INTRODUCTION
Radiology has been a cornerstone for the analysis of spinal alignment for over a century.1,2 Despite this tradition, there has been increasing pressure from within the chiropractic profession against routine use of radiology (i.e. ‘red flag’ only x-ray guidelines).3–6 Recently, the American Chiropractic Association joined this x-ray image reduction campaign with its ‘Choosing Wisely’ initiative and released the statement: ‘Five things physicians and patients should question.7’ Items 1 and 2 include restraint from spinal imaging.
The notion of restricting spinal imaging may not only be unsafe for the patient,8,9 it may also limit the effectiveness of care offered,10 and is not consistent with the views of large factions of the profession that routinely x-ray their patients.11–13 One of the driving goals behind the efforts of minimizing the public’s exposures to ionizing radiation in the form of x-rays is the presumed and feared development of future cancers. Alternatively, a foremost goal behind limiting radiography within chiropractic is the presumed lack of biomechanical information to be gained from spinal imaging (i.e. non-existence of ‘subluxation’).
The purpose of this commentary is to present a brief summary of evidence supporting the scientific basis of 6 contemporary subluxation types that currently underpin the basis for routine radiographic examination for biomechanical data related to the diagnosis and treatment of patients in modern chiropractic practice. We also discuss how these 6 types of subluxation satisfy Nelson’s criterion and achieve valid subluxation theory status.
DISCUSSION
The New Biomechanics: Rotations and Translations of Human Posture
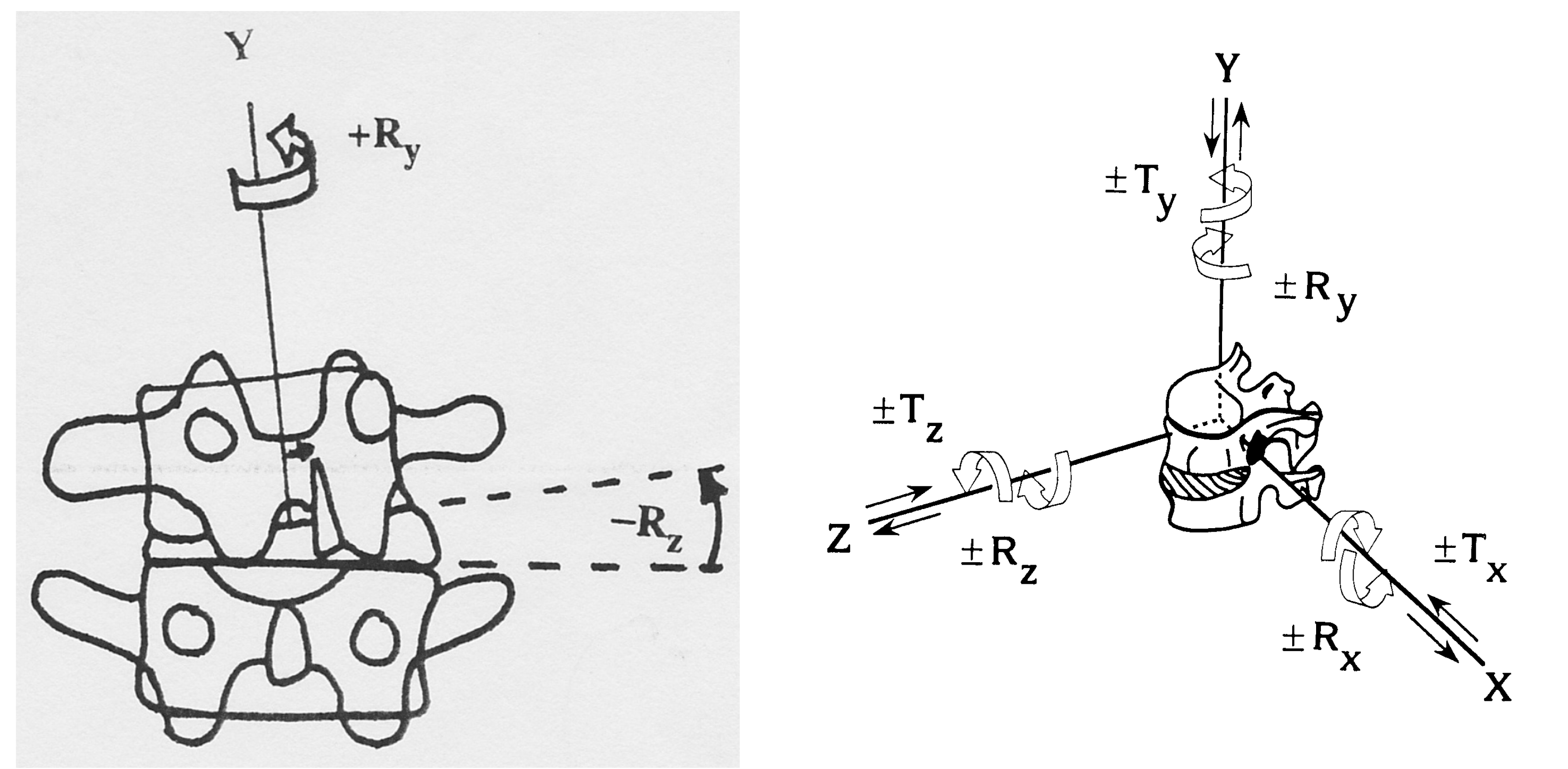
