




INTRODUCTION
Thoracic hyperkyphosis (THK) is a spinal subluxation or deformity featuring the exaggeration of the normal physiologic thoracic kyphosis.1,2 Often referred to as age-related hyperkyphosis in adults, it is a structural deformity subluxation that occurs when the physiologic kyphosis surpasses some threshold becoming pathologic.
Since the vital organs are situated within the thoracic cavity, any deformity of the thoracic spine, enough to change the internal dimensions of this cavity, will necessarily involve the vital organs. For this reason, THK is associated with many ill health effects3–30; the direst being early demise17–22 (Table 1).
The prevalence and incidence of THK in older adults is estimated to be 20-40% for men and women.1,2 Thus, THK is relatively common. Recent clinical evidence suggests a role for nonsurgical approaches to both delay its progression and to reduce the deformity.2 Indeed, treatment methods aimed at reducing the deformity and therefore its associated health consequences are needed to reduce the health burden on society.
Although there are clinical trials demonstrating improvement in THK by back extension exercise programs,31–37 most of these studies do not use the gold standard use of x-ray to measure pre-post treatment effects.1 Alternative methods to measure the thoracic spine curvature may be reliable, but do not characterize the true curve that is only attainable via radiography. Further, the contribution of compression fractures, which are often associated with THK, is an important structural finding to rule out prior to initiating a rehabilitation program as their presence will significantly limit treatment success.38
Recently, there has been cases presented documenting successful outcomes in THK patients as treated by Chiropractic BioPhysics® (CBP®) technique, such as Oakley et al.39 Since the CBP approach to correcting structural alignment to the spine has been demonstrated for the cervical40–46 and lumbar areas,47–50 we sought to identify the clinical evidence for THK. Thus, the purpose of the present study was to systematically summarize the clinical evidence documenting the reduction of THK by CBP technique.
METHODS
We searched Index Medicus, and the Index to Chiropractic Literature using search terms relating to the thoracic disease entity: ‘thoracic hyperkyphosis,’ ‘thoracic spine,’ ‘hunchback,’ ‘dowager’s hump,’ 'Scheuermann’s disease,’ and linked these with CBP technique: ‘CBP,’ 'Chiropractic Biophysics,’ and ‘structural rehabilitation.’
All located clinical studies had their references searched. Only peer-reviewed references that detailed the clinical treatment of THK patients by methods typically employed under the umbrella of CBP technique were included.
All located references were screened for clinical data details, including patient age, gender, number of treatments, duration of treatment, symptoms reported, pain and disability questionnaire scores, thoracic kyphosis radiographic measurement and improvement from treatment, treatment details including exercise, adjustment and traction descriptions as well as any post-treatment follow-up.
RESULTS
Seven clinical studies documenting the treatment of THK patients by CBP methods were located38,39,51–55 (Table 2). There were 4 single case reports,38,51–53 2 case series (n=1039; n=354), and 1 randomized clinical trial55 on treating cervical hypolordosis that reported improvements in thoracic kyphosis. All located sources (except the RCT) described the patient treatment protocol classic to CBP technique,56,57 namely mirror image thoracic extension traction (Figure 1) and exercises (Figure 2), as well as some type of spinal adjustment (mirror image for THK) (Figure 3) and/or classic spinal manipulative therapy. The RCT was specifically investigating cervical extension traction for patients with lumbosacral radiculopathy, where a control group and a study group both received TENS therapy and hot packs, treatments not specific to CBP methods.




In general, there were great variations in number of treatments (12-94), duration of treatment (4 weeks to 13 months), magnitude of thoracic kyphosis correction (9-23°; 3° for patients in the RCT), and age of patients treated (15-68 yrs.). The 2 case series reported a similar kyphosis reduction of approximately 11° achieved in a similar time frame of an average of 9-10 weeks of treatment. Overall, in the 17 cases (not including the RCT), there was an average reduction of THK of 12° over an average of 32 treatments, over an average of 14 weeks. There was an average 3-point drop in the 0-10 point pain rating scale. Although not shown in Table 2, all studies demonstrated improvements in quality of life measures.
