


INTRODUCTION
Vascular thoracic outlet syndrome (VTOS) can present a number of different ways, including with pain, numbness, paresthesia, or muscle weakness in the upper limb, swollen or cyanotic upper limb, large veins in the shoulder, chilly and pale hand, and pain during overhead arm motions. Thoracic outlet syndrome (TOS) has been most consistently diagnosed and classified when a complete history, clinical presentation, physical examination, and relevant radiographic and electrophysiological investigations are included. Due to the non-specific nature of regularly-used provocative tests such as Allen’s and modified Adson’s, there is no standard approach for establishing the diagnosis. The reliability of interdisciplinary diagnosticians in diagnosing TOS is limited. During routine TOS check-ups, orthopedic surgeons were more likely to diagnose TOS than neurologists. The standard treatment for TOS has been first rib resection, which has a success rate of more than 90%. Our patient with vascular TOS was managed conservatively.
CASE REPORT
History
A 30-year-old male had a sudden onset of intermittent numbness, tightness, and weakness in his right hand. The paresthesia was primarily on the right, and he was unable to use his right thumb to operate a smartphone or pinch with his right first and last fingers due to weakness. He stated that the symptoms began with a right-shoulder separation injury, and he experienced swelling and a chill sensation throughout his right upper arm. Exercise was identified as the provoking motion, and pain medicines were ineffective. He described the experience as a combination of pain, numbness, and tightness, which he assigned a rating of 6/10 on the Numerical Rating Scale (NRS). Due to the patient’s allergy to the contract media, his neurologist ordered laboratory and diagnostic tests, including MRIs of the cervical, thoracic, lumbar, right shoulder, and right wrist; general blood work; EMG and nerve conduction studies of the upper limbs, and full body thermography. He was diagnosed with negligible lumbar disc bulging, mild rotator cuff tendinitis, and unequal shoulder and hand temperatures (Figure 1). He was treated for ATOS with muscle relaxants, physiotherapy exercise, massage therapy, and acupuncture, but none of these treatments improved his symptoms. He then sought chiropractic care.

Physical and Other Examinations
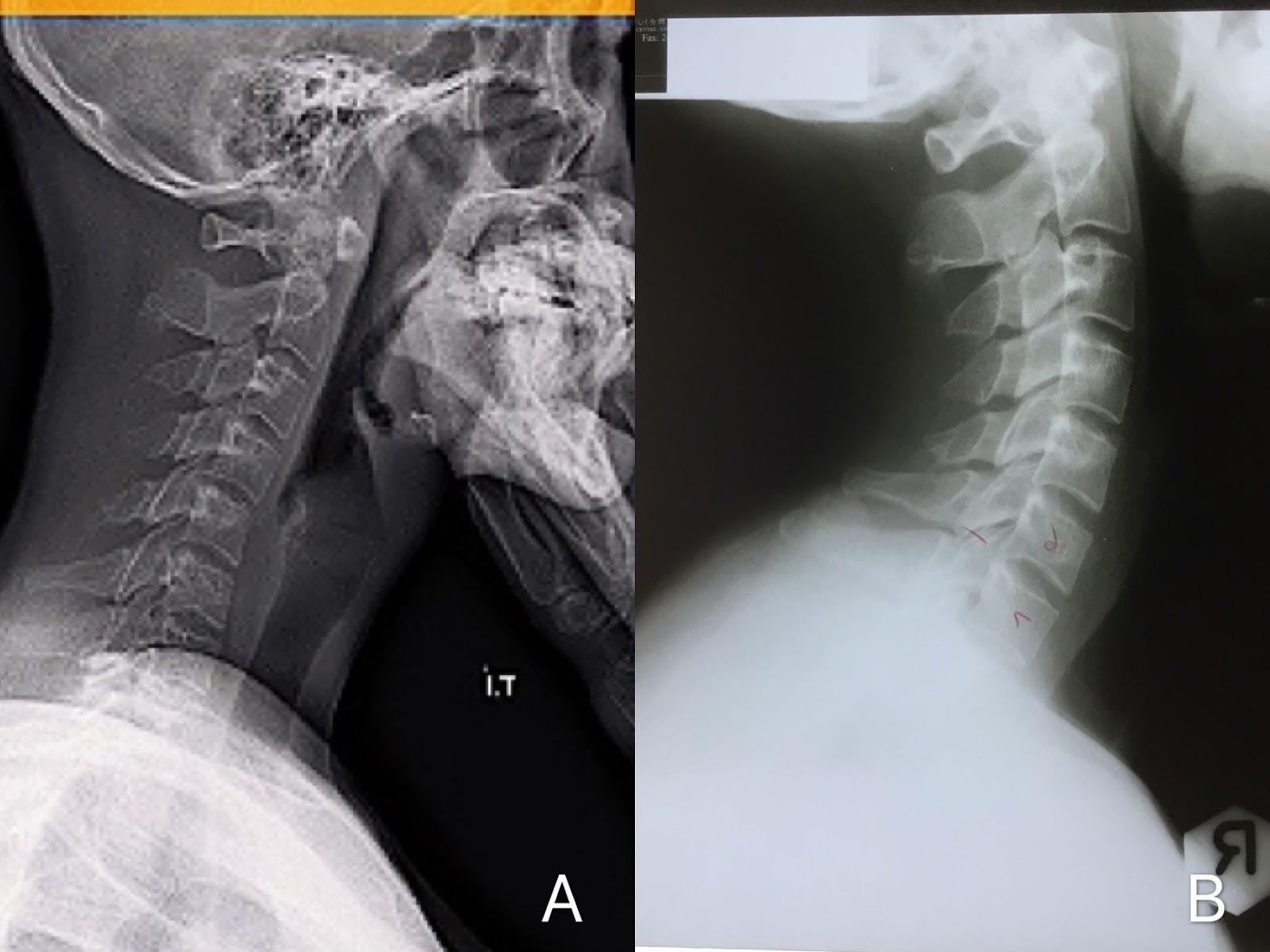
