INTRODUCTION
The chiropractic profession faces an ongoing challenge to establish credibility, including for the management of spinal disorders that constitute the core of its current healthcare market share.1,2 In a rapidly-evolving healthcare environment, where the recognition that being evidence-based is a requirement for clinical practice,3 the ability and proclivity of the profession to conduct and translate research into practice is assuming greater importance. Thus prioritizing, strategizing, funding, conducting, implementing, and translating evidence resulting from high-quality research must happen faster for chiropractic than the historical 17-year pipeline to convert 14% of medical research into clinical practice.4,5 It is critical to investigate whether chiropractors’ attitudes, perceptions, personal paradigms, and beliefs affect engagement with research and thus translation of evidence into clinical practice. It is also important to describe past research and publication activity, capacity, barriers, collaboration and funding access to organize research and bolster output.
Beliefs and Perspectives
The chiropractic profession has a colorful if a chequered history of opinions, beliefs, and ideologies that have shaped practice, some being metaphysical and others being mechanistic. It is reasonable that these beliefs and ideologies may influence ideas around research, research activity, and participation. The Australian Health Practitioner Regulation Agency (Ahpra) code of practice indicates that a practitioner may have their own personal views and opinions as long as they do not contradict public health policy and fundamental professional values.3 However, a number of ideological and behavioral patterns within the profession may need reconciliation and alignment with regulatory codes of practice to identify research priorities and strategies. Part of this reconciliation process is to explore current attitudes, ideas, and activities in research across the chiropractic profession and identify overlapping research priorities.
Terminology in the chiropractic profession-specific lexicon has often engendered heated debate. This is nowhere better illustrated than around the term ‘vertebral subluxation.’ There are prolifically published proponents such as Holt and Haavik,6 while many other academics and educators7,8 vocally reject such terminology as being simply historical, an artifact that creates a barrier to professional advancement.9 The relevance of terminology and personal paradigms is that they likely influence the propensity of practitioners and academics to engage with research and research priorities. Exploring the impact of terminology on research and research participation remains important reconciliation and compromise on specific terminology being the goal of future research strategies within the chiropractic profession.
Publication Activity and Barriers
Chiropractors are similar to other health professionals in terms of their favorable attitudes towards evidence-based practice (EBP), whilst expressing limitations and barriers related to EBP skills, research relevance, and lack of time.10–14 Improvements in both research productivity and participation may be attained through collaborative, consensus-led research strategies, thereby also bolstering confidence and skills in doing research. Bakkum and Chapman15 for example, found among chiropractors the most frequently cited barriers to publishing were pursuit of publishing as a low priority followed by a lack of time to prepare a manuscript.15 Our study explored research priorities and participation, which in turn, may inform research priorities and stakeholders, alongside the most valuable topics needing investigation.
Barriers to publication in the chiropractic community are closely related to the concept of knowledge transfer (KT).16,17 This is a term that is often used interchangeably with phrases such as knowledge transfer, translational research, knowledge mobilization, and knowledge exchange.16–18 Knowledge translation, also known as the science of implementation, is increasingly recognized as a critical element in improving healthcare delivery and aligning the use of research knowledge with clinical practice.16,17,19
A systematic approach may assist in identifying barriers to publication to help understand why a specific gap persists between what is known to be effective, what is done and how this gap might be reduced.17 Kawchuk et al17 listed multiple strategies for KT in chiropractic which may have application in facilitating research output among both academics and practitioners. Several studies have previously itemized the primary barriers to implementing evidence in clinical practice. These include a lack of time and the lack of skills to navigate and appraise literature. While these are two important barriers, over 250 other barriers have been identified with respect to medical physicians.20 Quite often, these barriers are easy to appreciate if they are grouped into those affected by individuals and those external.21
Funding
There are currently several key stakeholders who fund research in the Australian chiropractic landscape who have also published research agendas, strategies or priorities upon which we previously reported.22 Internal professional funding initiatives in Australia have included establishing the world’s largest voluntary practice-based chiropractic research network, the Australian Chiropractic Research Network (ACORN)23,24; assisting the establishment of the Chiropractic Academy of Research Leadership (CARL) program,25–28 scholarships for higher degree research (HDR) candidates,29,30 and for individual research projects.31 More generic financial assistance toward university-based chiropractic programmes, national research conferences and symposia has also been forthcoming.32–35 It is difficult however to measure individual or institutional funding secured in the absence of any aggregated publicly available sources or internal university balance sheets due to ‘commercial in confidence’ restrictions.