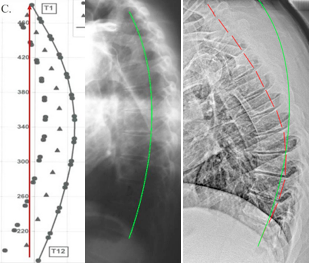
The RCT reported a 2.9° reduction in THK after 30 treatments over 10 weeks in 40 patients (Not shown in Table 2). The unique aspect about this trial is that there was reduction in THK despite having treatment not specifically directed at the thoracic spine. These patients received cervical extension traction using the cervical Denneroll™, TENS therapy and hot packs. The thoracic spine was measured via a raster-stereographic method. All other studies demonstrated a reduction in THK curvature as measured from the lateral thoracic radiograph using the Harrison posterior tangent method. This method measures the global kyphosis absolute rotation angle by drawing lines contiguous with the posterior vertebral bodies and has a standard error of measure ≤2.5°, and an inter- and intra-class correlation coefficient >.96.58 The different studies did report different endpoint vertebrae used in the thoracic measurement (i.e. T1-T12; T2-T11; T3-T10; T2-T12) (Figure 4).

In comparing the thoracic alignment to a normal/ideal, all studies (except the RCT) illustrated THK against the Harrison spinal model.59,60 Using the PostureRay X-ray exacting software (PostureCo., Inc., Trinity, FL, USA), the normal Harrison model is incorporated into the radiographic analysis, where any digitized patient radiograph gets illustrated against the ideal alignment. This makes postural subluxation diagnosis simple and obvious to the doctor and patient (Figure 5).

Only 1 case report included a patient follow-up and found stability of the initial correction.53 Interestingly, the series by Fedorchuk and Snow54 treated asymptomatic patients but reported improvements in SF-36 quality of health measures as well as 2/3 of the patients had increases in peak expiratory flow and forced expiratory volume; key measures of vital capacity.
DISCUSSION
This study systematically reviewed the scientific evidence of all clinical studies
documenting the reduction of THK by CBP technique. Although the clinical evidence is limited, there is promising evidence that the mirror image application of thoracic extension exercises, spinal traction as well as mirror image spinal adjustments, demonstrates to be an effective rehabilitative approach for the reduction of THK.
Although there are trials demonstrating back extension exercise programs may decrease THK,31–37 spinal traction targets the viscoelastic structures including the intervertebral discs and spinal ligaments.61,62 Stretching the spine in its exact opposite or mirror image orientation is the most direct and effective way to attempt to reposition the spinal structure towards a biomechanically optimal alignment. Thoracic hyperextension traction achieves this for those with THK deformity. As demonstrated in low back ligaments, optimal traction time is 20 minutes, though creep elongation may occur as early as 5 minutes.61 Thus, CBP trained doctors perform spinal traction to their patients from 10-20 minutes per session56,57 based on biomechanical models of soft-tissue deformity under loading scenarios.
It is important to realize that thoracic extension exercises do not achieve the same effect as a sustained extension stretch for 10-20 minutes. Obviously, exercises are dynamic and even if held at an endpoint in movement, for example, a back extension, it will be only held for as long as the patient has the energy to hold (not 10-20 minutes), but more importantly, an active thoracic extension stretch will not achieve a maximal extension stretch to the targeted anterior longitudinal ligament and anterior disc spaces. Traction is necessary to achieve creep (deformation over time62) and plastic deformation (structure permanently deforms62) to reduce the thoracic curve, and this can only be achieved with thoracic hyper-extension with the patient relaxed and without muscle engagement (Figure 1).
