



INTRODUCTION
Although the sacroiliac joints (SIJs) are often involved in patients with low back pain,1 reliable and valid methods for assessing motion of the SIJ has been lacking.2 Some have recommended using clusters of pain provocation tests combined with motion analyses when evaluating the SIJ joints for dysfunction.3–5 The Gillet test6–8 is used to assess motion at the sacroiliac joint (SIJ). It has also been described as the step test,9 the 1-legged stance test,7 and stork test.10,11 Although there is some variation in the method, most examiners place 1 thumb on the posterior superior iliac spine (PSIS) and the other thumb on the S2 tubercle of the sacral base (SB). The traditional expected normal finding in performing the upright Gillet test is understood to be posterior and inferior rotation of the innominate bone with respect to S2 during hip flexion . Kapandji explains that hip flexion results in hamstring tension, thus drawing the innominate bone posterior.12 The interpretation of the Gillet test is as follows: if the SIJ is movable, the PSIS thumb moves caudally in relation to the S2 thumb when the patient flexes the ipsilateral hip and supports weight on the other leg.13 This movement has been understood to be monotonic, suggesting that increasing hip flexion resulted in greater SIJ movement. Presumably for this reason, some authors recommended asking the subject to flex the hip to 90° or even as much as possible14 to render caudal PSIS movement more evident.
At least 2 investigators have found the Gillet test to be potentially non-monotonic. Arab3 noticed possible “paradoxical” reversal of PSIS movement (relative to S2) in a cephalad direction as the hip increased its angle of flexion. Similarly, in a very small exploratory study, Cooperstein et al15 reported that although relatively small amounts of hip flexion were usually associated with caudal movement of the PSIS, larger amounts of hip flexion were associated with a change in direction, to cephalad PSIS movement. For movable SIJs the peak amount of motion detected by the Gillet test was at approximately 30° of hip flexion, beyond which the PSIS usually reversed course and moved cephalad in relation to S2.
These observations led to a more comprehensive follow-up study16 which concluded that the interpretation of the Gillet test was confounded by the fact that subjects tended to shift their body weight over the weight-bearing leg during the test. This would lead to pelvic obliquity, creating the mere appearance of SIJ movement, even in the absence of intrapelvic joint movements. When that occurred, pelvic tilting rather than intrapelvic joint movements accounted for the PSIS assuming a more caudal position in relation to S2. Cooperstein et al16 found that the asymptomatic subjects used in the study seemed to exhibit different balancing strategies depending on which SIJ was being tested. For small amounts of left hip flexion, the pelvis initially sagged on the left, creating what may have been the mere appearance of SIJ movement. However, beyond 30° of left hip flexion, leaning toward the right support leg elevated the left innominate bone, obliterating even the appearance of SIJ movement. During right hip flexion, the subjects immediately shifted their weight over the left support leg, such that the pelvis tilted superiorly on the right. According to the traditional interpretation of the Gillet test, this might have given the impression of SIJ hypomobility on the right, even though the cephalad movement of the PSIS may have reflected pelvic tilting rather than intrapelvic joint movements.
The authors reasoned as follows: if the traditional understanding of the Gillet test were correct, their findings were tantamount to having found most left SIJs movable, and most right SIJs hypomobile. It seemed more plausible that the results of the Gillet test could be wholly or partially explained by mere pelvic tilting, by typical asymmetry in 1-legged stance balancing strategies.
Having found the upright Gillet test not useful to assess SIJ movement, Cooperstein et al16 suggested as follows: “There may be ways to mitigate the impact of asymmetric one-legged stance strategies by performing a Gillet-like motion palpation test in a non-weightbearing position. In principle, this would allow discrimination of SIJ movement from pelvic obliquity as a determinant of relative PSIS and SB positions.” To follow up on this suggestion, we began practicing a side-posture version of the Gillet test. It became apparent that active hip flexion to 45° resulted in pelvic obliquity, superiorly on the flexed hip side; and that this effect was bilateral. The spine appeared to accommodate active side-lying hip flexion by become concave on the upside. Among the major hip flexors (psoas, iliacus, rectus femoris, and sartorius) only psoas connects directly to the lumbar spine. This led us to conclude that active hip flexion in the side-lying position drew the pelvis cephalad toward the spine, creating pelvic tilt that could create the mere appearance of SIJ hypomobility, not unlike what may be seen in the upright Gillet test during left one-legged stance. During these practice-sessions it also became clear that when the hip was brought into flexion passively by a Research Assistant (RA), the pelvis did not laterally flex, nor did the spine assume lateral curvature.
The primary goal of the present study was to determine the feasibility of gathering data using a side-posture version of the Gillet test. The secondary goal was to determine whether the results depended on whether the hip on the tested side were flexed actively by the subject, or passively flexed by an RA. In the apparent absence of any previous reports on a side-posture of the Gillet test, the purpose of the study was not so much to gather data that would support or refute clinical hypotheses, but rather to test the feasibility of obtaining observational data in performing this version of the test.