Biomechanics is the study of mechanical laws relating to the structure and dynamics of the body, including the static analysis of spinal structure on x-ray. Although traditionally, the ‘chiropractic subluxation’ was thought to be a single vertebra out of alignment14 and was described by traditional ‘listings’ as measured from radiographic analysis (i.e. Gonstead listings such as ‘PRS’ – Figure 1),15 Harrison16 would later point out that these traditional listings were mere partial explanations of a vertebra as described from a full analysis of 12 simple motions (positions) in 6 degrees of freedom (Figure 1).
_are_simplistic_representations_of_t.png)
As chiropractic evolved into the era of scientific investigation after the 1970s, the few studies that have evaluated pre-post adjustment changes failed to demonstrate significant radiographic changes or re-positioning of the ‘subluxated vertebra.’ [i.e. Plaugher (17)], Harrison (18), Hurwitz (19), Shilton (20)].
Because of this apparent lack of evidence, a proportion of the profession (i.e. demanding evidence-based science) adopted the concept of the ‘manipulable lesion’17 (and many other terms18) as replacement of traditional ‘bone out of place’ aspects of subluxation terminology. As a result, the majority of chiropractic researchers pursued avenues in many areas; all but abandoning the long quest to identify the chiropractic subluxation).
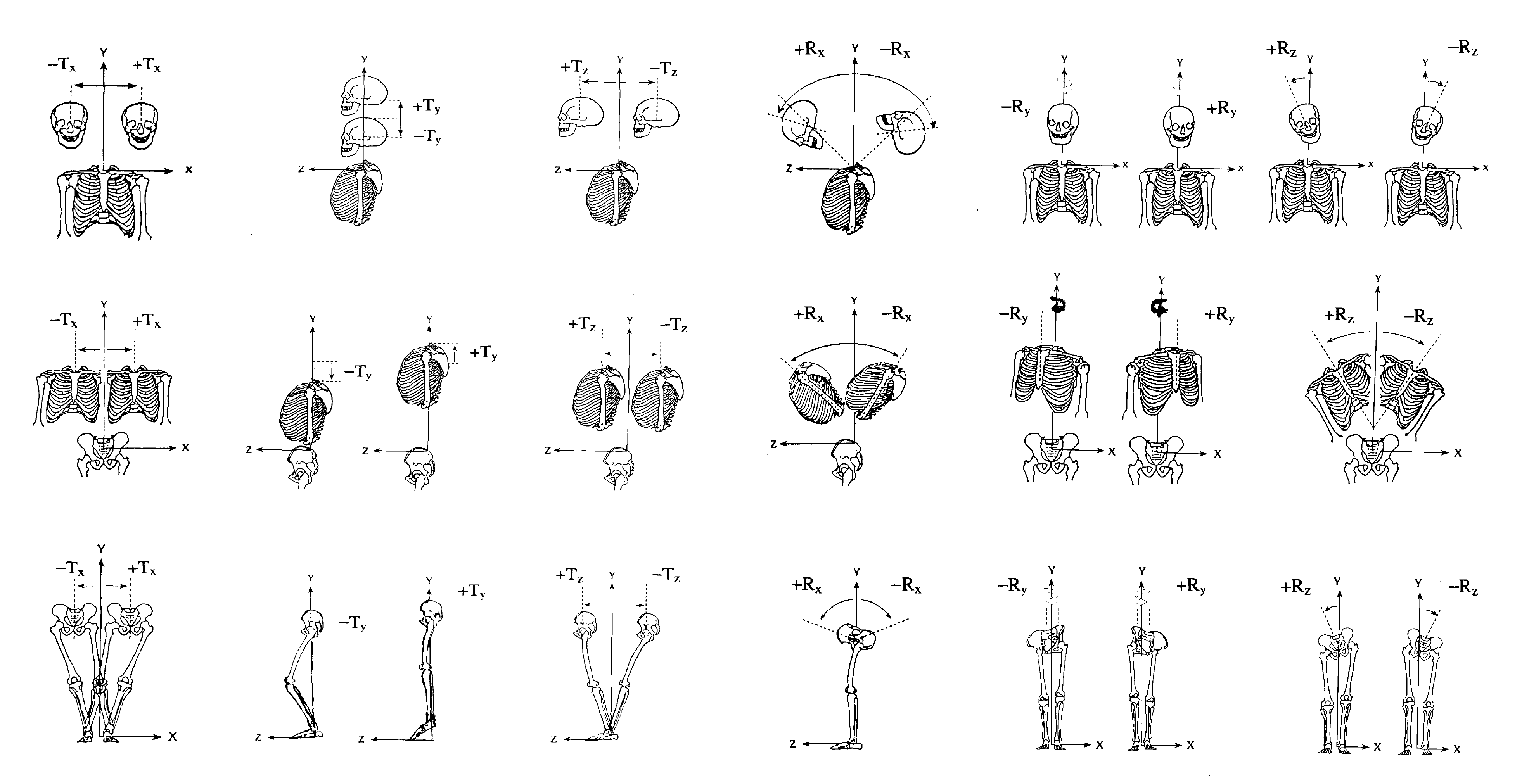
During the mid 1980s to mid 2000s, Harrison’s group achieved what the chiropractic profession long sought after – a precise, reliably measured, and validated normal and ‘subluxated’ human spinal model.16,19–21 Applying Panjabi’s rotations and translations descriptions of 3-dimensional movement about a Cartesian coordinate system,22 Harrison first described this in relation not to a joint, but to the main body segments of human posture (i.e. head, thorax, pelvis).16,19–21 With the description of ideal or physiologic posture (no rotations; no translations) comes with it, the non-subluxated posture and therefore, also