Historically, there has been relatively few instances of funding sourced from outside the profession for research in chiropractic topics in Australia, especially external, category 1-3 Higher Education Research Data Collection (HERDC) - funding. Consequently, Australian chiropractic professional membership organizations have unilaterally undertaken various initiatives to support healthcare research and build research capacity totalling approximately AUD$3.4 million in the last decade.36 As reported previously, this sum is very low when compared for example, to private pharamaceutical research36,37 or physiotherapy.38 This is all the more reason to develop research strategies that are inclusive, promote practitioner participation and facilitate implementation of consensus-led research areas.
Encouragingly, in June 2021 the Australian Federal Minister for Health and Aging, Greg Hunt MP39 announced a funding collaboration. The first of its kind, it included funding by the Australian Medical Research Future Fund (MRFF),40 Macquarie University,41 the ACA and the Australian Physiotherapy Association (APA) of a AUD$2.1 million study to investigate whether patients with low back pain would benefit from team-based care by integrating physiotherapists or chiropractors into GP clinics.
Aims and Objectives
While the primary aim of our study was to identify and compare the research priorities of Australian practicing chiropractors and academics across listed research domains, and to seek their views on existing chiropractic research strategies (already published),22 parallel objectives were to gain insight into the perspectives toward research, current capacity for research output and funding secured by academics and researchers. This paper reports on the latter group of items that is, research perspectives, publication output, barriers and funding secured in the previous 5 years.
METHODS
Study Design, Setting and Participants
Details of the methods and strategies employed to recruit study participants and development of the online survey used for this study have been published elsewhere.36 Briefly, Australian chiropractic academics (n=220) and practicing chiropractors (n=1680) were invited to participate in an online survey via an email containing a link. Practicing chiropractors were invited to participate via a link to the online survey questionnaire distributed to members of the Australian Chiropractic Research Network (ACORN) - a national practice-based research network housing a nationally representative sample of Australian chiropractors.1,2 The survey was conducted between the 19th of February and the 24th of May, 2019 using the Survey Monkey platform.42 Two further follow-up invitations were also sent at 4-week intervals as per standard online survey protocols.43 The study was approved by the Human Research Ethics Committee of the University of South Australia (UniSA Ethics Protocol #0000035553) and all methods were performed in accordance with the relevant guidelines and regulations.
Survey Instrument, Variables and Measurements
The questionnaire introduction explained the approximate duration, purpose and contents of the study, that survey completion was voluntary, and that participant information was anonymous. Consent was implied by completing the survey. Participants were asked to provide applicable demographic information such as age, gender, years in practice and/or academia, academic qualifications, and practice location. In most sections of the survey participants were invited to make suggestions or comments in the open text boxes provided within the survey instrument.
The various categories of questions are presented below;
Statistical Analysis
Responses were entered directly into the online survey by participants. On completion of the collection phase, data were exported from the SurveyMonkey platform into SPSS (V.24) for cleaning and statistical analysis. Required responses in most of the priorities section ensured minimal missing data and multiple responses from single participants were managed using the de-duplication procedure for online surveys as described by Konstan et al.44 Categorical data were descriptively analysed using frequency distributions and percentages, and continuous data analyzed using the median and interquartile range (as data were not normally distributed). Differences between groups (i.e., academics vs. practitioners) in Likert scale responses (e.g., perceived research funding and resource allocation priorities) were assessed using independent samples Mann-Whitney U Test. Comparisons were tabulated of research priorities based upon responsibility to fund research, perspectives on published research, output volume and type by author, time spent in research, barriers to research, collaboration and funding secured. Differences in means for the rating scales were presented in Bland-Altman scatter plots.