METHODS
This study was approved by the college’s Institutional Review Board. All subjects were required to provide written informed consent prior to participation. A convenience sample of asymptomatic subjects was recruited, the inclusion criterion for which was being able to flex both hip joints without pain. Subjects with sacroiliac pain >2/10 on the day of the study were excluded.
Each subject was positioned in side-posture, 7 inches from the side of a standard chiropractic bench-style table. The subject’s lower leg was flexed 45° at both the hip and knee by means of aligning the downside leg to 2 strips of tape on the table, serving as a template to approximate the aforesaid angles. An experienced clinician (33 years of practice) sat behind the subject in a position wherein he could apply one thumb to the upside PSIS and the other thumb to the S2 sacral tubercle, with the thumbs colinear and perpendicular to the plane of the table. The examiner’s thumbnails were marked with a line drawn in the middle of the nail and parallel to the length of the finger (Figure 1). The examiner looked away the subject or closed his eyes while palpating. A baseline photograph was taken with the examiner’s thumbs in position, prior to initiating any hip flexion on the tested side (Figure 2). To assess the results of active hip flexion, the subject was asked to flex the upside hip until the upside leg was juxtaposed over the downside leg (Figure 3). The subject then returned the upside leg to the baseline condition of no hip flexion. To assess the results of passive hip flexion, an RA used both hands to position the upside leg so that it was juxtaposed over the downside leg; the subject was carefully instructed to not voluntarily help create the movement (Figure 4). The entire protocol was then repeated on the other side of the subject’s body. The assessor alternated from subject-to-subject as to which SIJ was examined first.




A digital camera was mounted on a tripod placed directly behind and above the seated examiner, with the lens focused on the subject’s PSIS and sacral base. For each subject, 6 photos of the pelvis were taken, 3 on each side: baseline with no hip flexion, during active hip flexion, and during passive hip flexion created by the RA.
Analysis of photographs
Digital photographs were analyzed using a graphics program (Paint, Microsoft; and GIMP, Gnome.org) that measured coordinates of the thumb positions at the PSIS and S2. Pixel distances on the screen were transformed into millimetric equivalent distances by using a conversion factor based on the width of the examiner’s thumbnail as measured in both pixels and millimeters.
Each of 2 RAs determined the coordinates of the PSIS and S2 on each photograph. For any difference in photometric analysis of greater than 3 pixels, the RAs re-assessed the photograph until consensus was achieved.
Statistical analysis
To assess inter-examiner reliability in the photometric analysis, intraclass correlation coefficients (ICCs) were calculated for the 2 RAs’ baseline measurements for the PSIS and S2 coordinates on the left. The mean value for each photometric measurement was entered into statistical analysis. The coordinates for the PSIS and S2 were obtained in each of the following positions: upside hip in neutral position, in active flexion, and in passive flexion.
This allowed computation of the change in the relative PSIS/S2 positions during both active and passive hip flexion compared to the neutral position. The Wilcoxon signed-rank test was used to assess whether there were statistically significant differences. Analyses were performed for the entire dataset, as well as for subsets stratified by gender and by Body Mass Index (BMI).
Results
Thirty-four subjects were recruited for the study, all of whom satisfied the inclusion criteria. Table 1 presents their demographic information.
The ICC1,2 for the 2 RAs in in identifying the coordinates for the anatomical landmarks in this study, the PSIS and S2, could not be distinguished from 1.0, p<0.0001.
The primary study outcomes are presented in Table 2. During left active hip flexion, the PSIS moved cephalad 2.22 mm in relation to S2, and 2.33 cephalad during right hip flexion (row 1). During left passive hip flexion, the PSIS moved 1.80mm caudally in relation to S2, and 1.60mm caudally on the right (row 2). The Wilcoxon signed-rank test confirmed that the differences in rows 1 and 2 were statistically significant.
On the left 26.5% of joints exhibited no movement, while on the right 29.4% exhibited no movement. Overall, 27.9% of joints exhibited no movement. Among the 72.1% of joints that showed some movement, the average amount was 3.20mm on both the left and right sides.
The full dataset of 34 subjects was divided into 2 subsets to determine if BMI interacted with PSIS/S2 positional differences during passive hip flexion. Although there was a tendency for the 17 subjects whose BMI was less than 24.4 to exhibit less caudal movement of the PSIS than the other 17 subjects (1.06mm compared to 2.54mm on the left, and 1.49mm compared to 1.72mm on the right), independent t-testing did not show a statistically significant difference (2-tailed p=0.29 on the left, 2-tailed p=0.86 on the right). The full dataset of 34 subject was also divided into 2 subsets based on gender. There was no difference in the PSIS/S2 positional differences compared to baseline between the genders: (p=0.86 on the left, p=.94 on the right).
