

INTRODUCTION
Shoulder pain is a common condition that adversely affections millions of Americans each year. Point prevalence rates have been shown to range from 6.9-25%, while lifetime prevalence rates range from 6.7-66.7%. Chronic pain prevalence rates range from 15.5-50%.1 The incidence of adhesive capsulitis, or “frozen shoulder,” is approximately 3-5%, but is as high as 20% in patients with diabetes mellitus.2
There are no specific tests for diagnosis of adhesive capsulitis, as the condition is usually diagnosed once other causes of stiff and painful shoulders are ruled out.3 Adhesive capsulitis is characterized by pain and significantly decreased range of motion. While it is often reported that adhesive capsulitis is a self-limiting condition that resolves over 12-36 months, many long-term follow-up studies have shown that even with standard treatment, up to 50% of patients have long term pain and motion limitations after this period.4,5 This suggests that current treatments may not be effective.
The McKenzie Method of Diagnosis and Therapy (MDT) has become a valid and widely accepted method of classification and treatment, especially related to spinal issues. MDT uses a classification system to guide treatment. Regarding classification of painful disorders of the extremities, trained therapists have demonstrated approximately 92% agreement on classification.6 Specifically regarding shoulder pain, agreement was shown to be even higher, approximately 95%.7 Classifications are based on patient history as well as patient response to repeated movements and positions during the examination. The goal of the examination is not to find a specific diagnosis, but rather to classify the condition in order to find the most effective treatment, as each classification requires a unique treatment approach.8 There are 4 potential classifications of conditions: derangements, dysfunctions, postural, and other.8 A derangement is defined as a “mechanical obstruction of an affected joint” while a dysfunction is a “mechanical deformation of structurally impaired soft tissues.”8 These 2 classifications are the most common.6,7 Within the classification of derangements is a further identification of directional preference, where loading the joint in a specific direction is required for improvement of symptoms.8 In the spine, using an exercise in the directional preference of a patient will yield more effective results than using an exercise in the opposite direction.9 Thus, proper classification and proper exercise selection is vital for treatment.
Thoracic spine manual therapy and manipulation has been used for a wide array of conditions.10 Regarding the shoulder, a review by Peek et al showed that thoracic spine manual therapy accelerated recovery while also reducing pain and disability compared to typical care for non-specific shoulder pain.11 Another study showed that high-velocity thrust manipulation applied to the thoracic spine or upper ribs resulted in immediate post-treatment reductions in pain and improvement of shoulder range of motion.12
There is some debate as to the mechanism by which thoracic spine manual therapy works. Some, like Wainner et al, argue that “regional interdependence,” or the tendency for dysfunction in 1 part of the body to affect another region, is the driving force.13 If this is true, treating 1 area can often improve symptoms in another area. Others believe the neurophysiological effects, such as hypoalgesia, or non-specific effects (placebo, patient expectation) may be responsible for the change in symptoms.14
Instrument-assisted soft-tissue mobilization (IASTM) is a method for treatment of dysfunctional soft tissues, namely fascia, ligaments, muscles and tendons. The theory proposed by clinicians and researches is that IASTM produces a micro-trauma to the treatment tissue, which then initiates the body’s inflammation, healing and repair processes.15,16 IASTM uses instruments specifically designed for this approach. The method is still in its infancy, and a recent review noted that current research has shown only “insignificant results” for various pathologies, but there is evidence for providing short term range of motion increases.17 Laudner et al. showed that using IASTM lead to acute improvements in shoulder range of motion in collegiate baseball players.18
The purpose of this case report was to highlight the use of MDT, thoracic manipulation and IASTM in the treatment of a patient presenting symptoms that would often be diagnosed as adhesive capsulitis. The patient’s syndrome was classified as a derangement using MDT principles, and a directional preference was found and even changed from visit 1 to visit 2. Thoracic manipulation and IASTM were also utilized as both have been shown to improve range of motion in the shoulder.
CASE REPORT
The patient was a 59-year-old retired but active female with severe right shoulder pain and mobility limitations. She self-referred to a chiropractic and rehabilitation clinic. She reported that the pain started insidiously approximately 1 month prior to seeking treatment, and had been steadily worsening over the previous 2 weeks. She reported significant limitations with moving her arm, driving and caring for her elderly mother. A thorough review of systems was conducted which was negative except for her shoulder pain as well as a history of multiple hereditary exostoses (MHE). Regarding her history of MHE, the patient reported bony tumors around her forearms and knee areas but had no history of tumors in her shoulder region. She filled out a Disabilities of Arm, Shoulder Hand (DASH)19 outcome measure, which showed 57.5% disability. She reported constant pain that ranged from 5-9/10 on the numerical pain rating scale (NPRS).
