

Introduction
Carpal tunnel syndrome (CTS) is one of the most common musculoskeletal disorders of the upper extremity.1 Technically it is defined as a “symptomatic compression neuropathy of the median nerve at the level of the wrist, characterized physiologically by evidence of increased pressure within the carpal tunnel and decreased function of the nerve at that level”.2
Although the best evidence is for surgical treatment, usually non-surgical treatments are attempted first. The most evidence-based non-operative treatments for CTS are splinting/bracing or steroid injections. Based on neurobiomechanics, however, any loss of the normal cervical lordosis will create a lengthening of the spinal canal, and this changes physiologic tensions to become pathologic tensions to be exerted onto the spinal cord.3,4 When some critical threshold is surpassed, the body’s inherent ability to compensate for deteriorating spinal posture will result in symptoms.
A recent case report5 and 2 clinical trials6,7 demonstrated that the improvement in cervical posture (increasing the lordosis; decreasing forward head posture) relieves radicular symptoms by decreasing the spinal canal length and alleviating the pathological tensions onto the cord/nerves. Based on this evidence and its logical etiological implications for upper cervical radiculopathy this method of treatment was the choice approach for the patient described in this case.
We discuss a case of the complete resolution of CTS in a patient who presented with a cervical kyphosis subluxation spinal deformity who was treated using CBP technique that features cervical extension traction and exercise methods for the rehabilitation of the cervical lordosis.
Case report
A male patient, aged 29, sought care for a chief complaint of CTS previously diagnosed by a medical doctor. The patient was 175cm in height and weighed 81.6 kg. He described his symptoms beginning in the fall of the previous year becoming constant for the previous 3 months.
The pain was described as bilateral in the elbows, worse on the right, and radiating numbness into both hands. The pain was described as dull and throbbing and was worst at 3:00-4:00 am. The patient stated the pain felt like “someone is hitting me with a hammer.” He had sought treatment from multiple healthcare providers including 2 walk-in clinics, 1 neurologist, received acupuncture as well as chiropractic treatment and had taken pain medication. All modalities had provided temporary symptom relief, but none had alleviated the issue.
He reported a history of excessive occupational overtime, kickboxing and heavy lifting. The activities of daily living most affected were reported to be his ability to play the clarinet and perform physical tasks at work. He stated that the problem was worsening despite the treatments he had received. Numerical pain rating scale (NRS) for pain severity was described as a 5/10 on average and a 10/10 at its worst (0=no pain; 10=worst pain ever). The patient scored low on several short form-36 health scale scores (Table 1).

Upon examination the patient had an obvious forward head translation posture. Palpation revealed muscular tightness and hypertonicity at the levels of C1 and C4-C7, bilaterally. Spinal x-rays were taken and measure using the PostureRay system (PostureCo., Inc., Trinity, FL, USA). This system uses the Harrison posterior tangent method to measure the cervical lordosis. This method is repeatable and reliable with a standard error of measure <3°.7,8 Posture is also repeatable and reliable.9
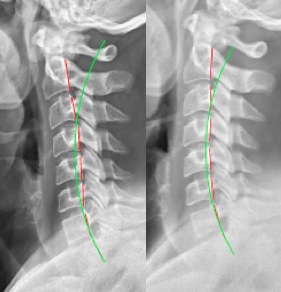
The patient had 16mm forward head translation (vs. 0-15mm normal10), and lordosis from C2-C7 of -3.7° (vs. -31-42° normal10,11), and an atlas plane line of -13.1° (vs. 24-29° normal10) (Figure 1). There was a cervical kyphosis deformity from C3-C5 of +10.3°. The patient also had a right-sided head translation of 11mm off of vertical midline (Figure 2).
_showing_cervical_kyphosis_from_c2-c6.jpeg)
_showing_an_11mm_right_head_.jpeg)
The patient was treated by CBP methods incorporating mirror image exercises, manual manipulation, and cervical extension traction designed to increase the cervical lordosis.12–14 CBP technique was created and Donald Harrison in 1980 and today has evolved into 1 of the most evidence-based posture correcting techniques.6,7,15–17
The proposed treatment plan was a frequency of 3 times a week for 8 weeks and 2 times a week for 4 weeks. Manual high-velocity, low-amplitude manipulations were given to the cervical spine bilaterally and mid-thoracic spine. Drop table adjustments were given in the prone position with the head and pelvic table pieces elevated, where with pressure placed on the thorax engages the thoracic drop-piece. This is to subtly jar the spine and stimulate joint mechanoreceptors as the patient is stressed into the mirror image, or improved postural position. The patient was also given bilateral full upper extremity adjustments to the shoulders, elbows and wrists. Finally, he was treated with the Arthro-stim (Impac Inc., Salem, OR, USA) hand-held adjusting instrument in a seated position along the cervical spine paraspinal muscles as his head was in an extended position, as well as in the prone position along the entire paraspinal muscles.