RESULTS
Demographic Data
Demographics of the participants have been previously reported thus will not be replicated here.22
Responsibility to fund research
Academics and practitioners agreed that it was the responsibility of professional organizations and CARF (p=0.47, 0.56), universities with chiropractic programs (p=0.06) and field practitioners (p=0.64) to fund research. Practitioners and academics disagreed significantly (p=0.02) that it was the responsibility of the ASRF to fund research and further, 21.2% of academics compared with 5.9% of practitioners rated it as ‘very unimportant’ that it was the responsibility of the ASRF to fund research. However, most of both academics and practitioners somewhat or strongly agreed that professional associations (87.9%, 84.7%, respectively), the ASRF (72.7%, 87.3%), CARF (90.9%, 86.3%) and universities with chiropractic programs (87.9%, 95.3%) had a responsibility to fund research on chiropractic topics (Table 1). To a much lesser extent, over half of academics (57.6%) and practitioners (55.3%) agreed (somewhat or strongly) that funding to support chiropractic research was a responsibility of field practitioners.
Perspectives on published research
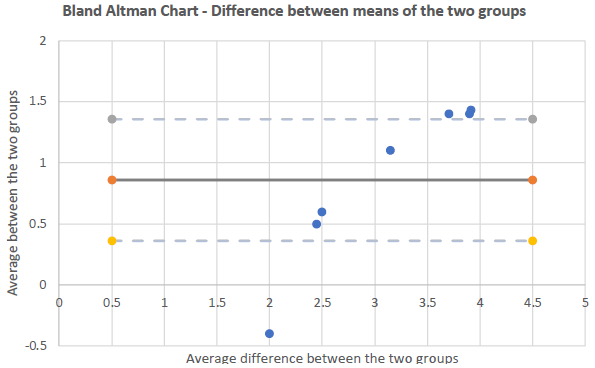
Practitioners were significantly more likely than academics to agree with the statements (Table 2); “I am more likely to engage with research… published in chiropractic focused journals” (p=<0.001); “that uses traditional chiropractic terminology such as subluxation” (p=<0.001), “performed by chiropractors” (p=0.02), “focused on traditional Chiropractic Philosophy” (p=<0.001), “focused on the detection/correction of vertebral subluxations” (p=<0.001), “focused on Chiropractic as independent of multi-disciplinary, mainstream health care” (p=<0.001). Academics were also significantly (p=0.04) more likely than practitioners to agree with the statement; “I am more likely to engage with research focused on musculoskeletal conditions”.

The Bland-Altman chart shows that three items lie within the 95% confidence interval upper and lower limits (dashed lines) – “by chiropractors,” “chiropractic journals,” and “chiropractic as independent,” respectively - suggesting agreement (average is the solid line) on these three items between the 2 groups (academic and practitioner). There appears to be disagreement between the 2 groups for the 4 items of “MSK focused,” “Detection/correction of subluxations,” “traditional chiropractic terminology,” and “Traditional chiropractic philosophy,” although borderline.
Publication Output (Tables 3-5)
Of academics, 39.4% reported publishing between 1-5 papers (av <1 per year) in the preceding 5 years while 24.2% reported not publishing any papers. There were 2 academics who reported publishing over 20 papers while there were 3 practitioners who reported publishing 20 or more papers in the same time frame and just under 9% of field practitioners reported they had published a scientific paper in the last 5 years. Approximately one-third (30.3%) of academics had not made a presentation at a scientific conference, while 75.8% reported not publishing a book chapter in the last 5 years. There were 2 field practitioners who reported publishing >20 book chapters in the last 5 years.
For academics, in descending order the most frequent types of publications (>=5) were; experimental studies in clinical science (n=8), experimental studies in education & workforce (n=7), systematic, integrative or narrative reviews / meta-analyses in clinical science (n=7), commentary/opinion articles in education & workforce (n=6), observational studies in clinical science (n=6), observational studies in education & workforce (n=6), qualitative studies in education & workforce (n=6), mixed or multi-methods in clinical science (n=6) and commentary/opinion articles in clinical science (n=5).
For practitioners in descending order the most frequent types of publications (>=5) were case studies/case series in clinical science (n=18), observational studies in clinical science (n=10), systematic, integrative or narrative reviews/meta-analyses in clinical science (n=9), commentary/opinion articles in clinical science (n=8), experimental studies in clinical science (n=7), commentary/opinion articles in education & workforce (n=6), commentary/opinion articles in public health (n=6), commentary/opinion articles in generic topics (n=6), systematic, integrative or narrative reviews / meta-analyses in basic science (n=6) and experimental studies in basic science (n=5).
