
INTRODUCTION
Osteochondrosis is a term used to describe a group of conditions that affect the patient population whose skeleton is still immature and growing.1 Osteochondrosis manifests itself in many different conditions. These includeLegg-Calvé-Perthes’ disease, Osgood-Schlatter’s disease (OSD), Sinding-Larsen-Johannson Disease, Sever’s Disease (SD), Frieberg disease, Kohler bone disease, medial epicondyle apophysitis or Panner’s disease, and Scheuermann’s disease.1 All these conditions stem from abnormal growth, injury, or overuse of the developing growth plate, surrounding ossification centers and the associated muscles attaching to these ossification centers. The exact etiology is unknown but hypotheses include repetitive trauma, genetic factors, vascular abnormalities, hormonal factors, and biomechanical factors all play major roles.2 More importantly, overuse injuries in children are more common with increased intensity of sports activities combined with a reduction in the daily physical activity of our adolescent population. This contributes to lower baseline fitness levels, thus further increasing the risk of overuse injuries.3
It is important that clinicians better grasp juvenile osteochondrosis to fully understand why these injuries occur. While preventative treatment should remain the primary focus of these conditions, it is imperative to continue to focus on the treatment aspect for such conditions. Curative treatment should no longer be to simply suspend all of the athlete’s sports activities until the symptoms go away. Rather, each athlete should be treated on a case-by-case basis with an adequate therapy program designed to alleviate his or her symptoms.
An atraumatic limp and anterior knee pain are often present in Osgood-Schlatter’s Disease. Symptoms may be further aggravated by jumping kneeling. Sever’s disease causes heel pain that is exacerbated by activity or by wearing cleats. It often mimics Achilles’ tendinitis, and current literature suggests that it is treated with activity and shoe modifications, heel cups, and calf stretches.1
Differentiating between overuse tendinopathy and osteochondrosis of the knee and calcaneus can be difficult. SD has a prevalence in sports clinics of 2-16%; however, the general population data has not been published. This disease is reported to be self-limiting, usually occurring in athletes between the ages of 8-15.4 SD cannot be diagnosed radiographically. In fact, Kose et al. state that the diagnosis of calcaneal apophysitis is a clinical decision, and radiographic assessment seems to be unnecessary; however, evaluation with this modality can assist in eliminating other conditions.5 SD typically consists of posterior heel pain, exacerbated with physical activity, and a physical examination devoid of swelling without edema or erythema.6,7 Further diagnosis may take place using MRI with gadolinium enhancement, illustrating bone marrow edema and inflammation.8
The purpose of this report is to describe the treatment delivered to multiple athletes diagnosed with either SD or Osgood-Schlatter’s Disease In each case, athletes maintained their participation in sport. In addition, treatment of OSD paralleled typical treatment of patellar tendinosis, and treatment of SD paralleled typical treatment of Achilles’ tendinosis. This retrospective case series is novel because it describes treating Osgood-Schlatter’s Disease and SD as respective tendinopathies rather than as a fracture. The objective of this study is to demonstrate that athlete’s pain levels can be managed by treating the associated musculotendinous dysfunction without having to prevent the athlete from athletic participation.
CASE SERIES
Methods
This retrospective study examined care of patients from 2011- 2016 who were treated for either OSD or SD. All patients were seen in a chiropractic department. Each athlete sought out care from the chiropractic physician. We included all cases of OSD or SD seen by the chiropractic physician. There was no recruitment involved. Patient’s whose data was used gave consent. This consisted of 11 patients ranging from 9-14 years of age. Eight of the patients were male and 3 were female. Patients who were diagnosed with OSD were treated with instrument-assisted soft-tissue mobilization to the quadriceps and patellar tendon followed by manual myofascial release to the quadriceps muscles. The tibia was then manipulated. The patients who were diagnosed with SD were treated with instrument-assisted soft-tissue mobilization to the plantar fascia, Achilles’ tendon, calf musculature and hamstrings. Manual myofascial release was then performed to the gastrocnemius, soleus, Achilles’ tendon and hamstrings. The patient’s talus and/or calcaneus was also manipulated. Kinesiology taping was applied over the treated muscles at the end of the treatment for both conditions. All patients were taught the post-isometric relaxation (PIR) stretching methodology. The patient who had SD were instructed to stretch their calf muscles and hamstring muscles with the PIR method 3 times a day. The patients who had OSD were told to stretch their quadriceps using the PIR method 3 times a day.
Analysis
No previous study on the topic of the treatment of Juvenile Osteochondrosis was found that included a combination of instrument-assisted soft-tissue mobilization, manual myofascial release, chiropractic manipulation, therapeutic kinesiology taping and an at-home exercise program. Only 11 patient records were selected since that was the total number of patients who met our criteria for inclusion. The overall improvement was measured using the Lower Extremity Functional Scale.
