INTRODUCTION
Neck pain is a common global issue that has a significant impact on the UK’s national health perception. It adds considerable economic costs to the national health service.1,2 Safiri et al found that the largest percentage increased change in age, incidence and years lived with neck pain per 100, 000 were in the UK, recorded at 14.6%, 9.1%, and 14.2% respectively.2 They also found that the point prevalence globally was highest in females between 45 and 49 years of age2 Neck pain is the second most common complaint seen by chiropractors worldwide, responsible for 22.5% of all chiropractic patients.3 The General Chiropractic Council (GCC) stated in their counterfactual report that 1,005,000 patients saw a chiropractor in 2009.4 Patient numbers were projected to increase to 1,043,000 over the next decade, meaning approximately 234,675 patients are currently visiting chiropractors in the UK for neck pain per annum.
Spinal manipulative therapy (SMT) has been shown to be an effective treatment intervention for patients with neck pain.5,6 The risks of cSMT however, are not fully understood.7,8 with adverse events following cSMT being well documented in the literature7,9–17 Adverse events from cSMT are defined as mild, with short-term, non-serious, transient/reversible effects; moderate, that can be medium to long-term and described as distressing; and major events are described as long-term, serious events that require further treatment.18
Adverse events from cSMT are described in the literature as common7 and include increased pain, stiffness, dizziness, tiredness, headache, nausea, neurovascular compromise, vertebral artery dissection, stroke, and death.7,15,19–27 Cagnie et al investigated the frequency of side effects following SMT using lifestyle factors such as sex, smoking status, and existing medical conditions.28 They concluded it is theoretically possible to reduce the frequency of side effects following SMT if the patients at risk can be correctly identified. Cagnie et al did not use any form of pre-treatment diagnostic imaging to assess their participants of underlying risk factors.28 Jenkins et al found that 30% of cervical spine x-rays obtained in chiropractic clinical practice will find anomalies that may alter the application of spinal manipulation.29 Cagnie et al only assessed side effects following the first treatment, and the authors fail to provide data on how to identify those patients at risk of side effects.28
Some researchers have concluded that cSMT should be abandoned due to the risk of potentially catastrophic events such as neurovascular compromise30 Wand et al reference a systematic literature review of adverse effects of cSMT by Ernst11 The Ernst review paper was reviewed during the literature review process for this current study but was excluded for being conducted by a single researcher, failure to provide details on the appraisal criteria, and high level of bias as per the Joanna Briggs critical appraisal checklist.31,32
There is disagreement within the chiropractic profession regarding the appropriate use of x-rays in clinical practice for both diagnostic and screening purposes.33–37 One side of the debate are authors advocating the use of diagnostic imaging for “Red Flag” evaluations only.38–40
The basis of the “Red Flags” only stance for spinal x-rays hinges on 2 premises that are specifically for the use of x-rays for cases of acute low back pain39 The first premise is that 90% of acute episodes of low back pain will spontaneously resolve within 4-6 weeks.41–45 The claim of 90% of low back pain cases resolve within 2 months originates from Fry. Fry conducted a retrospective review of records of 125 patients who presented to a general practice surgery with low back pain and concluded that 82% made a complete recovery within four weeks.45,46 However, Fry included patients who failed to return to the clinic for a follow-up appointment in the recovered group.45 Similarly, Coste et al reported 90% of 92 patients with low back pain experienced spontaneous resolution of their symptoms within 2 weeks.47 Several flaws exist within the Coste et al study, notably a lack of detail regarding if the participants sought the treatment of another healthcare professional, or any self-directed treatment the participants may have employed, such as the application of ice, or exercise.