Academics reported on average spending 24.9% of their time on research while practitioners reported 6.9%. Of academics reporting no publications in the last 5 years, 6 (18.2% excluding PG-HDR students) reported spending on average 15.3% of their time currently engaged in research. Both groups reported a desire to spend significantly more time on research (academics 1.7, practitioners 2.9 times). Time (academics 59.4%, practitioners 61.6%) and financial support (academics 40.6%, 34.8% practitioners) were reported as the greatest barriers to research activity. Practitioners reported knowledge and skills (33%) and institutional support (20.7%) as barriers while 15.7% listed lack of interest as a barrier. Collaboration was common among academics both with other institutions (66.7%) and with researchers from other professions (78.8%).
Funding Secured in the Preceding 5 Years (Table 6)
The majority (78.8%) of academics reported not having secured any funding for research with 3 academics reporting having secured Category 1 funding in the preceding 5 years. The two most reported sources of funding secured (54.5%) were university funding and category 3 (39.4%). Of academics, 27.3% reported self-funding their own research.
DISCUSSION
Responsibility to Fund Research
This is the first study to capture data from both academics and field practitioners in this space. Both groups agreed that professional associations, the Australian Spinal Research Foundation (ASRF), Chiropractic Australia Research Foundation (CARF) and universities with chiropractic programs all had a responsibility to allocate funding and resources to support chiropractic research. While 72.7% of academics agreed it was the responsibility of the ASRF to fund research, this is countered, paradoxically, by our previous finding that 70% of academics strongly reject the research strategies and priorities of the ASRF.22 Only 20% of academics thought it unimportant that ASRF fund research; thus, it is unclear what these findings indicate beyond academics as a group being strongly opposed to the ASRF research activities and agenda. This result where ASRF research is opposed or rejected, appears based on perceptions and assumptions around the nature of the research rather than the funding itself. If a compromise and consensus research agenda were achieved, then ASRF funding may become acceptable since over the 45 years of its existence, the organization has funded over 250 projects in excess of AUD$2.8 million.45 Academics seeking scarce funds may consider the benefits of collegiality to access this resource. Both groups agreed the Australian Spinal Research Foundation (ASRF) and Chiropractic Australia Research Foundation (CARF) have a responsibility to allocate funding and resources to support research. This would be expected since this is the charter of these varous organizations. Naturally, individual organizations identify and allocate research funding based on their own discretion, but results of this study suggest that chiropractic research organizations could at least interact and cooperate to identify and develop a common research agenda to facilitate research in topics of value and meaning to the chiropractic professional within the context of the broader public health landscape. Such a research agenda would include research related to the primary health sector, in which chiropractic is embedded. A common reseach agenda would, thus, depend on the appetite for cooperation.
The difficulty in formulating a truly collegial approach to support of research in the Australian Chiropractic profession relates to partly to quantifying funding and projects. Despite laying claim to be the “peak body for evidence-based Chiropractic” in Australia, CA/CARF appear to be the least transparent with respect to publication of recipients of research funds.46 Thus, it is not possible to compile a register of all projects funded in Australia by the 3 main stakeholders, since CA/CARF do not publish an itemized list of funded projects.
