
Introduction
A significant amount of evidence about Chiropractic BioPhysics® (CBP®) technique exoists in the scientific literature.1 The CBP NonProfit website (www.idealspine.com) lists 277 formal, peer-reviewed publications.1 Recent systematic reviews have been published outlining the clinical evidence of CBP methods to increase cervical lordosis,2 increase lumbar lordosis,3 and reduce thoracic hyperkyphosis.4
CBP is based on the assessment of the 3-dimensional analysis of the head, thorax and pelvis in terms of rotations and translations about or along the x, y, and z-axes.5 Thus, there are many postural subluxations; in fact, Harrison has calculated over 1.5 million different combinations of misaligned or subluxated postures based on this system.6 One of the postures for which clinical reports exist is for the reduction of lateral head translation posture, a coronal offset of the head over the midline of the thorax (Figure 1).7
Oakley and Harrison determined that approximately 50% of patients with neck pain and/or headaches have a lateral head translation posture.8 They suggested lateral head postures exert asymmetrical forces onto the cervical spine tissues, which in turn contribute to neck pain and headaches. This is supported by their research on 146 patient x-rays where the older the patient was, the longer they had suffered pain and the greater the lateral head translation magnitude.8 Thus, lateral positioned head postures may be a clinical important finding that is amenable to treatment by CBP methods.9
The purpose of this review is to characterize the evidence of CBP technique in the reduction of lateral head translation (also referred to as pseudo-scoliosis) and its effect on pain, disability and quality of life.
Methods
A review of the CBP NonProfit citation listings1 was performed for clinical papers reporting on the reduction of lateral head translation postures. Any clinical study type was included. A search on both Pubmed and the Index to Chiropractic Literature (ICL) was also done using the keywords lateral head translation or pseudo-scoliosis; no papers were located that were not already listed on the CBP NonProfit site.
To be thorough, CBP case reports were searched for this postural correction even if not mentioned in the title; for example, when the emphasis was on another postural subluxation. References of located studies were searched. Searches were also performed in chiropractic-dedicated conference proceedings, and experts were contacted on the topic of interest to locate further studies (e.g. authors of located cases).
Information extracted from located studies included age and sex of patient, chief complaint, number of treatments, time duration of treatment, treatment specifics including traction set-up, traction duration, exercise protocol, adjusting protocol, as well as pre- and post-treatment magnitude of coronal offset and corresponding cervicodorsal (CD) and Rz angles (Figure 1).
Based on the data from located cases, we sought to evaluate the relation between magnitude of correction of lateral head posture to treatment number and treatment duration. This was done using correlation coefficients as calculated using the statistical program R.10

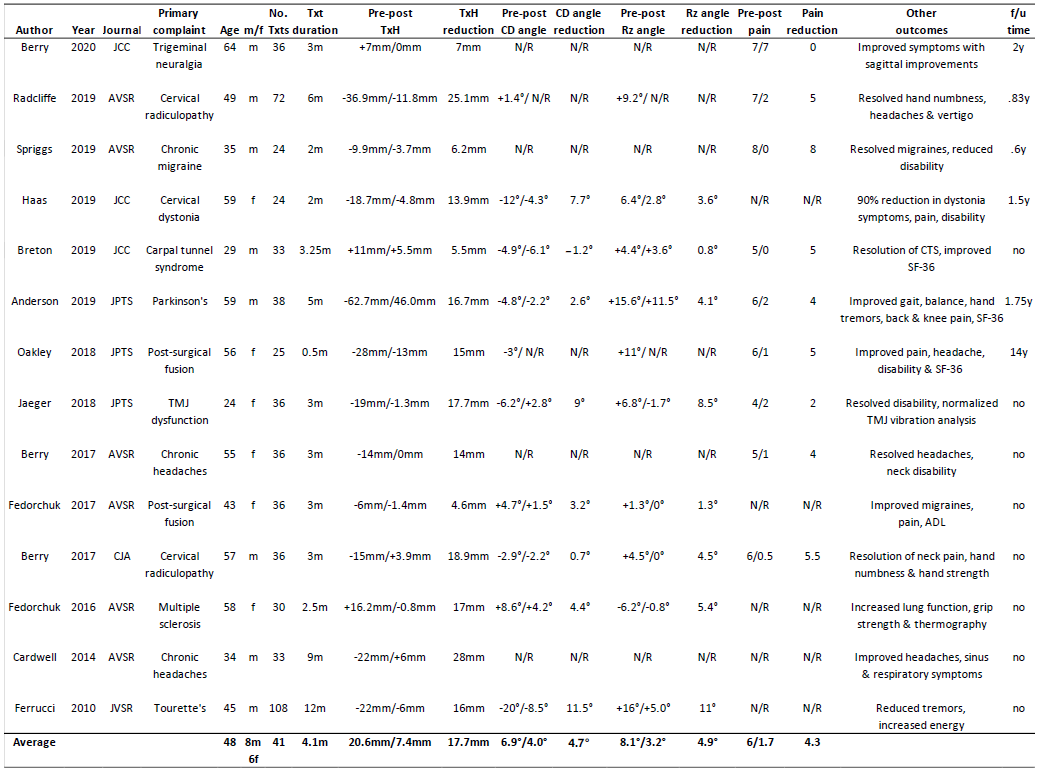
Our search of the CBP NonProfit site located one non-randomized controlled trial (nRCT)9 and 14 case reports11–24 (Table 1). Searches in Pubmed revealed 5 hits and ICL 23 hits; all were already located from the CBP NonProfit site. No other cases were located by searching conference proceedings, references from included cases or contacting case report authors.