The second premise states that serious pathologies of the spine are rare and collectively represent approximately 6% of all causes of low back pain.48 The assumption, therefore, is that x-rays are not required unless serious pathology is suspected, such as infection, fracture, dislocation, cancer, or an inflammatory disease process.39
Contrary to the first premise, Kӓӓriӓ et al in a prospective longitudinal study of 902 participants with follow-ups at 5, 10, and 28-years concluded that 88% remained symptomatic 28-years later.49 Several authors have concluded that the greatest predictor of low back pain in adolescence and adulthood is low back pain during childhood.50–56
Signs and symptoms of patients who present to any health care professional can vary depending on the stage of the disease/pathological process57 In cases of musculoskeletal disorders, such as cervical spondylosis, many patients are asymptomatic.58 However, once the condition progresses to affect neural or vascular structures, it has 3 symptom complexes: neck pain, radiculopathy, and myelopathy.57–59 Beck et al discuss spondylosis, concluding that chiropractors must be aware of the discrepancy between clinical signs and symptoms of some musculoskeletal disorders and there radiographic appearance, thus relying on symptoms alone may not be appropriate.60 Cases can seem advanced in symptomatology and disability yet appear mild or moderate on radiograph. The pathological process of spondylosis can lead to segmental instabilities and kyphosis,57,58 which are listed in the literature as contraindicated to cSMT.61
One reason for limiting the use of x-rays in the chiropractic profession is the accusation of inappropriate or overuse of x-rays by the profession and thus unnecessarily exposing patients to ionising radiation.62 This perspective has already influenced the chiropractic profession, with a ban on chiropractors having x-ray facilities within their clinics in The Netherlands.63 Notwithstanding, until 2010 the GCC and its Professional Conduct Committee found 26 instances of unjustified exposure to ionising radiation spanning 8 years.4 The GCC then extrapolated these data to show this equated to a total of 3.25 instances per annum or approximately 0.000323% of the total population of patients under chiropractic care in the UK.4 The GCC annual report a decade later found a total of 6 complaints of “lack of clinical justification for investigations/x-rays.”64 The risk of cancer from chiropractic x-rays of the lumbar spine has been estimated to be 2.75%, which equates to quality-adjusted life years lost through cancer from chiropractic x-rays to be 0.0011.4 However, this is specifically for lumbar spine exposures, which the UNSCEAR 2000 report states delivers an effective dose to the patient is 1.8 milli Sieverts (mSv), whereas cervical spine examinations are recorded at 0.27 mSv.65 Thus, cervical spine x-rays have a smaller impact on patient lifetime cancer risk. Along with a plethora of literature questioning if low dose and low dose rate ionising radiation carries any risk to the patient.66,67 Vaiserman et al state there is no increased cancer risk from diagnostic examinations using <100 mSv67 Schultz et al concluded from their systematic literature review that doses from as many as 20 CT scans are unlikely to result in cancer.68
Several attempts have been made to determine the appropriateness of SMT using x-rays.33,69–71 Beck et al reviewed 847 full spine patient x-rays spanning from 1997 to 2001, concluding that 68.1% of the x-rays they reviewed revealed anomalies that may alter the application of SMT.60 Pryor and McCoy reviewed 500 patient files at a chiropractic teaching clinic, of whom 423 received x-rays of their spines. Pryor and McCoy found 91% of the cervical spine radiographs revealed pathologies, abnormalities, or anomalies that might alter patient management using manual therapy intervention.70 However, Pryor and McCoy also discuss the lack of evidence that some conditions they included in their study are true contraindications for cSMT. Ammendolia uses this lack of evidence to question if there is a need to alter patient management and sites a lack of improved patient outcomes as their main critiques of the use of x-rays to screen patients for contraindications to SMT.62 Jenkins et al found 30% of the cervical spine x-rays reviewed in their study revealed contraindications to cSMT.71 However, Jenkins et al questioned the validity of the posterior ponticle as a true contraindication to cSMT and stated that upon removal of this finding from their data, the prevalence of cervical spine contraindications dropped to 2.1%.71 To support the removal of posterior ponticles from their contraindications, Jenkins et al reference 2 chiropractic textbooks72,73 by Gatterman73 and Yochum and Rowe.72 Of interest, Jenkins et al do not reference the most recent edition of the Yochum and Rowe textbook from 2005, in which they stress that whilst vertebrobasilar insufficiency from a posterior ponticle is controversial, the importance of taking appropriate precautions and conducting a thorough examination when this finding is discovered on x-ray.72 Gatterman discusses the posterior ponticle as a relative contraindication, but state that extension and rotational manipulations should be avoided73
If the argument can be made that these findings do not alter treatment options due to insufficient evidence of compromised patient safety,62 then the literature must support this claim. However, the literature is controversial72; thus, there is insufficient evidence that they do not require alterations in treatment options from cSMT. If patient safety is the absolute objective, then these findings should be treated with caution a priori until evidence can be provided that cSMT is safe in the presence of such findings.
