Introduction
Musculoskeletal conditions are among the most common conditions that plague humans. Low back pain, neck pain, and other musculoskeletal disorders rank in the top 10 in 2013 for years living with disability (YLD) based on findings published in The Burden of Musculoskeletal Diseases in the United States,1 Low back pain has the highest prevalence among all persons over the age of 18, affecting 28.5% of the population1 and is a common reason to seek treatment at an emergency department (ED). Prevalence of low back pain in the ED ranges from 0.9% - 17.1%2 and 6-year prevalence of 3.17%.3 Of the low back pain ED cases only 0.7%-7.4% required urgent care for conditions like vertebral fractures, spinal cancers, and other.4 In fact, 97%of patients with back pain were not admitted to hospital after waiting in the ED. Therefore, non-emergent low back pain cases are more prevalent than emergent cases, contributing to overcrowding and consumption of unnecessary resources.5
To combat the use in non-emergency musculoskeletal complaints, physiotherapists within some ED’s evaluate and manage patients with musculoskeletal conditions. Evidence shows numerous benefits to this type of integrated care. An observation study performed by Sutton et al found that there were no adverse events associated with a primary-contact physiotherapist in 1320 patient encounters. The model decreased the average length of stay in the ED from 185 minutes, with typical medical evaluation, to 103 minutes when evaluated by a physiotherapist.6 This was not the only study to have these conclusions. Articles published by Taylor and Bird also concluded that a primary-contact physiotherapist evaluating patients with musculoskeletal conditions significantly reduced the wait time and treatment time for the patients.7,8
Chiropractic treatment (ie. spinal manipulative therapy, myofascial therapy, therapeutic exercise) are effective treatments for low back pain.6 The objective of this report is to describe coordination of care between an emergency department and hospital-based chiropractic clinic paralleling the role primary-contact physiotherapists have served in evaluation and management of musculoskeletal conditions within the ED for low back pain patients.
Case Report