Both groups felt to a much lesser extent that providing funding and resources to support chiropractic research was a responsibility of field practitioners. Given the funding for all the organizations listed (excepting universities) has been primarily from the Australian chiropractic practitioner community through membership fees, this may not be surprising. Over 95% of practitioners and just under 88% of academics felt universities with chiropractic programmes had a responsibility to fund research; thus, it is somewhat dissonant to observe the current funding model of Australian chiropractic research in universities is one that involves substantial funding indirectly from field practitioners via their peak professional organization, the ACA.22,35 This occurs despite the unrevealed but seeming profitability of chiropractic programs to their hosting institutions where it appears a relatively small proportion of revenue is directed back to ‘chiropractic’ research. Another concerning, paradoxical finding was the relatively high proportion (27.3%) of academics who claimed to self-fund their own research. Just how this self-funding occurs is unclear. Anecdotally it is possible academics may be expected to carry out research in their own time due to the tighter fiscal landscape of Australian academia over recent times.47
Perspectives on Research
Personal paradigms affect clinical practice and attitudes to research regardless of where one is positioned on the ‘philosophical’ or ideological continuum whether they be practitioner, academic or researcher. The simplistic division of the profession into two discrete ‘camps’ based on a historical schism,48 often reflects authorship bias and ignores the full range of professional perspectives and risks descending into scientific imperialism49 and what Sackett described as ‘the tyrannizing’ of evidence-based practice.50 Our data confirm nomenclature and terminology are still flashpoints within the profession engendering passionate debate and posturing from each end of the continuum. Despite being listed in the ICD-11 (M99.10) and definition within WHO publications, the use of ‘vertebral subluxation complex’ or ‘subluxation’ remains controversial within the profession. All stakeholders may consider the desirability of a more pragmatic, collegial approach to professional dissonance. For example, if one were to replace the controversial ‘subluxation’ with the generic term ‘spinal disorders’ or “dysfunction of the functional spinal unit* (FSU)”,51,52 there would appear to be little disagreement between academics and practitioners regarding perspective on the ASRF research agenda. The ASRF research agenda items cover basic science, clinical practice, public health and epidemiology. When substituting the term ‘spinal disorders’ for ‘subluxation’, the items would correlate with the research priorities of academics as evidenced in our previous report.22,53,54
The Bland-Altman chart shows that there seems to be disagreement between the 2 groups for the 4 items of “MSK focused,” “Detection/correction of subluxations,” “traditional chiropractic terminology,” and “Traditional chiropractic philosophy”. However, it appears very borderline disagreement for the three items of “Detection/correction of subluxations”, “traditional chiropractic terminology,” and “Traditional chiropractic philosophy.” In practice, this implies there is scope for negotiation and compromise on these 3 items, toward agreement, between the two groups.
Publication Output and Type by Author, Time Spent in Research, Barriers to Research, Collaboration
The average publication rate per year for Australian chiropractic academics in the PubMed database has previously been found to be very low when compared to other health disciplines.55,56 No studies to our knowledge have previously recorded publication data for field practitioners in Australia. Thus, the assumption is that research output across the entire chiropractic profession is also low. This is the first time to our knowledge the publication output and capacity, indeed the interest and desire to participate in research among Australian field practitioners has been investigated. Unfortunately among academics, there has been little improvement since 2013 when the average yearly publication rate for academics was reported as 0.62, which is very low when compared to other professions.55 We found 39.4% of academics, reported publishing between 1-5 papers (av <1 per year) in the preceding 5 years, while 27.3% reported not publishing anything in that time. The universities with chiropractic programs may need to undertake a pragmatic review of time and resource allocation to facilitate greater quality publication output in future.
An anomalous incidental finding was that of academics reporting no publications in the last 5 years, 18% (n=6, excluding PG-HDR students) reported spending on average 15% of their time currently engaged in research. Since Australian academic salaries range between AUD$80,000 (level A)-$215,000 (level E), translated into financial terms, this non-productive time may cumulatively represent around AUD$100,000 annually.57 This raises serious questions over scarce resource allocation. It still appears as though there are a small number of high performers in terms of publication output among academics. Interestingly there were several field practitioners who reported publishing 20 or more papers in the same time frame, and just under 9% of field practitioners reported they had published a scientific paper. This would appear to be a potential resource that could be accessed to facilitate increased future output, possibly in collaboration with unpublished and underperforming academics.
In defense of chiropractic academics and their institutions, their primary mandate is not to undertake or lead high-level research or compete for research funding, but rather to deliver sound quality teaching, learning and supervision in undergraduate chiropractic programmes. Furthermore, in times of global financial crises and pandemics, the viability of many university-based courses has been challenged, where the quality of taught courses and student numbers are a higher priority over research. Hence, it is probably unreasonable to expect chiropractic academics and their respective institutions to fully-fund, lead and undertake research, when this is not their ‘core business’. In fact, the results offered in this paper broadly support the notion that chiropractic institutions focus on producing competent, safe practitioners by offering quality taught undergraduate courses rather than research.