Oakley et al state that x-ray evaluation is the only way to assess cervical spine parameters associated with patient symptoms, “red flags” and both relative and absolute contraindications to cSMT.74 Alternatives including pre-manipulation tests have been found to lack sensitivity, specificity, and validity, thus are unhelpful to the clinician assessing a patient suspected as vulnerable to neurovascular compromise following cSMT.75,76 Also, pre-manipulation tests are supposed to assess for vertebral artery insufficiency75,76 Therefore, these tests are only useful when examining those patients at risk of the most severe adverse events and fail to provide anything meaningful when assessing those patients at risk of mild or moderate adverse events following cSMT.75
McAviney et al used lateral cervical spine x-rays to demonstrate a relationship between a loss of cervical lordosis and sagittal balance are associated with the development of neck pain.77 These authors found that a cervical lordosis <20˚ and cervical kyphosis are associated with the development of neck pain and cervicogenic symptoms, positing a normal range of lordosis between 31˚ and 40˚.78 These data are similar to previous literature that has shown hypolordosis of the cervical spinal is associated with neck pain.79 Kyphotic deformity of the cervical spine increases compressive loading of the vertebral bodies, and intervertebral discs, which accelerates degenerative changes, leading to discoligamentous injury and neck pain.57,80–82 Restoring the cervical spine to a lordotic configuration following surgical intervention is seen as an optimal outcome as it reduces the likelihood of adjacent segmental disease.83,84 Alteration of the instantaneous axis of rotation of the cervical vertebrae strongly correlates to neck pain indicating abnormal movement patterns of the cervical spine are common in neck pain patients.85,86 Capsular ligament laxity is a known sequela to abnormal movement patterns, leading to joint instability and neck pain.87
Loss of cervical lordosis has been shown to alter vertebral artery hemodynamics.88,89 Bulut et al matched 30 patients with confirmed loss of cervical lordosis to 30 controls with a normal cervical lordosis measured on lateral cervical spine x-rays. Doppler ultrasound evaluations of the participants’ vertebral arteries discovered a reduction in lumen diameter, flow volume, and peak systolic velocity of those with loss of cervical lordosis compared to those with normal cervical lordosis.88 Whilst the patients in this study were young (between 18 and 49 years) it has been shown that patients at risk of vertebral artery dissection are younger than those who suffer a thromboembolic stroke.9,90–92
Katz et al assessed the cervical lordosis of 7 participants (5 female, 2 male) between 28 and 58 years of age using lateral cervical spine x-rays. The geometric shape of the participants’ cervical spines ranged from 19˚ kyphotic to 20˚ lordotic. X-rays were repeated in the supine position with the addition of a spinal orthotic, which altered the participants’ cervical spines to lordosis ranging from 22.1˚ to 44.7˚. The participants then underwent a cerebral magnetic resonance angiogram (MRA) to evaluate the arterial blood flow of the circle of Willis and cerebral artery blood flow when lying in a neutral position. The MRA’s were then repeated with the addition of the same spinal orthotic as the repeated x-rays. Katz et al found improvement in blood flow ranging from 23% to 225.9%.89 Whilst the sample size of seven participants is poor, Katz et al demonstrated limited evidence that hypolordosis and kyphosis of the cervical spine result in vertebrobasilar insufficiency in some patients with neck pain. The findings from Katz et al echo previous findings from Olszewski et al who concluded that cervical spondylosis is associated with altered vertebrobasilar blood flow velocity leading to the development of vertigo.93
As a clinician who uses x-rays in chiropractic clinical practice, the data and findings discussed above lead me to ask the question; how frequently do lateral cervical spine x-rays alter treatment options in chiropractic practice?
METHOD
The method selected to conduct this study was a service evaluation using a retrospective review of patient records from a private chiropractic clinic in the South of England, UK. The records of all the patients who attended the clinic between the 1st March 2017 and 1st March 2021 were first identified. Ethics approval was granted by the ethics board of Sheffield Hallam University, and no ethical approval was required from the local National Health Service (NHS) due to the research method. The lists of x-ray justifications used are from the British Chiropractic Association (BCA) and the Practicing Chiropractors’ Committee on Radiology Protocols (PCCRP) For Biomechanical Assessment of Spinal Subluxation in Chiropractic Clinical Practice34,94 are shown in Tables 1 and 2. The PCCRP document is published in the US National Clearinghouse in July 2009 and is the accepted radiological guideline book of the International Chiropractor Association (ICA) The BCA justification lists the clinical findings that require x-ray evaluation of the patients presenting to British chiropractors. Patient records were then analysed to show who required x-ray examination of their cervical spine prior to commencing cSMT.