Results
The clinical trial reported a 7mm reduction in lateral head translation after an average of 37 treatments over 13 weeks in 51 chronic neck pain patients.9 There was a 3.3-point drop in pain rating (4.0/10 to 0.7/10) during the treatment while there was no change in head posture or pain rating reported in the control group of 26 untreated patients with chronic neck pain.9
The 14 located case reports (Table 1) showed an average lateral head translation reduction of 17.7mm after 41 treatments over 4.1 months.11–22 The corresponding reduction in CD and Rz angles were 5.0° and 4.9°, respectively. The average age was 48 and the average reduction of pain was 4.3 points on a 10-point rating scale (6.0/10 to 1.7/10). The reduction of lateral head postures successfully relieved symptoms in patients with cervical radiculopathy,12,21 chronic migraine,13 cervical dystonia,14 carpal tunnel syndrome,15 Parkinson’s,16 post-surgical fusion,17,20 TMJ dysfunction,18 chronic headaches,19,23 multiple sclerosis,22 and Tourette’s.24 Many of the cases also reported improvements in functional measures (e.g. cervical range of motion), disability (e.g. neck disability index), and quality of life (e.g. SF-36). There were no adverse events reported.

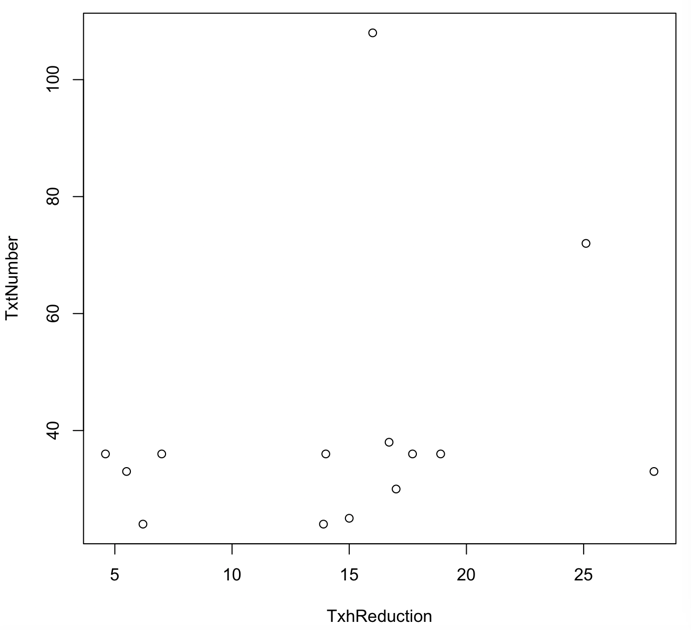
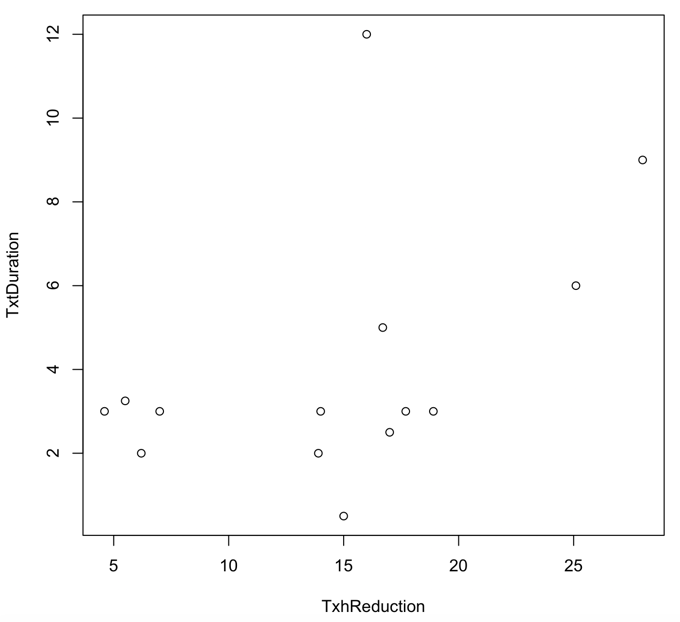
Correlations between lateral head posture correction magnitudes and treatment number and treatment duration was .27 and .47, respectively (Figures 2 and 3). As seen, most patients received less than 40 treatments (Figure 2: 12/14 cases) and most were treated for less than 4 months (Figure 3: 10/14 cases).