Upon examination, both passive and active ranges of motion for the right shoulder were found to be severely restricted and painful compared to the left, (Table 1). Most orthopedic tests were deferred, due to the severe lack of motion. Resisted shoulder internal rotation was 5/5 without pain bilaterally. Testing of external rotation revealed 4+/5 strength of the right shoulder with pain. Tenderness to touch was found along the anterior and posterior shoulder region along with the spinous processes of the upper thoracic spine. Cervical range of motion was within normal limits and without pain. Thoracic range of motion was within normal limits with only thoracic extension eliciting minor end-range pain.
Repeated motion testing was then performed, with a focus on any change in symptoms or motion. Per MDT methodology, the cervical spine and thoracic spine were tested first. Twenty repetitions each of cervical flexion, cervical retraction and cervical retraction plus extension were performed with no change to symptoms. Twenty repetitions of thoracic extension and flexion were also performed without change to shoulder symptoms, but patient did report end range pain and stiffness during thoracic extensions. Shoulder motion testing was then initiated. Twenty repetitions of shoulder extension were performed, with no change in symptoms. Ten repetitions of flexion were then performed, which increased her symptoms and led to a decrease in active abduction range of motion. The next motion performed was passive shoulder adduction behind her back using a belt (see Figure 1). Twenty repetitions of this motion resulted in a mild decrease in pain and active abduction and flexion of approximately 40°. Based on the findings during the repeated motion exam, the patient was classified as having a shoulder derangement with a directional preference of adduction. She was sent home with the instructions to perform the belted adduction for ten repetitions five times per day and return to the clinic the following day.

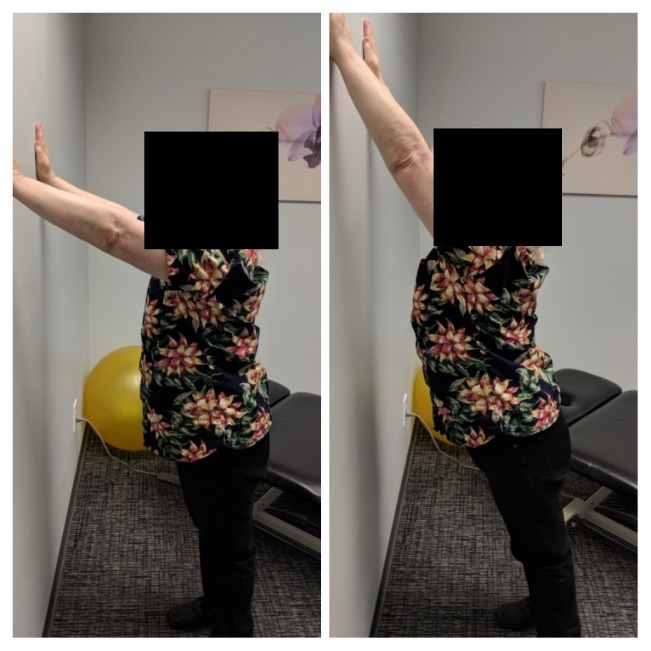
On visit 2 (~30 hours after initial visit), she reported improvement of pain to a level of 3/10 on the NPRS, but motion was still limited. A few sets of the belted adduction exercises were performed to verify correct form. No change was produced during these exercises, so repeated movements were tested again. Shoulder extension again produced no change in symptoms. Repeated shoulder flexion then produced a decrease in pain and increase in flexion, abduction and Apley’s internal scratch test. Thus, her directional preference had changed. She was told to discontinue the belted adduction exercises and to now perform the shoulder flexion exercises five times per day. Figure 2 shows the start and ending positions for the shoulder flexion exercise.