The data collected for the current study were obtained from patient records, therefore not all patients who attended the clinic required x-rays of their cervical spine. Patients were only x-rayed if they exhibited 3 or more of the justifications listed in Tables 1 and 2.
For the current study, the lateral cervical spine projections were reviewed. These projections alone were reviewed because:
-
It provides a strict data pool for analysis.
-
Lateral cervical spine projections are predominantly used for biomechanical analysis and segmental stability of the cervical spine thus is essential for some contraindications to cSMT.95–101
-
Flexion and extension evaluations of the cervical spine are performed in the sagittal plane to assess segmental motion and stability.95–101 Thus, these were included in the study.
All lateral cervical spine projections obtained between the 1st March 2017 to 1st March 2021 were reviewed providing 4 consecutive years of patient data. The PEO model of Patients, Exposure, and Outcomes is applied in this study as demonstrated in Table 3.
Inclusion criteria for the patient’s x-rays include all lateral cervical spine x-rays obtained in the clinic during the period stated that contain all relevant anatomy (C1 to C7) X-rays were excluded if the images were of poor quality due to motion artefact, inadequate exposure (too high or low) or if not all the relevant anatomy was visible. These criteria allow for maximum data collection and negate the possibility of any sexual, racial, or gender discrimination against any patients.
The study aims to identify the number of lateral cervical spine x-rays taken in a UK chiropractic clinic that directly influence the application of cSMT. This will include pathological/disease processes, segmental stability, segmental alignment, and biomechanical dysfunction as it impacts the integrity of the functional spinal units. White and Panjabi described a systematic approach to the biomechanical assessment of the cervical spine using x-rays (Table 4).102
Data collection
Firstly, the total number of new patients who attended the clinic between 1st March 2017 and 1st March 2021 was determined by searching the clinic’s electronic patient database, PracticeHub. These data were then divided into the year that the patients’ x-ray examination took place, providing a total of four years of consecutive data. These twelve-month intervals were determined to start from:
-
Year 1: 1st March 2017 until 28th February 2018
-
Year 2: 1st March 2018 until 28th February 2019
-
Year 3: 1st March 2019 until 29th February 2020
-
Year 4: 1st March 2020 until 28th February 2021
Next, a review of the clinics’ x-ray log was performed to find those patients who received x-ray evaluations of their cervical spine. Of these, only those patients whose x-rays had been electronically analysed using PostureRay® were included. PostureRay® software allows the operator to biomechanically assess the patients lateral cervical spine x-rays for relative rotation angles (RRA’s), absolute rotation angles (ARA’s), Cobb angles, Risser-Ferguson angles, sagittal balance, rotational angles of excursion, excursion distances, and the posterior tangent method.98,101,103–108 The DICOM x-ray images are imported into PostureRay® from the Carestream Vita Version 4 x-ray processing software. Biomechanical x-ray analysis using PostureRay® consists of mapping all four vertebral body corners of C2 through to C779 These biomechanical measurements, alongside findings of specific disease/pathological processes, degenerative changes, anomalies, and congenital normal variants listed as relative and absolute contraindications to cSMT were used to deicide is cSMT was appropriate in each patient’s case.
These lists of contraindications are included from Haynes-Mazion in Table 5, Jenkins, Zheng, and Bull in Table 6 and Puentedura et al Rushton et al and Scholten-Peeters et al in Table 78,13,15,29,61
The author is also the examining physician of all patients within the clinic.
-
All x-ray analysis was performed by the author, using the same computer system and software (PostureRay®)
-
All patient records were created by the author, thus accessing these data for analysis did not require any additional permissions from third parties.
All data pertaining to the patient’s identities were removed prior to analysis and for the write of up of this project. This included names, dates of birth, patient numbers, and any specific dates of when the examinations took place. Data collection included data found only within the patients’ x-ray reports, meaning that no data collected will be tracible to any individual patient should a breach in data security occur. All data were stored on a password-protected external hard drive, which was housed in a locked, fireproof safe, to which only the researcher had access within the clinic premises.