_and_lateral_head_translation_correction_in_mm.png)
_and_lateral_head_translation_co.png)
Discussion
This review has summarized the details from one non-randomized controlled trial and 14 case reports which have documented the reduction of lateral head translation postures in the treatment of various cranio-cervical disorders. The average reduction of lateral head posture was 7mm after 37 treatments in the trial9 and averaged 18mm after 41 treatments from the 14 individual cases.11–24 The individual cases demonstrated that a significant neck pain reduction (>4 points) can be achieved by reducing a lateral head postures after approximately 40 treatments over 4 months (Figures 2 and 3).
It is perhaps surprising that the correlation between lateral head reduction magnitude and treatment number was low (r =.27),25 but this may be because some of the cases did a re-assessment after a larger than average treatment number (i.e. Ferruci, 108)24). The correlation between lateral head reduction and treatment duration approached a moderate strength at r = .47 and would have been stronger perhaps if some of the cases did a re-assessment sooner than at a long-time follow-up (i.e. Cardwell (9-months)23 and Ferruci (12-months)24). The lack of strong correlations are likely due to the fact that in achieving significant clinical outcomes, the magnitude of correction can be small yet still provide an improvement where the biomechanical stresses and strains are reduced beyond some threshold sufficient enough to relieve the associated symptoms.
It has been noted that most treatments for neck disorders have limited efficacy and this is particularly evident after long-term, post-therapeutic follow-up.26 The nRCT had no long-term follow-up and only 6 of 14 cases included a follow-up. Of the cases that did include a follow-up,11–14,16,17 the involved patients remained well and the corresponding spine improvements were maintained. Future studies of CBP clinical treatments for this posture need to include long-term outcome data.
As the scientific evidence for the manual therapies is limited,27 lower forms of evidence must suffice; thus, case studies can play a role in guiding practice.28,29 Based on the magnitude of corrections divided by the treatment number, the data indicates a range of 0.2-0.4mm’s of correction per treatment. Therefore, a 1mm reduction requires 2.5-5 treatments. This is useful information for a treating chiropractor utilizing these methods to estimate a range of treatment number based on the existing evidence base; for example, a patient presenting with a 20mm lateral head translation would require 50-100 treatments for its reduction.
In the only prevalence study of lateral head postures, Oakley and Harrison found a prevalence of 53% in a sample of 335 neck pain and/or headache patients.8 They also suggested that lateral head postures exert asymmetrical forces onto the cervical spine tissues, which in turn contribute to neck pain and headaches.8 It is conceivable that asymmetrical forces on the cervical structures may also contribute to other symptoms such as TMJ disorders.18 We concur with Oakley and Harrison that because neck pain etiology remains controversial, lateral head shift postures are likely an unrealized factor in the causation of neck pains, headaches and other cranio-cervical symptoms in patients presenting with these postures.
Because neck pain is a significant contributor to disability,30 and due to the wide variation in assessment methods and treatment approaches,31 the screening for lateral head postures seems like a wise recommendation particularly since the data presented show evidence of an effective treatment intervention utilizing CBP methods. It must also be stated that although postural photogrammetry may show this posture, only radiographic assessment allows for a more precise assessment and measurement including the CD and Rz angles and to confirm a normal spinal S-configuration coupling pattern or not.7
Limitations to this review is that there was a limited number of cases, including only one trial. The generalizability of the data is also limited as treatment was typically provided to mid-aged patients. Since CBP methods uses a multimodal treatment approach, it is not known which procedures contributes to which extent to pain reduction and other positive clinical outcomes. Presumably it is the reduction of the spinal deviation that provides the long-term successful outcomes as has been shown in the correction of cervical and lumbar lordosis,2,3 however, this needs to be substantiated for lateral head translation postures. Future research in the treatment of lateral head translation postures also should include long-term follow-up and document disability and quality of life data.
CONCLUSION
There is a limited but evolving evidence-base supporting the unique mirror image approach to reducing lateral head translation postures by CBP technique methods. Since there is little consensus in the assessment and treatment of cervical spine disorders, the routine screening for head postures would allow for routine definitive diagnosis of those having a lateral head posture for which there is a specific treatment.