Results
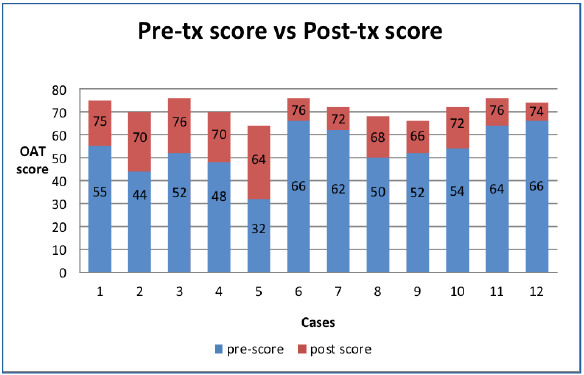
We had a total of 11 subjects, with 1 patient having both OSD and SD, for a total of 12 cases of juvenile osteochondrosis (n=12). In all 12 cases, each athlete was treated until he or she was discharged from care. All patients completed the Lower Extremity Functional Outcome assessment at the start of treatment and then again at the day of discharge. Each outcome score was reported as the Lower Extremity Functional Score (LEFS). Using the pre-scores and the post-scores, we calculated the percent of improvement that each individual athlete achieved, and then averaged the overall percent of improvement from the 12 conditions. There was an average of 22.625% improvement for those involved. This is demonstrated in Figure 1 and Figure 2. The overall percent improvement from each individual varied from 10.0-40.0% as measured by the LEFS.


Statistical Analysis
Using the mean improvement and n=12, we were able to calculate the standard deviation and confidence interval. The standard deviation was 7.05, with a CI of 13.8 to 21.8 at a 95% confidence level. The actual point difference from the LEFS score at the initial exam compared to the score at the day of discharge ranged from 8-32 points, with a minimum clinically important difference being 9 scale points. This is of significant relevance being that only one individual fell below an improvement of 9 scale points. Of the 11 out of 12 cases, the improvement demonstrated was all clinically significant. The mean improvement was 17.83 scale points, which is almost nearly doubled that of clinical relevance. The p value is < 0.01 and the result is significant at p < 0.05.
DISCUSSION
This retrospective case series was developed to highlight several aspects in which we feel there is insufficient literature making recommendations to athletes with OSD and SD. First, we sought to portray the importance of treating these conditions as a tendinopathy. Achilles’ and patellar tendinopathy is characterized by the absence of inflammatory cells, tendency toward poor healing, decreased collagen quality, disorganization of collagen, decreased tensile strength, and lack of inflammatory mediators.9–11 Furthermore, patellar tendinopathy is a painful overuse injury to the knee, common among athlete’s, particularly jumping athletes.12 Because complete rest from sport is often neither a feasible nor an effective treatment option for patellar tendinopathy in elite athletes, active treatment options should be initiated in the plan of care.12 In regards to OSD, the current literature still sites that is a common practice to rest athletes suspected to have OSD.13 However, it is important to realize the imaging findings are frequently unrelated to pain presentations and rest is not indicated in the treatment of patellar tendinopathy and could prove detrimental to recovery process.13 Instead, athletes should be allowed to continue activity as tolerated.
Often, the literature suggests suspension of activity or activity modification as the primary treatment.1 we could find nothing that even mentioned keeping athletes in play if tolerable. This case series is an example and early indication that these conditions can and should be managed using active care while allowing the athletes to continue to participate in their athletic events by treating these injuries as tendinopathies. As previously mentioned, imaging modalities and pain presentations suggest that the primary pain mechanism may be tendinopathy. There is only limited evidence suggesting that OSD and SD can be treated as tendinopathy cases, which again is what this case series demonstrates. It seems clear to us that more literature is needed to further assess the idealistic treatment methods for these conditions. Again, as mentioned in the results, of the 12 cases presented, the average improvement from the LEFS was 22.625% and not a single athlete was held out of his or her respective sport.
It sought to portray the importance of active care in regard to the treatment of both conditions while allowing the athlete to continue to participate in the sport. It also highlights the importance of treating these conditions as a tendinopathy.