Since CBP technique incorporates multiple therapeutic modalities into a typical treatment program, it avails itself to be more effective versus monotherapy approaches. On the topic of low back pain, for example, Bogduk concluded that most monotherapies simply don’t work or have limited efficacy.63 Thus, multiple therapies targeting the various tissues in a comprehensive and cohesive rehabilitation program including the extension traction, exercises, as well as spinal manipulation that CBP technique incorporates logically would seem to provide better patient benefit (i.e. greater reduction of THK).
We could only locate 2 trials documenting pre-post thoracic spine x-ray improvements following an exercise program. In a small trial, Itoi and Sinaki31 evaluated a 2-year exercise program in estrogen–deficient women aged 49-65. Although they found no statistical difference between the control and exercise groups, upon re-analyzing their data they noted that those women who increased their back strength regardless of original group placement, did improve their kyphosis angle by 2.8°. In the only other trial, Katzman et al. found a 3° improvement in the kyphosis angle in seniors performing an exercise program for 1 hour, three times a week for 6 months, compared to a control group.32
The CBP RCT on restoring cervical lordosis to treat patients with chronic discogenic lumbosacral radiculopathy reported a 3° reduction in THK after 30 treatments over a 10-week period using the Denneroll for cervical extension traction. It should be noted that although the thoracic spine was not specifically treated for the purpose of reducing THK, the improvement was equal to the amount of improvements in both the exercise only trials.31,32 This is likely because the patients were in a supine position while performing cervical extension traction; as a flat bench may provide a small but significant ‘mirror image’ traction effect on a patient with THK. Another reason may be that increasing the adjacent cervical curve may have reciprocal effects on encouraging a realignment of the thoracic curve towards improved physiologic posture. More research is necessary however, to elucidate full-spine responses to spinal traction applications in CBP technique.
Considering the incidence of THK in common practice is high, it is surprising that the treatment efficacy has been found to be highly subjective.64 It is strongly recommended that the gold standard x-ray measure be used to quantify thoracic kyphosis in those with THK, to provide a precise means of monitoring treatment efficacy. Further, because vertebral compression fractures may be associated with those with THK, it is the only practical method to screen for the presence or absence of vertebral bone deformities.
Although it is important to screen for vertebral compression fractures in patients with THK, it is known that up to 70% of THK patients may be void of vertebral fractures.4,65 As discussed, the THK spinal subluxation is a serious health compromising deformity, and as Kado et al. state “the realization that hyperkyphosis is not synonymous with vertebral compression fractures may lead to interventions specifically targeted at improving posture, possibly resulting in reduced mortality rates.”19
For such a serious health disorder, it is surprising that typical treatment modalities used in the treatment of THK are diverse.63 For example, many physiotherapists based their management of hyperkyphosis on their undergraduate education alone.63 However, considering the average reduction in THK was 12° for the CBP treated patients versus 3° reduction in 2 exercise only trials, the CBP multimodal program may prove to be the ideal treatment approach. Obviously, at this point in time, more research is needed to clarify the best treatment approach for THK and future studies need to further evaluate multimodal treatment programs particularly to include the combination of thoracic extension exercises and traction methods.
It should be noted that traditionally the views toward x-ray use focus on concerns over radiation exposures and possible future cancers. Recently, however, x-ray safety has been thoroughly substantiated. In fact, there is no risk for future cancers from the amount of radiation exposure from spinal x-rays; this is because they are 100 times less than the threshold for inducing cancer (leukemia)66 and our bodies may experience health improvements from such low dose exposures.67,68 Thus, there should be no concern about theoretical radiation risks in a risk-benefit ratio over the choice to image patients with THK; spine radiographs should be routinely taken for such patients.
CONCLUSION
Although limited, there is promising evidence that the CBP technique approach for the reduction of THK by application of mirror image traction and exercises as a part of a multimodal rehabilitation program may prove very effective. As opposed to the limited evidence offered by monotherapy exercise trials, the application of thoracic hyperextension traction combined with hyperextension exercises is logical from a biomechanics standpoint. A randomized clinical trial to further evaluate the CBP approach to treat THK is warranted.