non-ideal/non-physiologic postures represent a type of ‘subluxation,’ (i.e. specific rotations and/or translations of the head, thorax, pelvis). Although presented in 199616 (the seminal and only indexed chiropractic journal at the time) it was not widely recognized (i.e. did not make a significant impact), likely due to its mathematical basis. Despite this, it remains the key biomechanical discovery essential for the mathematical description of the fundamentals of posture and ‘subluxation.’

The Normal Human Spine
Although traditionally debated within chiropractic, there absolutely must be an ideal configuration of the human spine as based on evolutionary considerations (lumbar lordosis essential for bipedal gait23), anatomical considerations (i.e. wedging of discs creating cervical/lumbar lordosis24; wedging of vertebra creating thoracic/sacral kyphosis24; orientation of facet joints24; sagittal alignment determining spinal coupling25,26; sagittal balance27–29), and biomechanical considerations (i.e. spinal load-bearing capabilities24,30,31; injury mechanisms24,30–34; osteoarthritis development23,35–37). A general overview of the biomedical literature supports a normal human spine; it is the precise orientation of the spine, however, remains debated (i.e. precise shape of spinal regions with associated average/ideal normative data).
Although many have attempted to model the shape of the normal human spine, few have done so as comprehensively and systematically as the Harrison group.38–45 In a series of papers, elliptical shape modeling of the path of the posterior longitudinal ligament was performed on radiograph samples of asymptomatic subjects. The modeling would determine a best-fit geometric spinal shape by fitting various ellipses of altered minor-to-major axes ratios to the digitized posterior vertebral body corners of the spinal regions (i.e. cervical,38–40 thoracic,41,42 lumbar43–45).