A 35-year-old woman was brought from the ED to the chiropractic clinic. She had an acute flare-up of chronic low back pain that encompassed her low back, sacrum, and gluteal region. The initial onset of her back pain was in 1999 from a hyperflexion injury that occurred while carrying a rucksack during basic training. At the time of her initial visit, she described the pain as a burning, sharp and constant that she rated as a 10/10 that occasionally radiated into the left gluteal region. Aggravating factors included standing upright, being in a prolonged seated position, and lumbar flexion/extension. No relieving factors were identified, and symptoms have been worsening since the onset in 1999. Comorbidities included anxiety, post-traumatic stress disorder (PTSD), bipolar disorder, migraines, alcohol, and tobacco use.
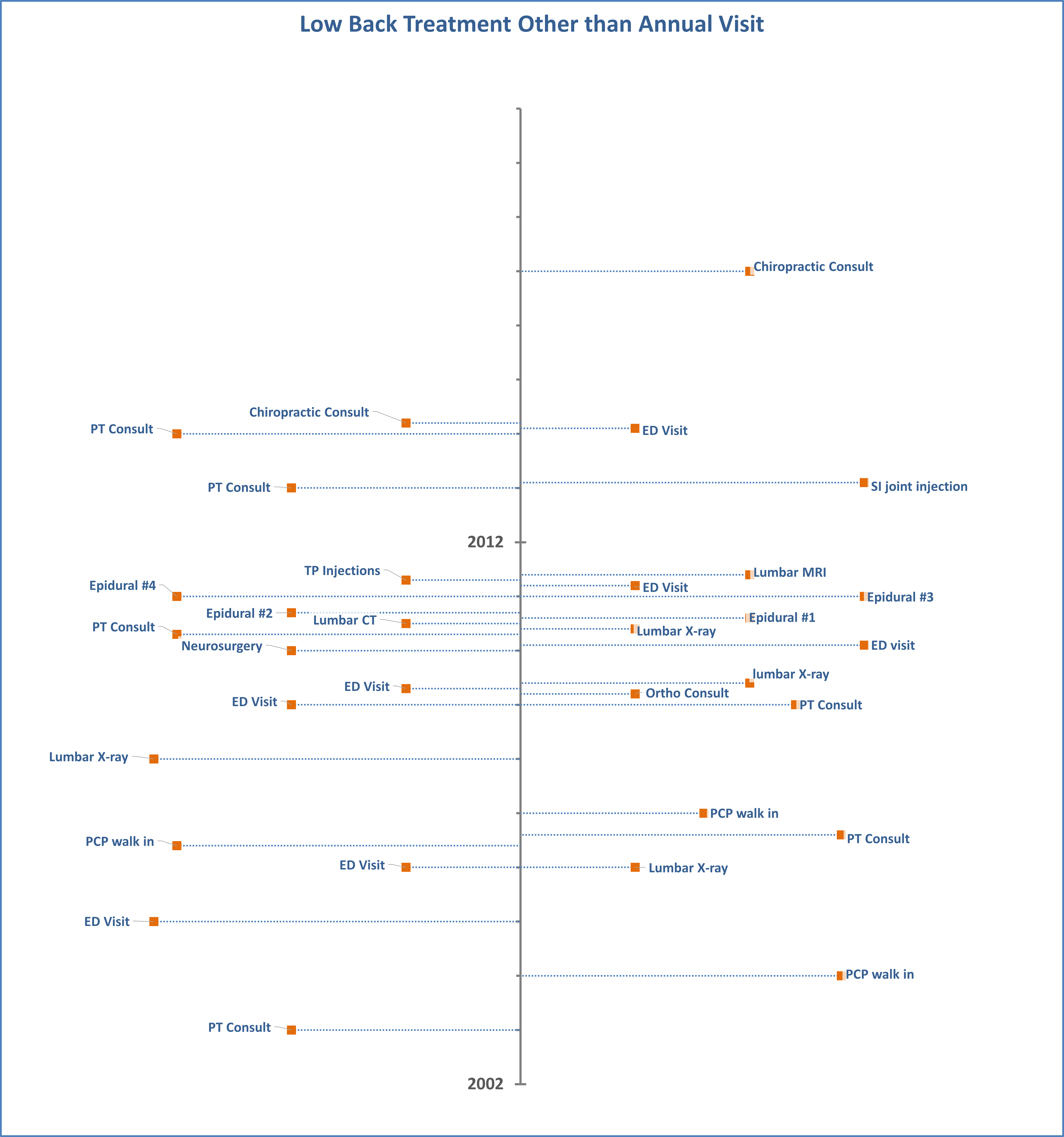
Previous care and timeline are present in Figure 1. Prior to her visit at our clinic, review of her documentation illustrated that from 2003-2014 she had 12 visits as either a walk-in to her primary care physician or to the ED for severe aggravation of her low back pain. Numerous physical therapy appointments, injections, pain management visits, radiographs, and an MRI occurred without any prolonged benefit. Trials of NSAIDs, glucocorticoids, muscle relaxants, neuropathic medications, and opioids also offered little to no benefit.

Examination by us provided positive orthopedic findings for the straight leg raise, Slump’s, Ely’s, Nachlas’, Kemp’s, Femoral Nerve Tension, and SI joint compression, which all provoked bilateral sacral pain. Trigger points were found within the gluteus medius and piriformis muscles. Sensation, motor function, and reflexes were all normal during the neurological examination. Previous lumbar x-rays found mild degenerative disc disease in the lumbar spine.
Treatment included side-lying manipulation of the SI joint along with myofascial release technique to the gluteus medius and piriformis muscles, followed by therapeutic exercise including gluteus bridges. Patient education included information about the natural course of low back pain, differentiation between hurt and harm, reinforcing the therapeutic benefits of activity, and negating bed rest. This treatment plan was performed over 12 visits over 14 weeks.