The patient haad skin flakes on his right upper limb, cyanosis on the right shoulder (Figure 2); and a cold and pale right hand (Figure 3). Orthopedic examination revealed positive Allen’s test on the right for radial artery insufficiency; and positive modified Adson’s tests for bilateral upper limb numbness and right diminished pulse. Muscular palpation indicated swelling along his right upper arm, hypertonicity on the right scalene muscles, and hypotonicity at right rhomboid and levator scapulae. His motor strength of right elbow/wrist flexors and extensors were graded 4/5, and both flexors and abductor of right 5th metacarpal were significantly weaker than left. (Figure 3). Spinal palpation found intersegmental dysfunction in C4/5, C5/6, T1/2, and T3/4 and his cervical spine X-ray showed reduced cervical lordosis and a forward head posture (Figure 4A). Based on the clinical presentation and that the cervical rib was not identified in diagnostic images, the patient was treated for thoracic outlet syndrome with vascular involvement.


Management
The treatment protocol included spinal manipulative therapy (diversified technique) and thermal ultrasonography to rehabilitate the cervical and thoracic regions’ mechanical and nerve dysfunction. To rectify the posture deviation, instrument-aided soft-tissue mobilization (Strig ®, IASTM Tool, Korea) was used on the scalene muscles, and strengthening exercises were prescribed for the trapezius, pectoralis, levator scapulae, and rhomboids. The patient received 24 treatments over a 6-week period and experienced complete remission of his upper arm symptoms and skin issues, but observed periodic tingling in his left hand. He resumed his treatment with the goal of correcting his posture. Extension-compression traction (Chiropractic Biophysics Technique@) was added to his treatment schedule twice weekly for an additional 3 months to improve his frontal head position. The patient reported that his symptoms had completely resolved, and his repeated orthopedic exams for TOS and cervical lordosis were normal. (Figure 4B).
_pre-treatment_sagittal_radiograph_indicated_l.jpeg)
Follow-Up and Outcome
At the 12-month follow-up, the restoration of craniocervical stability improved neck pain, cervical mobility, and overall quality of life. The patient expressed high satisfaction with the treatment. During the 12-month period of care, no adverse events occurred.