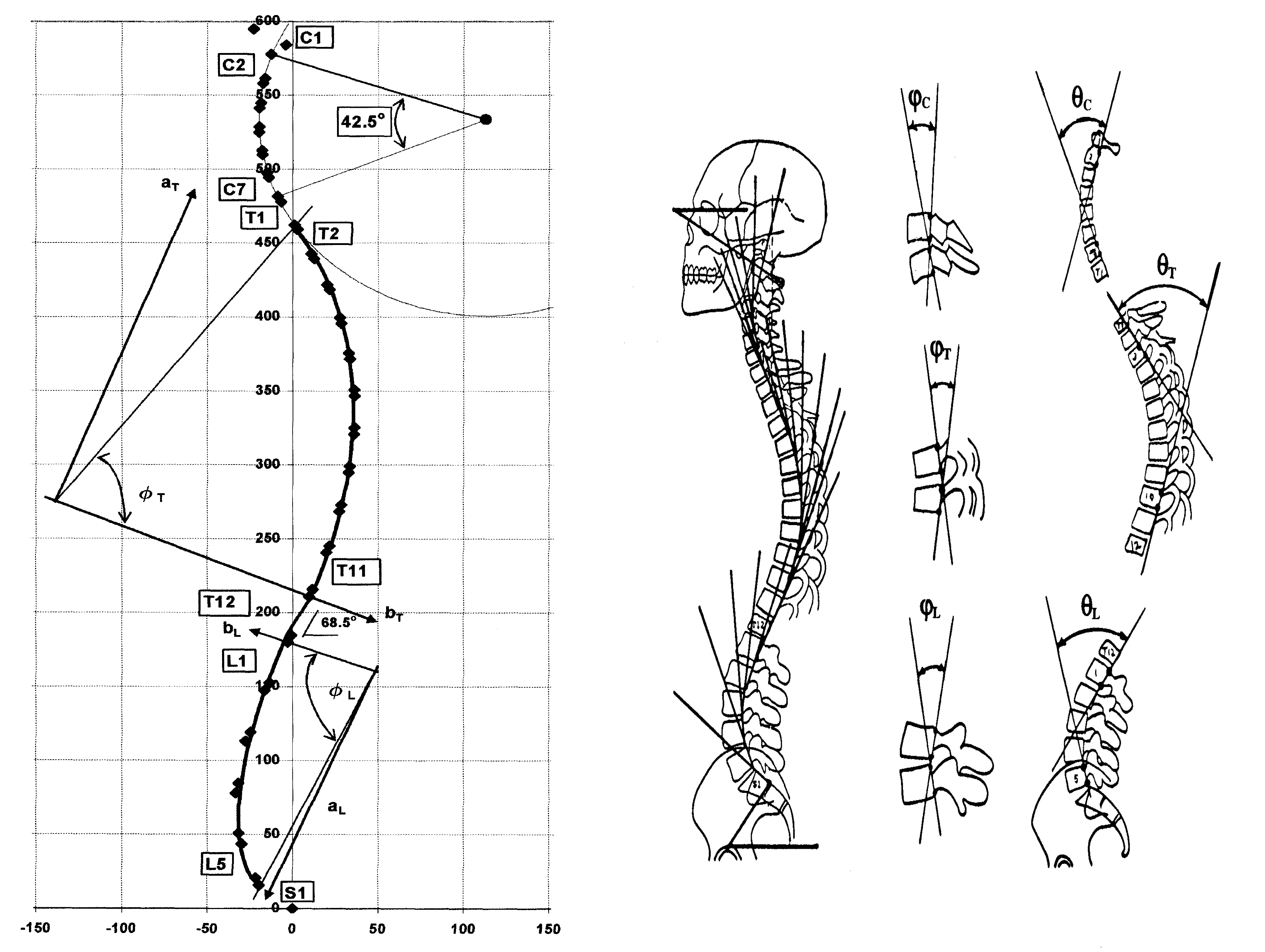
The Harrison normal spine model (Figure 3) features a circular cervical lordosis, an elliptical thoracic kyphosis (more curvature cephalad), and an elliptical lumbar lordosis (more curvature caudad). Consequently, features of the normal human spine revealed that the opposite thoracic and lumbar curves meet together at the thoraco-lumbar junction being essentially straight; the upper, deeper curve of the thoracic spine reflects oppositely at the cervico-thoracic junction (between T1 and T2) and continues into the cervical lordosis; the lower lumbar spine increases its lordotic alignment having two-thirds of its curve between L4-S1 as it meets the forward positioned sacral base. The spine is modeled as vertical in the antero-posterior view. Spine alignment is easily measured and quantified by radiography46–50 (Figure 3).