Furthermore, when separating OSD from SD, the OSD population prevalence was found to be 9.8% within a Brazilian adolescent population.14 In addition, the latter study stated that 74% of the OSD population suffered from rectus femoris shortening.14 Rectus femoris shortening is common in patellar tendinopathies14 In our study, active care was geared toward the rectus femoris and the entire quadriceps muscle group, to help alleviate the tension and thus reduce the pain associated with the tendinopathy. While OSD cannot be diagnosed radiographically, attempts to validate imaging changes have been conducted using MRI.5 Patients with OSD showed significantly greater thickness (7.2 mm) in the patellar tendon at the attachment site compared to patients without (4.0 mm), which is also common in patients with pure patellar tendinopathy who have not been diagnosed with OSD.15 Patellar tendinopathy or bone marrow edema was also present in 43% of OSD patients.15 Another paper reported that 69% of patients in the progress stage and all patients who were in the late stage exhibited patellar tendinopathy, including increased thickness of the tibial insertion of the patellar tendon.16 For the latter reasons, we feel strongly that comprehensive treatment for OSD should also include treatment options for patellar tendinopathy.
Regarding Achilles tendinopathy, there is strong evidence suggesting eccentric loading exercises and extracorporeal shockwave therapy is the superior treatment method for such condition. Although extracorporeal shockwave therapy was not used by us, eccentric exercises were. There is moderate evidence suggesting the use of splinting/bracing, active rest, low-level laser therapy and concentric exercises. In-shoe foot orthoses and therapeutic ultrasound had limited evidence.1 Gajda and Cook suggest that painful eccentric squats using a 250 decline board is supported as first-line treatment for patellar tendinopathy; meanwhile, steroid injection is an inferior treatment compared to exercise interventions and currently is not recommended.12 Cleary the treatment provided in our retrospective study falls in-line with recommended guidelines for Achilles tendinopathy. Whereas, rest from the athletic activity was not prescribed to these athletes, something that the literature currently calls for SD.
Pertaining to both Patellar and Achilles tendinopathy, treatment to date may be conservative, injection-based, or surgical.12 There is strong evidence to suggest eccentric exercise for tendinopathy and weak evidence suggesting manual therapy.17–22 Furthermore, de Vries et al found that sports tape can reduce pain in patellar tendinopathy on a short-term basis.23
Manual therapy in the form of IASTM, such as Graston Technique, is currently assessed as a weak level of evidence as a result of the limitations of studies with small sample sizes, a lack of histological studies, and a lack of randomized controlled trials. However, animal histology studies have been conducted and do illustrate increased fibroblastic infiltration,24 better tissue organization,25,26 increased blood perfusion,27 and increased tensile strength of the tissue.28 Although assessed as a lower level of evidence, it may simply be because of the reduced amount of literature suggesting it may be helpful. Again, we feel this small sample size further helps support treating OSD and SD with such forms of treatment. Therefore, an argument can be made to support the combination of IASTM with eccentric exercise as a treatment for OSD and SD.
Lastly, when comparing tendinopathy vs. juvenile osteochondrosis, we mentioned that the rectus femoris remains shortened in both patellar tendinopathy and OSD. Furthermore, in both OSD and SD, the respected tendons also remain relatively short during the pubescent growth spurt, which also likely remains a cause of the pain.28 Important to note, this makes history taking essential in regard to making the correct diagnosis. Even more importantly, a thorough history optimizes prevention while minimizing the recurrence of overuse injuries. Mechanical pain is the main sign of overuse injuries.29,30 Mechanical pain is the pain generator in overuse injuries and can be divided into 4 stages:
-
Pain after physical activity
-
Pain during physical activity with no impact of function
-
Pain during physical activity that lasts all day and has an impact on function
-
Pain during all physical activities, even basic musculoskeletal functions.16
Limitations
There are a number of limitations of our study. The study is a retrospective case series that has inherent design limitations, including small sample size, reliance on documented findings, and no randomization nor blinding. Additionally, in this study, all athletes properly adhered to the recommended treatment plan and followed through with the plan of care until day of discharge. In a clinical setting, this is not always the case. Furthermore, given no control group, the results may have been due to placebo effect; therefore, more rigorous studies are needed. Again, it is also important to note that the treating chiropractor is one of the publishing authors. Furthermore, this study only used 1 Functional Outcome Assessment, the Lower Extremity Functional Scale, to address a means of improvement.
This study provides exploratory data suggesting juvenile osteochondrosis may be treated similarly to tendinosis injuries. The results can help inform inclusion, frequency and duration of care, and outcome criteria for future explanatory studies, thus providing framework from which progress future studies more robust in size as well as being controlled allowing for more realistic measures of chiropractic management strategies for juvenile osteochondrosis.
CONCLUSION
This case series demonstrates an improvement, as measured by the Lower Extremity Functional Scale, of 11 different cases of patients who had either Osgood-Schlatter’s Disease or SD. Treatment was aimed at treating the conditions as an overuse injury, providing similar if not identical care to what the current literature recommends for treatment patellar tendinosis and Achilles tendinosis. This is just a small sample size and suggests the need for further research to be performed regarding up-to-date management of Osgood-Schlatter’s and SD.