DISCUSSION
Feasibility studies “enable researchers to assess whether or not the ideas and findings can be shaped to be relevant and sustainable. Such research may identify not only what—if anything—in the research methods or protocols needs modification but also how changes might occur.”17
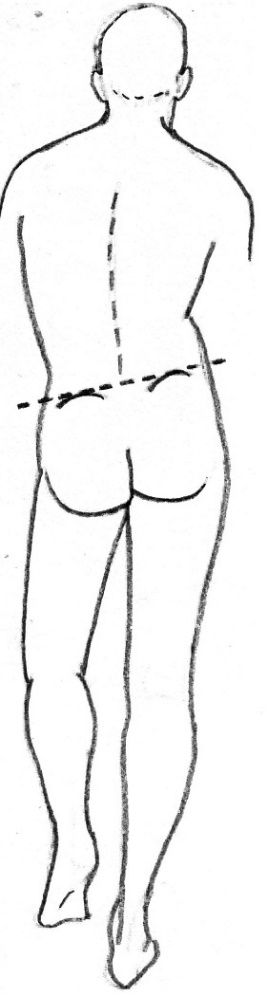
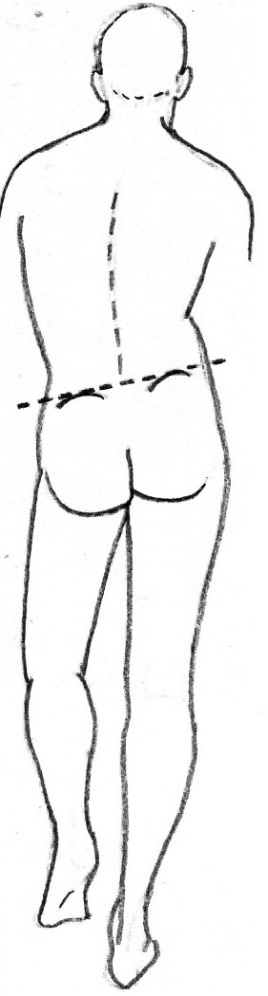
The current investigation was a feasibility study intended to determine whether a side-posture version of the Gillet test would be appropriate for further testing, either as a standalone test or as part of cluster of tests. Since it became apparent during rehearsal sessions that having the patient actively flex the hip on the tested side produced confounding pelvic obliquity, we considered limiting this feasibility study to passive hip flexion. However, we thought it would be instructive to gather data for active hip flexion as well, to demonstrate that side-lying active hip flexion could result in the same ambiguity seen in upright Gillet testing. Figure 5, which depicts a positive Trendelenburg sign for delayed activation or weakness of the gluteus medius, indicates how standing on 1 leg can create the appearance of the PSIS moving caudally in relation to S2, whereas in fact all that has occurred is sagging of the pelvis, or tilting of the pelvic frame of reference.
I previously reported15 that for small amounts of hip flexion this Trendelenburg-like effect was typical during 1-legged stance on the right, granted that the amount was so small that individuals would not be judged as having a positive Trendelenburg sign. It hardly ever occurred during 1-legged stance on the left. This observation was consistent with Kendall’s finding18 that the left gluteus medius muscle tends to be stronger than the right gluteus medius. The gluteus medius tends to be weaker on the side of handedness, usually the right.18 Apparently, most right-handed individuals find it easier to balance on the left leg, because they more often engage the right leg for kicking and other physical endeavors.
Although estimates for SIJ motion vary depending on the postures and movements of the study subjects, there is a tendency for high-tech methodology (e.g., Roentgen stereophotogrammetric analysis) to detect only slight amounts of SIJ movement. Some authors have argued that the movements of the SIJ are so slight that a manual palpator would not be able to assess the presence or absence of such movements.19–21 Granted that the results of a feasibility study are less important that the testing of the method, we think it worthwhile to briefly compare our quantitative results to those of high-tech studies of SIJ movement.
Based on the finding that a typical innominate bone is 133mm in width,22 we determined trigonometrically that each degree of innominate posterior rotation about a transverse axis through the symphysis pubis23 would correspond to 1.7mm of caudal PSIS movement. Since the sacrum would likely travel posteriorly to some extent with the innominate bone, we rounded this down to approximately 1mm, a heuristic estimate. Therefore, among the 72.1% SIJs in our study that showed at least some movement, the approximately 3mm we measured implied approximately 3° SIJ rotation. Goode et al,19 in their systematic review of three-dimensional movements of the SIJ, included a table titled “Measures associated with report of rotation about the sij during lower extremity initiated movements.” Among the studies included in this table, only that of Smidt et al,24 which used fresh cadavers, created hip flexion passively, as we did in our study. In their study SIJ rotation during reciprocal hip flexion/extension in the side-lying position resulted in 4° (-4 to +3) on the left and 4° (-3 to +2) on the right, slightly exceeding the 3° we reported, perhaps because we did not introduce reciprocal hip extension.