Data Analysis
The safety to proceed with cSMT was determined by the biomechanical measurements of ARA and RRA’s were all compared to the predetermined normal values found in the literature. Segmental stability/instability was determined by comparing each patient’s intersegmental values of RRA, ARA, sagittal balance, rotational angles of excursion and excursion distances and compared to normal values found in the literature.79,98,102–105
The RRA and ARA values, along with the conditions listed in Tables 5, 6, and 7 were used to determine if the application of cSMT was appropriate for each patient x-rayed. Jenkins et al define contraindications as “a problem identified before a procedure is applied that would make application of the treatment (SMT) inadvisable to that area because of its potential harm or delay appropriate treatment.”71 Jenkins et al define clinically significant findings as “something that involves a change to treatment approach for best treatment outcomes.”71
Results
A total of 626 new patients attended the clinic between 1st March 2017 and 1st March 2021. Of these, 319 (51%) were female and 307 (49%) were male. A total of 293 met the clinical justification criteria warranting x-ray examination of their cervical spine prior to commencing cSMT (46% of total new patients) Of these, 152 (52%) were female and 141 (48%) were male. These data show that of the 319 female new patients, 48% required x-ray examination, and 47% of the 307 male new patients required x-rays of their cervical spine. A breakdown of the number of new patients and the number of whom required x-ray examination per annum are displayed in Table 8.
The gender distribution across these years shows most new patients who attended the clinic were female (51%) However, this finding is not consistent across all years, as years one and three show most new patients were males (51% and 53% respectively) Of those who required x-rays, 52% of the total x-rays were female, however, years one and three show mostly males were x-rayed (60% and 52% respectively) This is logical as both years one and three had the greatest number of male patients. Table 9 demonstrates the full analysis of the patient gender profile of those who received x-rays.
Patient ages range from two to 90 years of age throughout the years included in this study (Table 10) The average age of patients was 43 years, and the median age across all four years data was 42 years with a standard deviation of 17 years.
Patients’ age demographics from those who required x-ray examination shows year 1 having the greatest median age of 44 years, whereas year 2 shows the greatest average age of 45 years. The data from year 2 also revealed the greatest age range of patients who required x-ray examination from five to 90 years of age. The total average age of those patients who required x-ray examination was 44 years, with a median age of 42 years and a standard deviation of 16 (Table 11)
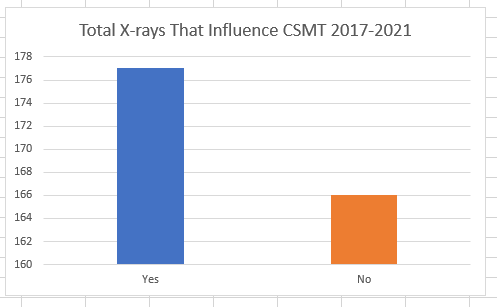
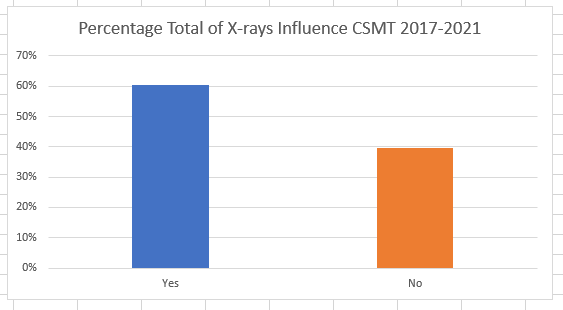
Of the 293 lateral cervical spine x-rays reviewed in this study, 177 (60%) altered the treatment options deeming cSMT inappropriate (Figures 1 and 2) This equates to 28% of all new patients who presented to the clinic subsequently had their treatment options altered as a direct result of contraindications found on x-ray (Tables 13 and 14) Zero x-ray images or reports were excluded from the study.


