INTRODUCTION
Pudenal neuralgia (PN) is a neurological condition that was first described in 1987, where it was called perineal paralysis of cyclist. This pathology was due to the history of repetitive cycling in that patient.1 The prevalence of this condition in the general population is thought to be approximately 1%, with women affected more than men.2 Patients with PN can experience a wide variety of symptoms that are neuropathic in nature due to the various functions of the pudendal nerve. It acts as both a sensory and somatic nerve, in which sensory symptoms can include severe pain, paresthesia, and/or altered sensitivity in the nerve’s dermatome.3 In rare cases, saddle-like paresthesia is sometimes noted. This also includes change in sensation with urination or defecation.4 The change could involve pain during urination or defecation or an altered sense of urgency.4 Sexual function may also be affected, in which the diagnosis is usually then classified as restless genital syndrome (ReGS).4 Patients may have pain during sexual function, decrease in sex drive, or have constant unwarranted genital stimulation2,5 Due to the somatic function of the pudendal nerve within the act of urination and defecation, dysfunction in those processes is also possible. Furthermore, treatment for PN has been unclear. The largest series of 170 patients with pudendal neuralgia reported cure in 45% and improvement in 22% after surgical neurolysis. In the same study, imaging-guided pudendal nerve blocks offered short-term improvements in 65% of the patients.6
Correct diagnosis of PN is challenging for several reasons. As previously mentioned, there is a high variance of PN symptoms, thus making the diagnosis of PN often difficult for clinicians assess and diagnose. It can also can be difficult to diagnose because it can occur around ligamentous, osseous, and musculotendinous structures within the posterior hip region.7 The pudendal nerve exits the greater sciatic foramen and continues to travel over the sacrospinous ligament and through the pudendal canal, known as Alcock’s canal, which is formed by the sacrotuberous ligament and obturator fascia. The nerve then reappears inferior the the pubic bone to innervate the perineum and genitalia.8 The pudendal nerve can become entrapped at any location throughout its journey. The most common location is between the sacrospinous and sacrotuberous ligaments at the ischial spine. It is also common for the obturator internus muscle to compress the pudendal nerve medial to the ischium.8 Figure 1 is an anatomical picture of the pudendal nerve taken from Hough et al.

Lastly, diagnosis may be challenging as it can be caused by a wide variety of reasons. This includes mechanical compression (the most common cause), repetitive cycling, iatrogenic factors following surgical procedures, muscular entrapments, various tumors, and ganglion cysts to name several.1,6,9–12
Upon physical examination, tenderness to palpation can occur at the greater sciatic notch, medial to the ischium, over the obturartor internus muscle, or near the sacrotuberous and sacrosponous ligaments.3 Sitting generally increases pain except when sitting on a toilet seat. Unlike a flat surface, a toilet seat does not add increased pressure in the area medial to the ischium.7
The purpose of this case report is to demonstrate a treatment approach in which multimodal chiropractic care was used to treat a patient with PN. Currently, there is little evidence in the literature discussing multimodal chiropractic intervention for PN. This case provides evidence towards the possible presenting symptoms of PN and complicating factors, as well as a treatment plan that was successful in resolving the condition.
CASE REPORT
A 24-year-old male sought chiropractic care for persistent left-sided medial gluteal pain and associated proximal thigh and genital paresthesia. This began after a period of intensive physical activity, specifically squatting, and had lasted for greater than 3 years. At rest, he described his left-sided gluteal pain as dull, rated 3/10 on the Visual Analogue Scale (VAS). He described frequency as continuous with an occurrence 80%-100% of the time. Provoking factors included straining, ejaculation, bowel movements and sustained sitting. These activities increased pain and paresthesia in his penis and posterior medial thigh. He was unresponsive to antibiotic regimens, conventional physical therapy, pelvic floor therapy, and activity modification. He reported regular use of a donut pillow and heating modalities for relief. Physical activity had been limited due to increased symptoms mirroring activity levels. He denied use of current medication, past medical and surgical histories.
Of note, he had been referred for chiropractic care after an online search he conducted found a case report by Olson et al, about pudendal neuralgia treated with multimodal chiropractic interventions. When reading the report, he believed his symptomatology was similar to that reported in the case and sought out the authors for guidance. After enacting certain stretches to address his obturator internus musculature, he noticed amplification of his symptomatology. The corresponding authors helped refer the patient to an appropriate chiropractor in his area.