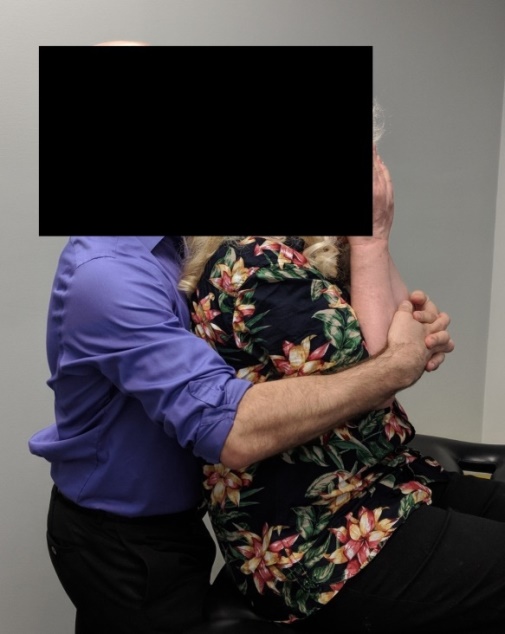
On visit 3 (4 days after initial visit), the patient reported her pain as no longer being constant and rated it as a 3/10. She was very excited that she could now curl her hair on her own and use her right arm while driving. Examination confirmed flexion once again as the directional preference. To further increase her range of motion, a decision was made to incorporate thoracic manipulation and IASTM. A seated thoracic long axis-distraction procedure was performed (see Figure 3). For IASTM, a tool produced by Ascension Biosystems was used (Figure 4). IASTM was applied to the anterior and posterior shoulder for approximately 30 seconds with the patient in a seated position. The patient was then instructed to perform a set of her shoulder flexion exercises while the clinician performed IASTM around the shoulder area simultaneously. This treatment (shoulder flexion exercises, thoracic spine manipulation and IASTM) was repeated on the fourth visit as well.


On the fifth and final visit (11 days after initial visit), the patient reported her pain as a 0/10 on the NPRS. She reported no limitations with range of motion or with any activities. Range of motion examination was performed again and the results are shown in Table 2. Following another treatment of thoracic manipulation and IASTM, the patient was told to continue her exercises and return for a follow-up 2 weeks later. However, due to financial constraints, she cancelled her appointment. She was given another DASH outcome measure over the phone, which showed 0% disability. The patient provided consent for publishing of the case study without personal identifiers.
DISCUSSION
The patient had severe lack of shoulder motion and pain. Barring any other pertinent imaging or examination findings, a diagnosis of adhesive capsulitis would often be given to a patient with this presentation. Treatment would include some combination of physical therapy, pharmacological therapy, steroid injections and operative procedures. As mentioned previously, up to 50% of the time the patient would still have symptoms years after onset despite these treatments. There is a need for more effective treatments.
Pathoanatomically, adhesive capsulitis is characterized by a contracture of the glenohumeral capsule. This would be considered “mechanical deformation of structurally impaired soft tissues,” and classified as a dysfunction per MDT methodology. Treatment for dysfunctions would typically be repeated stretching into the restricted motions to “remodel” the tissue.8 This remodeling takes months to fully restore the restricted range of motion.
Here, the patient was classified as a derangement, due to having a directional preference and rapidly changing symptoms. The derangement is a unique classification used by MDT, and no corresponding medical diagnosis exists. A 2012 survey of MDT practitioners found that over 40% of shoulder issues were classified as derangements.20 This indicates the possible need for MDT training, as many shoulder issues may rapidly change if a directional preference exercise is given to the patient.
Typical MDT treatment for derangement involves end-range loading exercises of the directional preference. Mobilizations and manipulations are only used on the area of symptoms if patient-centered exercises fail to progress.8 In this case, both thoracic manipulations and IASTM were used in conjunction with the directional preference exercises. The clinical reason for use of these adjunctive treatments was twofold. First, the patient’s primary functional limitation was range of motion. Thus, any treatment option that can increase range of motion should be considered. As mentioned previously, both thoracic manipulation and IASTM have been shown to provide short term range of motion increases in the shoulder. Secondly, thoracic manipulations and IASTM may increase the effectiveness of the directional preference exercises. Increasing range of motion even temporarily provides a unique opportunity to perform the directional preference exercises in an increased end range immediately after treatment, which is the goal of treatment for derangements. However, more research is needed to judge efficacy of using adjunctive treatments in addition to standard MDT treatments.
A previous case report also utilized MDT for treatment of adhesive capsulitis that was classified as a derangement but there were a few key differences from this case study.21 First, the patient still had mild pain and functional limitations at conclusion of treatment. Also, a different directional preference was found compared to the patient in this study, indicating the need for individualized assessment and treatment. Finally, the only treatment in that case was directional preference exercises. Despite these differences, it appears that not all adhesive capsulitis patients have “true” adhesive capsulitis. For those cases where a directional preference is found, rapid change in symptoms may be possible.
CONCLUSION
The results of this case study suggest that the use of MDT classification and treatment, along with thoracic manipulation and IASTM of the shoulder, can be effective in shoulder pathology. While a single case cannot establish cause-effect relationship, it shows that this treatment method may be a useful approach in some patients that present with symptoms similar to adhesive capsulitis, especially when compared to typical treatment and its outcomes.
ACKNOWLEDGEMENTS
The author would like to sincerely thank Mike McShane, PhD for his help on editing.