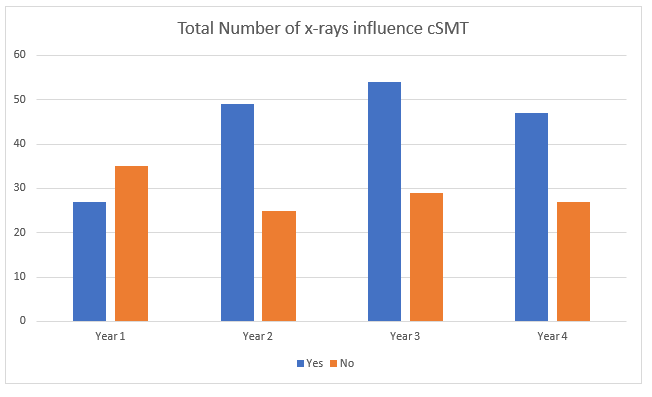
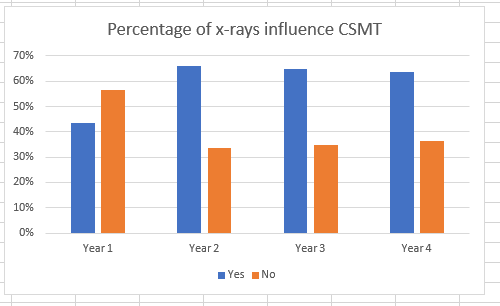
Per annum data shows that year one was the only year where most x-rays (56%) did not alter treatment options (Figure 3) There is no obvious explanation for this outlying data, as data surround patient demographics do now show any outlying factors for year one. However, clinical factors regarding the necessity for x-rays are a likely explanation and were not investigated by the current study.


The data gathered regarding the x-rays that revealed contraindications were analysed to assess how many x-rays revealed a single contraindication to cSMT and how many found >1 contraindication present in the same patient. Of the 177 x-rays that revealed contraindications, 95 (54%) contained a single contraindication to cSMT and 82 (46%) revealed >1 contraindication (Tables 12 and 13) On average of 15% of new patients had a single contraindication to cSMT, 14% showed multiple contraindications per annum. Finally, 32% of lateral cervical spine x-rays revealed a single contraindication to cSMT and 29% revealed multiple contraindications.
Data from year two shows the highest percentage of patients x-rayed (56%), however year two also received the larger population of older patients with the highest median age of patients (44 years) This is in comparison to the data from year four, which revealed 56% fewer x-rays (33% of total new patients) of patients but more than twice as many new patients attended the clinic in year four (223) than in year 1.95 One explanation of this high frequency of cervical spine x-rays in year one and such a low frequency in year 4 could be due to the median ages of the patients within these year groups. The patient median age in year 1 was the highest at 44.5 years (SD 16), whereas year 4 had the lower median age of 40 years (SD 16) of each patient this cannot be established is not the purpose of this study.
Further analysis of the data is required to gain more specific detail into how many of the findings occur in isolation or combination. Initial analysis of the x-ray findings showed multiple findings (e.g., cervical kyphosis and segmental instability) were found in the same patient however this data was not reported due to overlap of some findings. For example, advanced degenerative changes, adjacent segmental disease, and segmental instability are associated with one another and therefore frequently found simultaneously 57. As a result, attempting to differentiate between them provides no benefit, and combining them as a single finding renders each meaningless. Also, these findings contribute vastly more data points from the same patient group making it difficult to gleaming meaningful conclusions from so much data compared to so few patients. The decision was made to simply report the data as either a single contraindication or >one contraindication found simultaneously as this is relevant to clinicians and does not create more data points than necessary to answer the research question.
Discussion
The current study was designed to evaluate how frequently x-rays of the cervical spine altered the application of cSMT. It was hypothesised that using a deductive approach, it is possible to explore the research question of how frequently lateral cervical spine x-rays alter treatment options in chiropractic practice.
The current study revealed 46% of patients required x-rays evaluation of their cervical spine prior to commencing cSMT. Of which, 60% altered the application of cSMT as a direct result of their findings. This equated to approximately 30% of new patients presenting to the clinic required alterations in treatment options per annum. These data are comparable to other data published in the literature29,60,69,70 This study also found that 46% of these x-rays found more than one finding contraindicating cSMT present in the same patient.