His deep-tendon reflexes were symmetrical bilaterally in the upper and lower extremities. Coordination and motor strength were normal. Sensation was normal in his lower extremity. He opted not to undergo sensory testing within his perineal region. Orthopedic evaluation of lumbar spine and pelvis were negative. Orthopedic evaluation of left hip demonstrated equivocal findings of irritating, dull, gluteal pain. Lumbopelvic ranges of motion were minimally restricted. Digital palpation of left-sided obturator internus muscle elicited pain referring into the patient’s penis and adductor musculature to approximately the proximal one-third of the posteriomedial thigh. A provisional diagnosis of pudendal neuralgia was given.
He was treated conservatively 2x/week for the first 2 weeks, and 1x/week for the next 3 weeks for a total treatment period of 5 weeks and 7 visit. Initial treatment consisted of myofascial therapy to the left obturator internus and surrounding musculature and spinal manipulative therapy of the lumbopelvic region. Incorporation of nerve flossing techniques were provided at the third visit and dynamic cupping was added on the fifth date of service.
After the initial visit, he reported exacerbation of buttock, penile, and proximal medial thigh pain for a period of 3 days. After 4 days, his symptoms began to improve over the course of the week. At the second visit, he further indicated at that there were times in which he even felt as if he were normal again. There was diminished irritation with sitting and physical straining. Over the next 3 weeks, myofascial therapy continued, in addition to incorporation of dynamic cupping of posterior gluteal musculature over ischial tuberosity and into the proximal hamstring. Patient was encouraged to engage in physical activity over this time period. Upon the final visit, patient reported experiencing no pain or paresthesia at rest or with activity. He reported continued mild symptomatology into his penis but now associated only with bowel movements. He continued cross-friction massage over the obturator internus location mirroring myofascial release procedures, which he reported provided prophylactic relief. Hewas discharged at this time. A follow-up conversation 1.5 months later revealed he had completely resolved all symptoms at rest and during straining. Hereported a full restoration of function without pain or paresthesia.
DISCUSSION
Apart from 2 other case studies published by Olson et al, this is 1 of the very few reported cases in the literature documenting the treatment of PN via multimodal chiropractic management. The results here demonstrate that the patient had a clinical diagnosis of PN with a measurable improvement in his symptoms. This case report should be important to all health care providers since conservative care for PN is not well documented. Key to the proper treatment of this condition falls with first establishing the proper diagnosis. In diagnosing PN, the essential criteria, which have become the gold standard for clinicians to use when diagnosing or ruling out PN, includes:
-
pain in the sensory innervation of the pudendal nerve
-
pain worse with sitting
-
the patient is not disturbed at night by the pain
-
there is no objective sensory loss on clinical examination
-
there is a positive response to an anesthetic pudendal nerve block3,4
Complementary diagnostic criteria include numbness in the sensory innervation. Exclusion criteria includes: exclusively coccygeal, gluteal, pubic or hypogastric pain, pruritus, and exclusively paroxysmal pain.3,4 This criteria is known as the Nantes Criteria and was developed in 2008 by a group of clinicians to aid in diagnosing this condition.4 The 5 components of Nantes Criteria highly suggest a case of PN if the all are present. However, due to the wide variety of presenting symptoms from case to case, use of the Nantes Criteria in combination with a proper history and quality exam will allow the best chance for a proper diagnosis.3
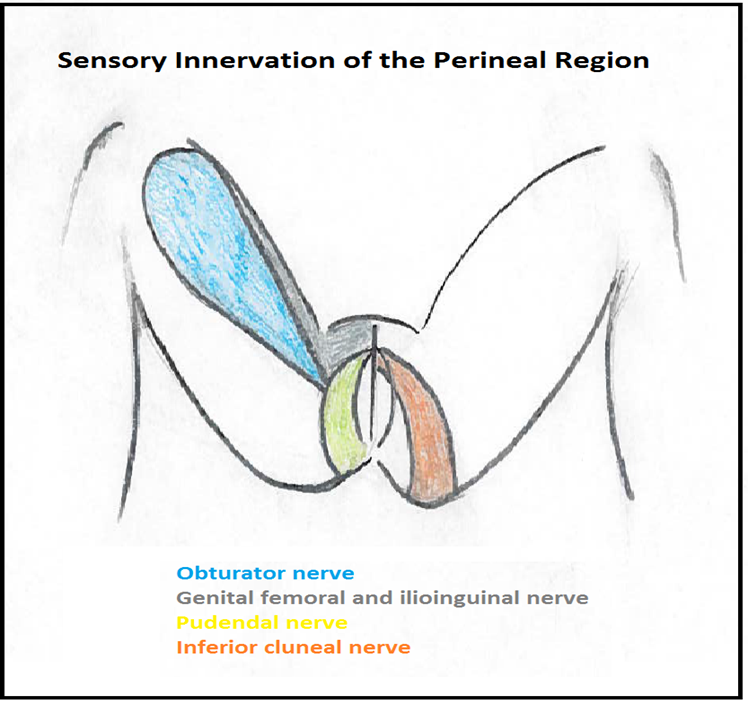
As mentioned, proper diagnosis of PN may be challenging. Figure 2 is the sensory distribution of the pudendal nerve.
