
Introduction
There is currently interest in understanding the biomechanical alignment of the cervical spine and related radiographic metrics in order to better treat cervical spine deformities.1–5 Whether by surgical or non-surgical approaches, the structural goal is to realign the cervical spine to achieve successful outcomes.
Non-surgical cervical lordosis correction has support in the literature.6–9 Cervical extension traction methods as developed and used within the Chiropractic BioPhysics® (CBP®) multimodal treatment regimen show that routine sagittal cervical realignment is possible within relatively short time periods (e.g. 8-12 weeks).6 CBP technique is a full-spine and posture correcting method that incorporates engineering principles into its approach.10 CBP applies the mirror image concept in terms of translations and rotations of posture as well as incorporates unique spinal traction methods including extension traction to restore the normal sagittal curves of the spine.10–14 High quality evidence points to better long-term patient outcomes associated with realigning the spinal column towards its normal/ideal configuration versus standard physiotherapeutic approaches that do not change the spine and posture.6
Despite many clinical trials supporting cervical lordosis correction in the treatment of various craniocervical ailments in patients presenting with hypolordosis,6–9 all involve the adult population. There appear to be no clinical trials involving the rehabilitation of the cervical lordosis in children.
Recently we documented the presence of many case reports demonstrating cervical lordosis correction by CBP methods and that in general, these are in good agreement with the results from the clinical trials on these same methods.15 Since there are no clinical trials on the pediatric population using CBP methods, a summary of pediatric case reports on cervical lordosis correction may provide important clinical data and direction.
The purpose of our paper to is characterize the existing literature on cervical extension traction methods as a part of CBP technique as applied to the structural rehabilitation of the cervical sagittal alignment in pediatrics. Additionally, we offer suggestions for the improvement of future clinical investigations and areas of needed research.
Method
This literature review screened for case reports and series reporting on pediatric patients who underwent cervical extension traction as a part of receiving CBP treatment aimed at improving a defined cervical hypolordotic curvature. As mentioned, CBP technique is a spine and posture correcting system of specific adjusting, exercise, and sustained loading procedures (called ‘extension traction’ in the sagittal plane) that are applied to precisely/uniquely correct displacements defined using mechanical engineering concepts.10–14 Specifically, regarding treatment directed at improving cervical lordosis, extension traction is incorporated to re-establish lordosis by creating viscoelastic creep deformation of the anterior column soft tissues such as the anterior longitudinal ligament and discs of the cervical spine.
The CBP NonProfit (NP) website lists all CBP publications including case reports/series (n=129).16 Since the CBP NP website is updated every fall, a literature search in the Pubmed and Index to Chiropractic Literature (ICL) databases was performed to locate possible cases published within the last year. Search terms included iterations of cervical spine, cervical lordosis, forward head posture, pediatrics, Chiropractic Biophysics, CBP, traction, improvement and restoration. Only peer-reviewed cases were considered.
Reports then had their references screened for additional publications . Authors known to have multiple case reports involving CBP traction methods were also individually searched in ResearchGate, ICL and Pubmed to locate any recent relevant cases. The inclusion criteria included pediatric ages (<16 years), case reports or case series, and use of cervical extension traction methods as part of a multi-modal structural rehabilitation program.
Cases were reviewed to extract the data pertaining to radiographic metrics, including cervical lordosis, atlas plane line (APL), anterior head translation (AHT), as well as details of patient demographics including age, sex, height, weight, chief complaint. Treatment specifics including traction set-up and time, treatment duration, number of treatments, exercise protocols and adjustment protocols were recorded as was any information pertaining to pain, disability or quality of life rating. The first 2 authors extracted the outlined details privately and then compared information. Any discrepancies were satisfied by consensus.
RESULTS
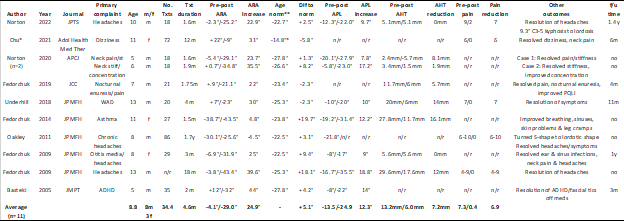
There were 11 cases reported in 10 unique publications (Table 1).17–26 Only 1 case was located from the literature search within the last year17; all others were listed on the CBP NonProfit website.16 The average age of the pediatric patients was 8.8years (range: 5-13yrs) and included 8 males and 3 females. The average number of treatments was 34.5 over an average duration of 4.6 months. On the post-treatment lateral cervical radiograph there was a 25° increase in cervical lordosis, a 12.3° increase in APL and a 7.2mm reduction in AHT. There was an average 6.9 point improvement in pain severity on the numerical rating scale.

The range of primary complaints documented to be improved after treatment included asthma, attention deficit hyperactivity disorder (ADHD), concentration difficulty, dizziness, headaches, neck pain, neck stiffness, nocturnal enuresis, otitis media and whiplash associated disorder.