Beck et al found 68.1% of the x-rays they reviewed revealed anomalies that alter the application of spinal manipulation. These authors also found that 11.6% of the reviewed x-rays were of asymptomatic patients, of which 69.4% showed an anomaly that altered the application of SMT. However, Beck et al (2004) did not limit their study to any one spinal region, reviewing full spine projections60 Jenkins et al (2010) found 30% of the cervical spine x-rays reviewed in their study revealed contraindications to cSMT.29
A total of 626 patients attended the clinic between March 2017 and March 2021. Of which, 293 received x-rays and were reviewed in the current study. Of the 293 patients who received x-rays, 152 (52%) were female, thus of the 319 female patients who attended the clinic during the four years data collected, 47% received x-rays of their cervical spine. This finding is comparable to the male patient population, where of the 307 male patients, 141 (47%) received x-rays of their cervical spine. The median age of the patients throughout the four years of data collection was 41.6 years, whilst the average of those who received x-rays of their cervical spine was slightly older with a median age of 42.5. These data are consistent with the findings of Beliveau et al from their scoping review of chiropractic patient profiles determined chiropractic patients are predominantly female (57%) with a median age of 43.4 years .3
Data in the literature report the most severe adverse events associated with cSMT occur in patients <45 years of age7,9,109–112 Rothwell et al stated that patients’ vertebral artery dissections were five times more likely to occur in patients <45 years of age.111 Others have reported risks of carotid or vertebral artery dissections are between three and twelve times more likely to occur in patients receiving cSMT in the <45 age bracket7,9,90–92,113 However, spontaneous vertebral or carotid artery dissections account for up to 25% of strokes in patients <45 years of age114–116 It, therefore, follows, that the data from these authors show that not only are the patients in this age category more likely to suffer spontaneous arterial dissections, but they are also statistically more likely to be seeking chiropractic care.3 The patient data in the current study revealed similar patient demographics regarding age and sex shown in the literature.3
Cassidy et al also found no increased risk of vertebral or carotid artery dissection from cSMT from their population-based case-control and case-crossover studies.9,113 This led the authors to conclude that the symptoms of headache and neck pain that prompted the patients to seek chiropractic care were likely caused by the vertebral or carotid artery dissection. However, Cassidy et al fail to rigorously define “chiropractic care” or “neck-related chiropractic care” in their studies, thus the relevance to their findings and the current study is questionable. Non-vascular complications from cSMT have been reported in the literature.117 Oppenheim et al discuss cases of pathologic fracture, cervical disc herniation, myelopathy, and radiculopathy following cSMT. Oppenheim et al describe complications of cSMT as “under-recognised” and “likely grossly under-reported” calling for pre-manipulation diagnostic imaging to identify those at risk of such complications.118 One criticism of Oppenheim is from Haldeman who pointed out that Oppenheim et al (2005) report 18 cases of various complications spanning six years, thus the incidence of these complications are exceedingly rare, a rate of which would be the envy of any other treatment interventions.118 Notwithstanding, if complications from cSMT are indeed under-reported as Oppenheim et al state, then the criticism from Haldeman is moot, as the actual number is unknown. Also, without additional evidence to support the gross under-reporting claim made by Oppenheim et al is conjecture.
Dvorak report a frequency of transient complications following cSMT using high-velocity/low amplitude thrust techniques of 1:16,716.119 Other authors have stated risks of serious adverse events following cSMT vary between 1 in 50,000 to <1 in 5,000,000.120–123 However, there is a great difference between safety risks following cSMT and the appropriateness of cSMT to a given patient. The current paper was not designed to explore adverse events following cSMT but rather to assess the frequency at which x-rays influence the application of cSMT.
Benign adverse events from SMT have been reported to occur in 23-83% of patients.7,17,22,23,28,124–127 Rubinstein et al reported 56% of chiropractic patients reported experiencing adverse events following SMT, 13% of which were reported as severe.126 Rajendran et al reported the highest incidence of adverse events following SMT (83%), 74% of which were increased pain, and 58% experienced stiffness.125 Neither Rubinstein et al nor Rajendran et al included any form of diagnostic imaging findings to aid in exploring predictors of adverse events following cSMT nor did they report if the patients who experienced adverse events were assessed for the appropriateness of cSMT.
Hurwitz et al reported from their randomised clinical trial that adverse events from cSMT occur in 30% of patients.128 These authors, therefore, recommend altering treatment interventions from manipulation to mobilisation, especially to those with severe neck pain.128 The current study found 32% of patient x-rays revealed at least one contraindication to cSMT, altering treatment options to alternatives, such as mobilisation.