DISCUSSION
VTOS only accounts for 5% of TOS, and the compression of the subclavian vessels usually occurs at the scalene triangle, the costoclavicular space, and the subcoracoid space. In patients with arterial TOS, cervical rib represents 50%, followed by soft tissue anomalies in 33% of patients and post-clavicle fracture representing 5%, leading to impingement of the artery.1 Scalene muscles may produce TOS when the rib or a fibrous band connecting the cervical rib to the first rib compresses the subclavian arteries and/or brachial plexus. Vascular obstruction causes signs include cyanosis, pallor, coldness, and early fatigability; therefore, clinical presentation becomes critical in making diagnosis of TOS.2
The osteo-structures of the thoracic outlet are made of the first rib, sternum and spinal segment. The 2 most common areas of compression leading to thoracic outlet syndrome include the scalene triangle and the costoclavicular space. The borders of the scalene triangle are made of the anterior scalene muscle anteriorly, middle scalene posteriorly, and superior border of the first rib inferiorly. It becomes the area of most common for brachial plexus impingement, leading to neurogenic TOS as the subclavian vein courses anteromedial to this space. The costoclavicular space is between the first rib and clavicle and it is the most common area leading to vascular TOS. The compression of subclavian vessels is commonly caused by either congenital anatomical variants such as cervical rib and abnormal tendon insertions, or acquired anatomic anomalies such as muscle hypertrophy.3 What makes our case interesting is that both neurological and vascular signs were alleviated through treatments of hypertrophy of the scalene muscles and spinal intersegmental dysfunction, with no involvement of congenital anatomical abnormalities.
Clinical presentation of vascular TOS can be variable, ranging from pain, numbness, paresthesia, or muscle weakness in the upper limb, swollen or cyanotic upper limb, prominent veins in the shoulder, cold and pale hand, and pain during overhead motions of the arm. These symptoms are the result of compression of the subclavian artery and vein, and an absent radial pulse is common. Hypertonicity of scalene muscles is commonly observed in vascular TOS. A variety of ischemic symptoms are shown at the orthopedic provocative tests, depending on chronicity and duration of ischemia.4
Although several studies have shown improvement with the use of conservative care, uncertain diagnostic criteria and the lack of a “gold standard” limit the generalizability and clinical utility of the studies.5 Our case report demonstrates the multifaceted nature of assessment for patients with unusual symptoms. Shoulder cyanosis, swelling, skin flakes, and upper limb weakness suggested a vascular cause for the findings. Physical examination is important and should include several provocative tests. Allen’s and modified Adson’s test are 2 useful maneuvers for reproducing the symptoms. Cervical x-ray should be performed first to assess for cervical structures and bony abnormalities. Since our patient was allergic to contrast media, MRI of spine, shoulder, and wrist was useful for analyzing nerve compression and to rule out soft-tissue abnormalities. Full body thermography is a good supplementary tool to assess temperature distribution in association with circulation, and electrophysiological assessment using EMG examination and nerve conduction studies are useful in identifying nerve injury. Arteriography is only meaningful to assist in planning blood vessels reconstruction.6
Effective management of the vascular TOS requires early recognition and elimination of other pathologies. Goals of chiropractic treatment include1 alleviation of motor and sensory dysfunction,2 reduction of vascular symptoms and3 restoration of muscular and osteopathic dysfunction. Many studies have confirmed the effectiveness of chiropractic spinal manipulation in alleviating cervical radiculopathy.7 It also increased the lymphatic return from sympathetic responses, which can help eliminate swelling.8 Instrumnet-assisted soft-tissue manipulation was useful for improving soft tissue function, removing pain substrates of hypertonic muscle fibers, and reducing swelling.9 Restoration of the hypolordotic cervical curvature may also have helped reduce the spinal nerve tension, release its pinched nerve, and subsequently alleviate arm numbness and muscle weakness in this patient.10 Similar therapeutic outcome for cervical radiculopathy had been reported recently by correcting a lateral head posture.11
CONCLUSION
We discussed the case of vascular TOS in a 30-year-old male who was successfully treated with conservative care. Although there is a paucity of published reports describing the management of patients with vascular TOS using conservative management, we believe our case is interesting due to aneurysmal changes of subclavian vessels alleviated by restoration of cervical lordosis and scalene hypertonicity without rib abnormality. To our knowledge this appears to be the first case that describes the successful amelioration of vascular TOS using both spinal manipulative therapy and instrument assisted soft tissue manipulation.
Funding Sources and Conflicts of Interest
No funding sources or conflicts of interest were reported for this study.