Six of 11 cases reporting details of a long-term follow-up assessment, ranging from 3 months to 1.5 years after the initial course of care. (Table 2).17,18,20,21,25,26 Most of the cases reporting a post-treatment follow-up (with and without maintenance treatments) lacked details of follow-up outcomes other than the chief complaint of the child which was universally reported to be maintained.

DISCUSSION
This review located 11 pediatric cases as documented in 10 separate published reports on the success of CBP cervical extension traction methods as part of a multi-modal structural rehabilitation program of care to increase the cervical lordosis. On the post treatment radiographs, there was an average 25° improvement in cervical lordosis, 12° improvement in APL and 7mm reduction in AHT after completion of 34.5 treatments over the course of 4.5 months.
A unique consideration in treating the pediatric cervical lordosis is that the limited normative data suggests that the curve is largest at the younger ages (i.e. 2 years), slowly decreases until age 9, then increases again until approaching the adult magnitude at approximately age 18 years.27 Using the limited available data, Table 1 suggests most reports document some over-correction of age-appropriate lordosis (8/11 cases). Thus, it seems prudent to re-assess the pediatric spine more frequently than an adult spine to prevent achieving an over-correction. Additionally, more research is needed to identify the exact range of cervical curvatures that could be considered normal at different ages. The 1 report that could be located providing a cut-off value for the minimum amount of cervical lordosis need in the pediatric spine was from McAviney et al.28 Here, the authors identified that pediatric populations aged between 9 years and 18 years where twice as likely to have neck pain when the cervical lordosis (ARA C2-C7) was less than 20°; furthermore, straight and kyphotic curves were 18 times more likely to have neck pain compared to a match control population.28 Thus, it seems reasonable to recommend a cervical curve of at least 20° as an outcome of corrective care in pediatric populations.
The average degree change in lordosis per treatment session equates to 0.7° (Table 1: 24.9° change/34.4 treatments). This is greater than the data from the trials involving adults which demonstrate about 0.45°/treatment.6,14 Thus, the limited amount of case data herein indicate that pediatric cervical spines more rapidly change when applying corrective vectors to increase lordosis. Again, the treatment protocols must be altered when treating the pediatric patient by extension traction methods, for example, radiographic re-assessment should be performed more frequently than when treating an adult; where a range from 18-24 total sessions could be applied prior to a post-treatment radiograph vs. 30-40 total sessions in adults.
This review builds on a dated review (2015) that located 5 CBP case reports documenting improvement in cervical lordosis in pediatric patients.29 The earliest located case included in this review was published in 2005. Thus, over 18 years, 10 reports were published, which translates to approximately 1 case published every 2 years. As discussed, since there is no clinical trial data on CBP extension traction methods involving pediatric populations, case reports serve as the only evidence. This review highlights the need for more case reporting on the treatment of pediatric patients by CBP methods as well as formal clinical trials.
Every case report featured herein demonstrated improved health outcomes involving craniocervical ailments (headaches, neck pain) as well as non-related symptoms (e.g. ear infections, sinus infections, fascial tics, skin problems, improved concentration, nocturnal enuresis). This is clinically important. This limited dataset shows what chiropractors have claimed for generations, that chiropractic treatment has whole body effects, not just pain-relief, in selected case reports. Further pediatric-dedicated studies are required to elucidate how chiropractic treatment incorporating cervical lordosis restoration may impact whole body function.
The allopathic community may not recognize the importance of the cervical lordosis; many medical radiologists do not report on cervical subluxation.30 That is, medical radiologists have been documented to inaccurately report normal cervical alignment or not even comment when there is actual significant cervical malalignment present on the lateral cervical radiograph.30 Additionally, in the management of pediatric patients, radiation concerns have shifted focus away from routine spine imaging for children.31 Problematically, since it is known infants are born with a lordotic neck curve,32 that there are considerable adverse effects for straightened and kyphotic infantile cervical spines,33 and that the normal alignment throughout child growth is lordotic,27 X-ray imaging remains the most efficient method to screen for cervical spine deformity.
The failure to diagnose cervical subluxation may lead to underdiagnosis and undertreatment of potential cervical deformity. We concur with Norton et al. who state “Routine X-ray of the cervical spine is recommended for patients presenting with craniocervical symptoms as spine alignment is often overlooked as pathognomonic for these conditions.”17 Cervical subluxation is implicated in many common cervical-related conditions in adults28,34–36 and may be implicated in many common cervical-related conditions involved in children.28,33
Limitations to this review include the limited number of located cases. No detailed analysis was possible due to limited cases and limited reporting of all relevant details (e.g. X-ray metrics, pain rating). Future case reports involving pediatric patients treated by CBP extension traction to increase cervical lordosis should consider the end goal lordosis magnitude relative to its suggested age-appropriate range. Cases should detail all relevant radiographic parameters as well as include at least a 6-12 month follow-up. Since there are few reports overall, there is a need for more cases and case series in the treatment of craniocervical ailments in pediatric populations.
Conflict of interest
Dr. Paul Oakley (PAO) is a paid consultant for CBP NonProfit, Inc.; Dr. Deed Harrison (DEH) teaches chiropractic rehabilitation methods and sells products to physicians for patient care as used in this manuscript.