It is our opinion that x-rays are necessary to determine the appropriateness of cSMT and accurately select those patients who are more likely to benefit from cSMT and reduce the risk of adverse events.
Study Limitations
The current study suffers from several limitations including only analysing lateral cervical spine radiographs whilst excluding other cervical spine projections. Any contraindications visible on anterior-posterior projections, such as advanced atherosclerosis of the carotid arteries may have been missed in the data collection.
Limitations with the study design and method mean the study results are not generalisable or meaningful to all professionals who use cSMT. As a service evaluation, the results cannot be generalisable across all UK chiropractic clinics, therefore the meaning of these results to the profession at large is low. As stated in the method section, not all chiropractors use cSMT in their practice, which further diminishes the findings of the current study are only relevant to those who practice cSMT as defined in the method section.
As the researcher, examining clinician and author of this study are one and the same, the issue of bias towards the findings of this study must be acknowledged. The issue of bias using a retrospective review of records was discussed in the method section. The researcher tackled the research question from a manual therapist’s perspective, using a post-positivists approach. Therefore, the introduction of bias cannot be avoided as a clinician who uses x-rays with their clinical practice, objectivity is in question. The inclusion of collaborators for this study may have reduced the risk of bias but was not possible for this MSc thesis.
Notwithstanding, however, the researcher simply applies the findings of other researchers discussed in this study. The practical application of x-rays prior to commencing cSMT provides the researcher with the experience of these data in the real world of clinical practice. The researcher then approached the research question using a deductive methodology from scenarios with patients who experienced adverse events following cSMT only to subsequently discover contraindications on x-ray when re-examining the patient. This can be viewed as either bias towards the study from personal experiences, or providing the researcher with hands-on, clinical experience of both adverse events and utilising x-rays in practice on patients with neck pain. Since ideas are generated from our sense experiences129 it is reasonable for a clinician to tackle the research question.
The inclusion of posterior ponticles as a contraindication to cSMT may bias the results. The lack of knowledge and investigations into mild and moderate adverse events in those patients with a posterior ponticle makes it challenging to include or exclude them as a true relative or absolute contraindication.
Clinical factors surround the necessity for x-rays were not investigated by the current study. For example, the clinical justifications from Tables 1 and 2 most frequently used were not collected for this study. This was not the purpose of the study, thus outside its scope. However, these data may help with data analysis regarding why some years show significantly more patients were x-rayed than others. Due to the unpredictability of clinical practice, the types of patients who may present to the clinic and why will influence the necessity for x-ray examination.
CONCLUSION
The current study found 60% of lateral cervical spine x-rays obtained in a UK chiropractic clinic alter the treatment options for patients. To the authors’ knowledge, this is the first study that analysed the findings of lateral cervical spine projections only to assess for alterations in treatment options. Whilst Jenkins et al (2010) included all spinal regions in their data analysis, the results from the cervical spine data were similar to the current study findings.71
Future studies into adverse events following cSMT may benefit from including data from pre- and/or post-manipulation x-ray findings of those patients who suffer even benign adverse events. Much of the literature exploring adverse events following cSMT focuses on severe and therefore rare adverse events whereas the more commonly experienced mild and moderate adverse events are largely ignored. Quantifying rare events is challenging by the nature of rare events, so focussing attention on more commonly seen mild and moderate adverse events may yield more applicable data on contraindications to cSMT.7
Whilst it is important to identify those at the greatest risk of severe adverse events, the ability to identify those patients for whom cSMT is not appropriate and those who are more likely to experience mild and moderate adverse events should be investigated. This study has shown that pre-treatment x-rays frequently alter the treatment options in chiropractic clinical practice. However, due to the nature of clinical practice, in the current study, not all patients presenting with neck pain received x-rays of their cervical spines.
Ultimately, the debate surrounding the appropriateness of x-rays in chiropractic clinical practice should be based within the patients’ values and preferences regarding that person’s healthcare.130 Clinicians and academics on either side of this debate are simply trying to reduce unnecessary risks to the patient. The current study adds evidence that x-rays frequently alter treatment options for patients seeking chiropractic treatment in the UK. The current study also adds evidence that x-rays are a valuable tool for identifying appropriate treatment interventions for patients with neck pain and reduce the risk of adverse events in chiropractic clinical practice by removing cSMT as a treatment option for those patients.