Allocation of ‘research time’ is intrinsic to publication output. The research performance of individual academics is based on their ‘research output’, in the form of publications, grants or supervision of research students, but historically, little attention has been paid to the ‘input’ or the time required to achieve these outputs. Evidence shows academic staff strongly support a transparent and holistic approach to workload planning which acknowledges the full range of activities they undertake.58 Bowen et al59 stress developing strong collaborative partnerships between health service researchers and the end users of the research to ensure impact. They call for a ‘re-imagining’ of methodologies and identify a need to develop capacity in the applied research and an equipped health workforce.59,60 Mixing experience with naivety offers the possibility for wide ranging discussion and development of innovative initiatives.61
It is possible that increasing research output can be achieved by various mechanisms such as the development of research centers and research training; strategically using doctoral student research; facilitating staff research through teaching release and other programs; encouraging collaborative programs with partner universities; increasing staff with doctoral qualifications; dealing with high student numbers; and devising marketing strategies to advertise research strengths.62 These are all mechanisms that are open to the chiropractic profession, and some have been used to date; however it seems from our data, little progress has been made over the last decade in terms of ‘per capita’ publication output.
To explore solutions to the issues of lack of research in the chiropractic landscape, it is key initially to determine the appetite for doing and participating in research across the various chiropractic stakeholders and interest groups in Australia – this would identify interested, capable and cooperative engagement and participants. With these groups in mind, then identify novel or innovative ways to fund and support research e.g., practitioner donations and institutional grants, possibly creating brand new research entities that have the capacity and resources to conduct/implement research. Relying on university-based chiropractic programs or institutions where research is not the mandate or priority, particularly where there is limited capacity, is seemingly unrealistic. In addition, engage with existing organizations that conduct chiropractic-related research with a view to finding ways to implement research with less bureaucracy and confounding interests. Finally, identify ways and organizational capacity, through associations, colleges and groups, to translate research into practice and lobby healthcare funders.
The research agenda and topic for study/testing should focus and cover the ‘common ground’ between stakeholder groups, institutions and organisations, while these agreed agenda research items should align and reflect broader health care priorities, such as in primary care, in which chiropractic is embedded. Prior to choosing the research agenda, those research topics with the highest probable impact and usefulness/relevance to practice, should be prioritized, with a view to improve on care services, access to services/delivery and facilitate professional interests.
Funding Secured
We previously observed that like researchers, practicing chiropractors also have a vested interest in the value of practice-relevant, high-quality research being conducted, both for their patient care and for the wider profession. Practitioners not only help fund research but need to have confidence that research findings are both applicable and definitive when informing clinical practice.22 Since many academics have not published anything, the finding that the majority (78.8%), also reported having not secured any funding for research in the preceding 5 years, is consistent. There were only 3 academics who reported securing Category 1 funding in the preceding 5 years. The 2 most commonly reported sources of funding secured (54.5%) were university funding and category 3 (39.4%). Notably, 27.3% of academics reported self-funding their own research. The nature of this self-funding was not specified but could conceivably include ‘free time’ spent in research. Universities may expect some academics to have research as a ‘hobby’. The higher level of Cat 3 funding (Industry and other research income e.g., contracts, grants, donations, bequests and foundations) compared to Cat 1 (Australian competitive grants e.g., NHMRC, ARC), illustrates that the profession is dependent on internal resources for the majority of research funding.
Comparison to Other Health and Medical Research in Australia
We refer to data provided by the Australian Institute of Health & Welfare63 and an eloquent summary of the history of health and medical research in Australia.64 After a restricted early focus of research prior to the 1940’s, Australian health and medical research has broadened and now includes basic biomedical science, clinical medicine and science, public health and health services. This is evidenced by the Australian Government’s (Federal) expenditure on health and medical research 2017-2018 being approximately AU$ 4.4 billion, of which AU$862 million was via the National Health and Medical Research Council (NHMRC). For 2017-2018 there was AU$404 million of non-government (private) funding, while State (non-Federal) funding was around AU$827 million, giving a grand total of around AU$5.75 billion. In 2018–19, $206 million was funded through the Medical Research Future Fund, providing grants of financial assistance to support health and medical research and innovation. The establishment of the NHMRC in 1936 formalized government funding with the role of the NHMRC expanding to support discovery research and also to work to achieve the benefits of research for the community.
