translation or forward flexion may not not cause loss of lordosis. In contrast, isometrically flexing or shifting the head forward to mimic cervical muscle spasm caused a significant effect on increasing the cervical lordosis about 50% of the time. The authors state: “The results of this study are in direct conflict with over fifty years of radiographic reports, physiologic texts, and articles stating that the loss or reversing of the cervical lordosis are caused by cervical muscle spasms.”44
Inappropriate patient positioning, as an explanation for the loss of cervical lordosis, has been a rationale stated by radiologists for a long time.31,45,46 There have been many studies that determined that postural positioning is reliable and that the spine alignment of an individual as measured on a lateral radiograph is repeatable; in fact, by minutes, days, weeks, months, and even years apart.23,24,47–52 Gore,47 for example, found no statistically significant differences in lordosis measures between repeat lateral cervical x-rays taken an average of 10 years apart. Cooke et al.50–52 found no differences in several repeat studies evaluating neutral head posture repeatability radiographs in several patients taken minutes, 3-6 months, 5 years, and 15 years apart. Harrison et al.48 state: “Posture, radiographic positioning, and radiographic line drawing are all very reliable/repeatable… these results contradict common claims made by several researchers and clinicians in the indexed literature.”
Finally, degenerative changes as the origin of cervical hypolordosis is another explanation offered by radiologists. This explanation is probably the most controversial. The surgical literature, however, has substantiated that degenerative changes often result in adjacent segments following spinal fusion due to the forced excessive adjacent segment motion and altered loading patterns post-surgery.13–15 Altered segmental motion patterns are also a direct result of abnormal cervical sagittal alignments, indicating that static alterations of the sagittal cervical posture and curvature directly cause altered flexion-extension kinematics at the segmental and global levels.1,24 Although many factors will come into play, it is conceivable that altered cervical alignment which simultaneously alters segmental coupling patterns will, over time, lead to degenerative changes, and not that insidious degenerative changes lead to a loss of lordosis. Both Hohl53 and Norris,54 found that patients with cervical kyphosis after injury have a significantly higher incidence of degenerative changes. Thus, biomechanically, altered loads and motion characteristics acting on the tissues after trauma with altered alignment is likely the causative variable explaining much of the resulting degenerative changes.55–58
The real conundrum is that regardless of explanation, when a radiologist states the reason for hypolordosis or kyphosis on a report, it will be perceived as holding merit and lead to subsequent treatment strategies. Even worse, when a radiologist states the alignment is normal when it is not – this is very detrimental to the patient and future treatment needs. In these cases (which seems to occur often), driven by a ‘normal alignment’ radiology report, no treatment may be offered when there is an obvious structural problem implicated in common disorders including neck pain, headaches, or radicular neurologic symptoms. This may leave the patient abandoned at a dead-end in the healthcare continuum and cause them to seek out other expensive medical testing and to remain biomechanically undiagnosed.
If structural alignment is not recognized and is under-appreciated (Figure 3: 70% had poor alignment) relative to patient complaint/pathology, then a structural treatment course of action would never be entertained as a potential course of action. This may be one of the greatest barriers between medical co-management for patient care between, for example, a medical doctor and a chiropractor or physiotherapist specializing in structural spinal rehabilitation methods.
The single aspect of this study that supported the radiologist’s comments about an abnormal cervical curve is that when comments of loss of lordosis were made, the alignment was very poor. There were no ‘false-positives’ in terms of misnaming a poorly aligned neck as normal when poor alignment was actually mentioned; it was often in partial kyphosis (Fig. 4).
It is not surprising that the majority of the sample had poor neck alignment, since these were people who were referred by the assessing chiropractor for x-rays after an initial examination warranted spinal imaging (i.e. pain, poor posture, limited flexibility, etc.). Since radiologists typically assess radiographs of patients as opposed to asymptomatic individuals, there needs to be better criteria to aid in more realistic commentary of an abnormal cervical alignment as visualized on the lateral cervical radiograph so abnormal cervical spines can be more routinely labeled as such.
The partitioning of cervical lordosis values into the categories of hyperlordosis, normal, acute pain tendencies, chronic pain tendencies, military neck and kyphosis might seem arbitrary; however, these served as a guide to quantify the frequency of occurrences of each. Importantly, these cut-points are defensible.8,34 Other ranges of normal versus abnormal could have been used, although we attempted to use conservative criteria. For example, McAviney suggested that the range limit of a normal lordosis could be 31-40°,7 whereas we used 29-42° so as to include a larger and more conservative range. Likewise, the categorization of anterior cervical SVA/FHP into normal (0mm-15mm), mild displacement (16mm-25mm), moderate displacement (26mm-40mm), and severe displacement (>40mm) might be contentious to some, though these cut-points are well supported in the literature8,16–18,37,38 and surprisingly none of the radiology reports mentioned this important sagittal plane alignment variable.
Limitations to this study were that all the radiology reports corresponding to the images analyzed originated from a single imaging centre. However, 10 separate medical radiologists generated the reports included in our 100 patient cases. There may be slight differences between different radiologist’s radiology reporting, as well as trends between different radiology centers in the writing of radiology reports; however, these should be minimal considering the ‘ABC’s’ guide to report writing.27–31 Further, we had no control over what instructions were given to the patient during the taking of the cervical radiograph at the imaging facility. Even if a patient stood with an artificially flexed neck position, however, we would have assumed it would have been mentioned on the radiology report.
CONCLUSION
From our findings we determined that medical radiologists may make generalized, non-specific comments regarding cervical lordosis, when mentioned at all. This suggests that they may not consider the importance of cervical spine alignment as being involved in a patient’s complaint even when evidence suggests that cervical spine sagittal alignment is implicated in neck and headache symptomatology, physiological function, neurophysiological outcomes, and degenerative changes. This situation may fuel barriers between differing healthcare professionals in how much emphasis should be placed on biomechanical alignment in the etiology of a patient’s cranio-cervical complaints.
Acknowledgements
We thank Niousha Navid Ehsani, MD for feedback on this manuscript.
Conflict of Interest
PAO is a paid consultant to CBP NonProfit; DEH teaches chiropractic rehabilitation methods and sells products to physicians for patient care as used in this manuscript.