Outcome
The patient experienced significant improvement. She was able to resume normal activity and was to begin exercise. Following the course of care, she has had no further aggravation of her low back pain. Documentation illustrates no ED visits, primary care walk-in, or additional diagnostic imaging since discharge from our clinic. Her course of care included 12 visits, resulting in the Oswestry Disability Index score decreasing from 50% to 8% and her PROMIS Pain Interference score improving from 30 to 8.
Discussion
Authors have provided models for triage of spine pain that illustrate the benefits of chiropractors and physical therapists in first-touch or front-line treatment of spine pain.9,10 The latter provide evidence of outcomes and cost savings in the management of spine pain, but lack direct evidence translating spinal triage by a chiropractor within the Emergency Department. Case collaboration of care between an emergency department and a chiropractic clinic is not well represented in the literature; however, Shilke et al recently published a model for consideration.11 In contrast, the physical therapist’s role within the ED has been established within the literature and the following benefits noted:
-
No misdiagnosis or adverse events over the course of the observational study6
-
Significant reduction in the time the patients spend in the ED,
-
Decrease in the diagnostic imaging performed, consistent with other studies.6,12–15
While the role of physical therapy cannot be directly translated to a chiropractor, crossover exists with scope of practice and literature supports both professions as appropriate options for front-line options for the triage of pain assist in validating concept and potential pilot.
Within the triage of spine pain, the importance of screening for yellow flags must be emphasized. Marshall examined the mediating effect of fear, anxiety, depression, and catastrophizing within the chronic low back pain population. His study found the following: “1) fear, catastrophizing, and depression explained 42.4% of the relationship between pain and disability, 2) the mediating effect of catastrophizing was conditional upon the performance of weekly physical activity, 3) catastrophizing mediated the relationship between pain and fear, the first proposed pathway in the fear- avoidance model, and this was not conditional upon the performance of regular physical activity.”16 Many different avenues were pursued to address our patient’s non-specific low back pain (Figure 1), but relief was not achieved, resulting in continued report to the ED. During her biopsychosocial assessment, it was clear that she felt like she was damaged, was anxious about the potential progression of her symptoms, and alarmed that no one could show her why she continued to have pain. Her comorbid conditions of anxiety, manic depression, PTSD, and bipolar disorder further complicated her presentation yet treatments addressing these comorbidities had not been embraced. Physical activity often aggravates patients reporting with low back pain and comorbid fear, anxiety, and depression as a result of catastrophization.17 Patient education addressing neurophysiology and neurobiology of pain can have a positive effect on pain, disability, catastrophization, and physical performance.18 During the course of care provided above, education related to the neurophysiology of pain, reassurance that she was not damaged, and positive association of activity complemented the manual therapy and therapeutic exercise. Quantification of the impact education made cannot be directly measured as multiple modalities (manual therapy, therapeutic exercises, patient education) were performed; however, this case does represent pragmatic implementation of evidence into clinical care.
Significant limitations exist in this report. First, this is a single case and no generalizable conclusions can be drawn from it. Second, the natural history of low back pain is favorable with 0 to 60 percent of patients recovering within 1 week; 60- 90%recover in 6 weeks, and 95%recover in 12 weeks.19,20 However, 40% of cases relapse within 6 months.21 Therefore, the patient could have experienced spontaneous resolution as a result of natural history. Third, this was retrospective assessment of a scenario and a causal relationship cannot be concluded since the results could be mere coincidence. Fourth and finally, falsification of criterion cannot be satisfied as reproduction of this case cannot be completed.
Conclusion
Collaboration between the emergency department and the chiropractic clinic provided a good outcome for this patient. Results are not generalizable to the population as this is a single case; however, it does serve as an example of pragmatic implementation of evidence into clinical care. Following engagement in the clinic, significant reduction of health care utilization occurred, and these results were longstanding.