Community support and recognition of health and medical research has been high in recent decades and Australian health and medical research rates highly against international benchmarks. To maintain the momentum of high-quality, relevant research, countries with a developed health system need an active, involved health and medical research effort.
Independent medical research institutes (private, non-government, and/or university-based) have long been a distinctive feature of Australian health and medical research and remain an important component to research conduct and activity, particularly in the development and testing of novel or existing treatments/ interventions.
By extrapolation, the key features of organized health and medical funding that may be translated to chiropractic-related research are:
-
The need for persistent and dedicated research efforts, despite potential barriers or setbacks
-
Good leadership, which is essential for the conduct of relevant, high-quality research
-
Research should test and discover, but also be meaningful to the community
-
Research funding should ideally come from both government and non-government (private) sources, engaging with both government and private research organisations
-
Research needs to be of high standard (quality, integrity, ethics), preferably of international standing.
-
Research warrants community support and recognition, including respect for research with the applicable industry
Limitations
There are several important limitations and caveats on our data. Participants self-reported only quantity and type of output (there was no measure of the quality of journal published in or other metrics such as impact factor or citations). Limitation of our own resources meant there was no triangulation of actual publication data for either group to verify output to compare with self-reported data. Finally, research output was measured in strata rather than exact numbers resulting in best estimates.
We would add that we did not collect data either on the quality of journals or citation metrics from either group which would be important for future studies. The debate of quality vs quantity is for future investigation. We received over 600 qualitative responses in the open text sections for future research the findings of which will be published in the future.
Summary of Insights
-
We present here a fascinating set of outcomes suggesting mixed views and opinions on research, but that there are research priorities in common between the practicing chiropractors and chiropractic academics.
-
There are recognised chiropractic organizations that fund research, but cooperation and consensus between these organizations regarding research strategy is lacking.
-
Communication and cooperation between funding organization should be encouraged and facilitated with a view to promote and enable meaningful research.
-
The overlap in research priorities encountered within the chiropractic profession, considering all stakeholders, should be identified and ear-marked for implementation within the context of the primary care setting of chiropractic profession.
-
Those academics who are employed in a purely educational role could be encouraged to transition to the production of research by collaborating with field practitioners.
-
Engagement and capacity building is possible for the large pool of practitioners who have indicated an interest in research to take up ‘research as a hobby’. Participation could improve overall capacity and open pathways other than clinical practice for the ‘clinician researcher’.
CONCLUSION
This study suggests that research activity and output across the Australian chiropractic profession is still modest and of variable utility, particularly related to contemporary evidence-based clinical practice. There remains a disconnect between time/effort allocated to research and volume of publications. There are a small number of organizations that support and fund chiropractic research, but their efforts appear fragmented and divided, lacking collegiality. There is clearly scope for cooperation between chiropractic research funding organizations and optimization of research activity to generate and implement a consensus research agenda. Any agenda should be duty-bound to align with needs and evolution of the chiropractic profession within a modern healthcare landscape. This study offers recommendations on facilitation and improvement on a consensus Australian research agenda.
Contributions
Concept development; BLW, LA-W: Supervision; LA-W, JA: Literature search; LA-W, BLW: Design; LA-W, BLW: Statistics: LA-W, GP-S, Writing; LA-W, BLW, JA, GP-S: Critical review of revised manuscript for intellectual content prior to submission; LA-W, BLW, JA, GP-S
Funding statement
The Australian Chiropractors Association (ACA) formerly known as the Chiropractors’ Association of Australia (CAA) initially funded the ACORN project. However, the funding source of the ACORN project had no influence on any aspect of the study. The research reported in this study is the sole responsibility of the authors and reflects the independent ideas of the authors alone.
Competing interests
LA-W was a committee member of the ACORN-PBRN, GP-S and BLW have no conflicts to declare. JA was the Principal Investigator of the ACORN-PBRN.
Patient consent
Not required.
Ethics approval
The study was approved by the Human Research Ethics Committee of the University of South Australia (UniSA Ethics Protocol #0000035553). Participants were informed about the study via the survey cover sheet. Informed consent was provided through entering the portal and completion of the survey.
Data availability
The dataset of this study is available by permission of the lead author at Harvard University Dataverse.65