.png)
Sensory innervation includes the area between the anus and penis or clitoris.3 Symptoms from a pudendal nerve injury or entrapment can be purely sensory, purely motor, or a mixture of the 2. Because the pudendal nerve also involves the genital region, patients may feel apprehensive about discussing this condition with their medical providers, yet alone have sensory testing performed in this region. Simple testing between sharp and dull sensations along the regions of the pudendal nerve, obturator nerve, genital femoral nerve, ilioinguinal nerve and inferior cluneal nerve may help physicians get a very clear picture of what nerve likely is being compromised. However, as in this case, the patient declined to have sensory testing performed. Furthermore, a chiropractic physician may argue that through the subjective and objective examination, not to include sensory testing, enough findings warrant a working diagnosis of PN and sensory testing would not change the treatment that the provider would be administering.
It is important to note that most neuralgias resolve fairly quickly, often within 1-2 months; however, there are those that may last longer. These can be very traumatic for the individual involved.10,13 In women, the most frequent finding of dysfunction is bilateral decreased sensation to the perineum and labia in and perineum, while scrotal involvement is common in males.10 Symptoms of pain usually resolve quickly, while those that are sensory in nature tend to last longer and may accompany sexual dysfunction as well.13 Anatomically, the obturator internus is a common entrapment site of the pudendal nerve due to muscular spasms.14 Without intervention, patients can experience a wide variety of symptoms that are neuropathic in nature due to its various functions as a sensory and somatic nerve. Sensory symptoms can include severe pain, paresthesia, and/or altered sensitivity in the nerve’s dermatome.3 In rare cases, saddle paresthesia is noted. This also includes change in sensation with urination or defecation.4 These symptoms can be devasting to an individual.
There is emerging clinical evidence suggesting that PN may be treated conservatively with chiropractic care to allow full resolution of symptoms. However, it is also possible that the patient here may have improved because of the natural course of the disorder or other factors that were not measured or that we were unaware of. Because this was a single case report, we cannot generalize the effects from this patient to other patients with pudendal neuralgia nor do we understood what factors were precisely responsible for the outcomes. In this case, multimodal chiropractic care was used, and it very well could have been only aspect of the treatment protocol that actually helped. Because pudendal neuralgia does follow a recurrent and continual natural course4 we hypothesize that the multimodal chiropractic treatment was at least partially responsible for the patient’s improvement. Further observation and experimental research with large sample sizes are needed to determine what the effects of multimodal chiropractic care has on patients with pudendal neuralgia. This case report is notable to health care providers, especially doctors of chiropractic, because of the low amount of experimental research on effective conservative treatment of pudendal neuralgia.
CONCLUSION
This report presents a case in which the obturator internus was thought to be causing a pudendal nerve entrapment, which led to the patient suffering from PN for 3 years. The patient responded favorably to multimodal chiropractic intervention. This adds to the initial reports from Olson et al that demonstrate the resolution of PN using conservative chiropractic care, allowing the patient to avoid more invasive treatment options such as a pudendal nerve block or surgical intervention. The results suggest that the treatment described in this case report could potentially aid in the recovery of PN and warrants further study.