Gluteus maximus, piriformis, quadratus lumborum, lumbar paraspinal, and other muscle groups have direct effects on the SIJ joint mechanics. In upright stance these postural muscles activate to maintain proper balance and assist the SIJ joints in weight bearing, owing to SIJ form-closure, the self-bracing nature of the SIJ in the upright position.25 Snijders et al26 developed a biomechanical model for the sacroiliac joints under load in which there is a self-bracing effect that protects them against shear. This muscle activation may alter an examiner’s ability to accurately assess motion in the sacroiliac joint as the hip actively flexes. By comparison, passive side-lying hip flexion may result in more measurable SIJ movement than upright hip flexion,
Limitations of the study
Since this was a feasibility study, no power analysis was performed to establish the number of subjects to be recruited. The asymptomatic subjects in our study were not representative of patients who generally undergo Gillet-like sacroiliac testing; it is possible that using symptomatic subjects would have resulted in different findings. As an observational feasibility study, our study was not intended to address the reliability of the Gillet test. All assessments were performed by one examiner; other examiners may have achieved different results. There may have been some slippage of the palpated landmarks from the bony landmarks during hip flexion. Although we suspect the caudal movement of the PSIS relative to S2 during passive hip flexion reflected SIJ X-axis rotation, there may have been some confounding frontal plane pelvic tilting (granted that using passive hip flexion was meant to mitigate that concern). Although subjects were asked to not assist in flexing their hip, some of them may not have fully complied with this instruction. We could not find any literature on which muscles effect active hip flexion in the side-posture position, which appeared to produce pelvic tilt; electromyography could address that issue. Although data were gathered on the subjects’ history of past and present SIJ and lumbar pain, there weren’t enough symptomatic subjects in the study to draw any conclusions. The photometric analysis used in our basic science study would most likely be impractical in a typical clinical setting, where a more qualitative and immediate impression of “moving or not moving” would be a more feasible outcome. In our experimental setting, the examiner sat behind the side-lying subject, thumbs in place, while an RA placed the subject’s leg into passive flexion. It was somewhat awkward to keep the thumbs in place, but with some practice the caudal movement of the PSI relative to S2 could not only be visualized but also tactilely experienced by the palpator. Since having an assistant available to perform this side-posture version of the Gillet test cannot be assumed in a private practice setting, the external validity of this procedure remains to be seen.
CONCLUSION
This study demonstrated that it is mechanically feasible to perform a Gillet-like SIJ motion test in side-posture to identify putative SIJ hypomobility, which most manual therapists believe clinically relevant to sacroiliac pain. I have been performing the test in my own private practice setting by creating hip flexion with 1 hand while palpating with digits 2 and 3 (or 1 and 2) of the other hand. Although it is more challenging to perform the test unaided by an assistant, especially when the patient has a relatively heavy thigh, the issues do not seem insuperable.
Although the primary purpose was to assess the potential for successful implementation of the methodology, the quantitative results are also of some interest, since the amount of SIJ movement detected was consistent with prior radiostereometric computations for passive side-lying hip flexion.24 In the present study, 72.1% of 68 tested SIJs exhibited some degree of caudal movement of the PSIS in relation to the S2 tubercle during passive flexion of the hip, indicative of possible posterior innominate rotation. It was important to create this hip flexion passively, in order to reduce the lateral flexion of the pelvis on the spine that occurs if the psoas muscle contracts actively and concentrically. During active flexion of the hip, the PSIS moved cephalad relative to S2, presumably due to lateral flexion of the pelvis that obscures possible caudal movement due to SIJ motion. The overarching conclusion is that it does seem feasible to assess SIJ movements using a side-posture version of the Gillet test, provided the hip flexion is created passively.
Clinicians should determine whether they find this side-lying version of the Gillet test practical in their individual settings, especially when an assistant is not available. The stage is set for interexaminer reliability studies, as well as a validity study to determine whether examination findings are related to the patient’s clinical status (such as established sacroiliac joint dysfunction). More definitive validity testing might involve using a very accurate measuring system (such as Roentgen Stereophotogrammetric Analysis) to establish typical amounts of SIJ motion seen during passive side-lying hip flexion, similar to the methods of the cadaveric study of Smidt et al.24 That would help us understand if the amount of SIJ movement measured in our study is within the limits detected using accurate instrumentation.
Conflict of interest statement
Dr. Cooperstein has no commercial interest in the results of this study.
Funding
This project was internally funded by the Palmer College of Chiropractic