Validation of the Harrison model has been achieved in several ways:
-
By analyzing alignment data of normals38–45;
-
By comparing normal samples to symptomatic samples38,51;
-
By comparing normal samples to a theoretical ideal model38,39,42,44;
-
By statistically differentiating normals from pain groups based on alignment data41,45;
-
By demonstrating paralleled alignment improvements with pain and disability, versus no change in untreated control groups in pre-post trials52–57;
-
By demonstrating, in randomized trials that only patient groups achieving lordosis improvement (lumbar or cervical) achieve long-term improvements in outcome measures versus comparative treatment groups not getting spine alignment improvement who regress long-term after achieving only short-term, temporary symptom relief.58–65
It should be noted that the Harrison normal spinal model (Figure 3) serves as the baseline for patient comparison. Specific patient comparisons to this model, however must include patient-specific measurements related to both pelvic morphology66 as well as thoracic inlet67 parameters as these may dictate a modification to this spinal model for a given patient. Although beyond the scope of this paper, pelvic morphology and thoracic inlet are important factors to be considered in the application of this model to patient care and are routinely considered by chiropractors practicing Chiropractic BioPhysics technique and is included in the PostureRay x-ray analysis software system (PostureCo Inc., Trinity FL, USA).

The 6 Contemporary Subluxation Types
There are 6 different types of spinal subluxations1,16,68:
Coupled spinal motions: Rotations and translations of the head, thorax, or pelvis (main motions) will display spinal coupling patterns that deviate in predictable ways about the normal static spinal position.69–73 These patterns of regional vertebral misalignments may occur with dynamic movement; however, they are specifically referred to here as diagnosed in neutral resting stance.1,16,68
Snap-through buckling: Primarily associated within the sagittal plane, ‘snap-through’ is a spinal buckling phenomenon that occurs when there is sudden change of an equilibrium configuration (i.e. a lordosis buckling into a kyphosis).32–34,74–87 Different biomechanical equilibrium states can be categorized as different buckled modes, such as first order (S-shaped), second order (triple curve), etc. These typically occur during sudden loading impacts (i.e. falls, head impacts), overloading events (i.e. lifting), or inertial loading events (i.e. motor vehicle collisions).
Euler buckling: Similar to snap-through, ‘Euler’ buckling occurs by similar loading events to the spine in the frontal/coronal plane.88–90 Euler buckling most often occurs in the lower spinal regions (i.e. cervico-thoracic, thoraco-lumbar, lumbo-pelvic junctions) and is readily visualized on AP/PA and lateral radiographic views.89,90 Euler buckling creates complex 3-D displacements of the affected segments where lateral flexibility, axial rotation, and lateral shear is seen in frontal views and hyper-flexibility/extension and anterior/posterior shear may occur in the sagittal plane. Goel et al. has demonstrated that this is the type of buckling that likely causes postero-lateral lumbar disc herniation after applying a flexion-compression axial load to the lumbar spine simulating the effect of a sudden load shift during heavy lifting.89
Slow-loading buckling: Scoliosis is a type of ‘slow-loading’ buckling.70,91 Not associated with a sudden impact or rapid loading, this spinal deviation develops over time with sustained and gradual buckling occurring continuously as its worsening displacement contributes to further buckling.
Segmental instability: Whether static or dynamic, a segmental instability is a segment that is at or beyond the limit of range of motion of the functional spinal unit.92–100 These are associated with ligament damage.
Segmental subluxation: A segmental subluxation is a segmental displacement of a vertebra relative to the inferior vertebra (occurring from C1-S1), and described in terms of Rx, Ry, Rz, Tx, Ty, Tz.101–103 This represents the traditional ‘subluxation’ where the focus to one vertebra malposition may occur from a coupled spinal pattern resulting from a main postural motion, a type of buckling, or a segmental instability. This probably represents the majority of traditional ‘segmental subluxations’ arguably a case of ‘missing the forest for the trees.’ That being said, there may be occasions where segmental subluxations occur unrelated to any of the subluxation types previously mentioned, such as for a C1 atlas subluxation.104,105
Nelson’s Criteria for a Valid Subluxation Theory
In attempts to clarify whether the subluxation phenomenon is a real and valid entity, Craig Nelson presented a set of 6 criteria necessary to evaluate a subluxation theory; in his commentary, he states its purpose was to “attempt to bring some order and reason to the debate and to suggest a means of resolving the issue.” We present these 6 criteria and briefly discuss how each are satisfied with the presented types of subluxation:
-
It should bear some resemblance to its historical antecedents: Palmer’s traditional ‘bone out of place’ ideology is analogous to an individual vertebrae placement within a regional spinal displacement from normal as occurs in the various buckling, spinal coupling associated with postural rotations and translations, or ligament damage subluxation scenarios.
-
It should be testable: These ‘new’ types of subluxations are testable as three-dimensional posture and two-dimensional spine alignment data are nowadays very easily attained and quantified using reliable and repeatable measurement methods from radiography and photography or other well-studied methods.46–50 Further, as discussed by Harrison,16 traditional listings (i.e. PRS) were not amenable to study, however, contemporary descriptions using rotations measured in degrees and translations measured in millimeters are easily studied.
-
It should be consistent with current basic scientific precepts and principles: Posture and coupled spinal motion patterns, spinal buckling from head impacts, inertial effects, scoliosis, and hyperkyphosis, as well as sub-catastrophic ligament injury spinal coupling behaviors are just some of the scientific inquiry that has born certain current biomechanical principles and precepts.
-
It should reflect current practice and educational standards: Current practice is varied; however, much of the concepts of these new subluxation types are well known. Scoliosis, for example, is understood to where it is routine to radiograph for the monitoring of curve development and measurement (i.e. Cobb angle).106 Ligament instability is a routine screening procedure in Davis’ series radiographic assessment of motor vehicle collision patients. All chiropractic students learn about some aspects of snap-through buckling in terms of sagittal spine variant positions i.e. cervical kyphosis, thoracic hyperkyphosis, etc.
Other concepts related to types of subluxation such as translations and rotations of posture are taught in a number of colleges (a number of chiropractic programs include CBP technique and its associated contemporary spinal biomechanics). It should be mentioned that although some of the concepts surrounding the new subluxation types are not fully integrated into current practice and education, this is not an inherent problem with the definitions of subluxations as presented1; it is more a problem of the lack of dissemination of relevant biomechanical information critical for contemporary knowledge related to the spine and its behavior.
-
It should be clinically meaningful: There is vast evidence of the subluxation types described as having implications for spinal pathology (i.e. osteoarthritis) and health consequences (i.e. pain symptomatology; specific disease states). All spinal displacements from ideal/normal are automatically subjected to both Wolff’s Law (bone remodels to stress)107–110 and Davis’ Law (soft tissue remodels to stress),110,111 and because these are laws and are a statement of fact, this alone provides enough ‘clinical meaningfulness’ to satisfy this attribute.
-
It should present a distinct and unique point of view: The view of rotations and translations of posture are unique rigid body movements taught as possibilities in linear algebra. Spinal buckling phenomena are from mechanical engineering. Both these concepts present unique and distinct points of view.
As shown, the 6 contemporary subluxation types all satisfy Nelson’s criterion for a valid subluxation theory (The authors each independently evaluated whether each subluxation type could satisfy each of the 6 criterion; it was unanimous that each satisfied all criterion - Table 1). Future research should be directed at the biomechanical scientific investigation of these subluxation types and the implications on health and disease.
As specifically stated by Lawrence: “Attempts to define the term (subluxation) are regularly made, only to fall afoul of political considerations rather than scientific ones112;” to this we concur. Further, because any ‘subluxation’ has a biomechanical entity, so too will its description and understanding; thus we also concur with Harrison et al.: “Because pathological changes are caused by abnormal spinal loads and functional and/or structural changes are altered positions (statics and dynamics), subluxations must be described with rotations and translations in 3D as per mechanical engineering principles and not political agreement by those without education in mechanical engineering.68”
CONCLUSION
The persistent debate about the validity of spinal subluxation needs to end. In this day and age the chiropractic profession needs to be beyond irrelevant debate and acknowledge that the lack of biomechanical, engineering and mathematical education is what has stumped the universal acceptance of contemporary subluxation concepts – not its inexistence. As presented, there certainly exists ‘vertebral subluxation,’ albeit various types; and all of these subluxation types satisfies criterion required for valid subluxation theory and scientific inquiry.