The patient was given home traction exercises on the cervical DennerollTM (Denneroll Spinal Orthotics, Wheeler Heights, NSW, Australia). He was to position the peak of the roll at C6 and lay supine over the roll for 10-20 minutes daily. This device is a proven cervical extension traction device. The patient was also prescribed left head translation exercises, 30 repetitions to be held for 10 seconds.
Results
Assessment after 13 treatment sessions revealed that our patient was ‘feeling great’ and back to normal. There was no longer numbness into his hands. Motion and static spinal palpation showed segmental loss of ROM at L4, T6, T5, C5, and C6. He was currently compliant and performing cervical extension traction daily for 15 minutes. The SF-36 scores showed significant improvements (Table 1).
An assessment after 31 treatment sessions revealed a reported 100% symptom relief of CTS related issues including no neck or elbow pain, no hand numbness, and no back pains. The patient also reported having performed the home cervical traction about 80% of the time. An updated SF-36 questionnaire showed a 100% score on half of the health indices, and above normal on all indices (Table 1).
An assessment a short while later (after 33 treatment sessions) showed the patient continuing to be well with no symptoms related to CTS. He reported that he performed the home traction most days of the week. The SF-36 questionnaire showed 5/8 indices at 100%, the rest above normal.
A radiographic assessment showed a correction of the original cervical kyphosis subluxation deformity, displaying an overall lordosis of -18.3° (vs. -3.7°) (Figure 1). The forward head translation reduced to 5.1mm (vs. 16mm), and the atlas plane angle increased to -24.7° (vs. -13.1°). The follow-up AP cervicothoracic radiograph showed a 50% reduction in right head shift (5.5mm vs. 11mm) (Figure 2).
DISCUSSION
This case demonstrates the resolution of CTS in a male patient having an initial pathologic upper cervical kyphosis that was reduced, and had an overall improvement in lordosis of 15°, as well as a reduction in a lateral head translation posture over a 13-week period.
In 1973, the ‘double crush’ hypothesis was proposed as an etiological event for the symptoms of CTS.18 Upton and McComas suggested that axons that are compressed at 1 site (cervical spine) are especially susceptible to damage at another site (wrist).18 This theory was substantiated by the work of Massey et al, who determined that in a sample of 19 patients, a co-existing diagnosis of CTS and cervical radiculopathy existed.19
As the nerves from the upper extremities arise from the cervical spine, we believe that the root cause of CTS is often from subluxation misalignment of the neck. This implicates that the correction of the cervical spine alignment would be the solution to CTS, as the ‘first crush’ in the double crush hypothesis would be eliminated; therefore, the ‘second crush’ would not be a sufficient enough of an irritation to cause symptoms.
There are now several randomized and nonrandomized clinical trials verifying the efficacy of CBP cervical extension traction methods to improve the normal physiologic lordosis.6,15–17,20 These methods will undoubtedly become a more popular treatment option for cervical spine disorders, including CTS, which we believe may be a cervical spine disorder. Further, the more combinations of head and cervical spine postures, the more complicated the potential impact and pathological tensions exerted onto the cord and nerves.21 Therefore, all abnormal postures of the head and neck need to be identified during comprehensive screening, in order to optimally restore physiologic posture22 in attempting to resolve neurological symptoms in a patient.
We believe that cervical lordosis screening is overlooked and not routinely performed in the clinical assessment of patients with CTS. As this case suggests, the cervical spine may be the key etiological factor in the evolution of CTS. We suggest that the primary screening in the initial examination of patients with potential CTS should include a visual and radiological assessment of the head and neck posture in the sagittal and frontal view with an emphasis on presence of the cervical lordosis.
One can question whether routine screening with x-ray is warranted given the perceived risk associated radiation exposures. Recent research suggests that radiation in the low-dose amounts given during radiography may not be harmful, and may potentially be beneficial.23–25 We recently wrote that, contrary to traditional ideology, “Radiography increases benefits and reduces risks”.25 This is a source of controversy in the chiropractic profession, though we cite supporting literature. We strongly believe that radiography is essential to diagnose cervical spine subluxation before a proper treatment may be applied; otherwise, misdiagnosis may occur and improper treatment given.
Limitations
Limitations to this case include that it is only a single case, and it also lacks a long-term follow-up. Further, because the patient received multiple treatments, it may not be determined which resulted in the correction of the cervical spine alignment. Randomized clinical trials by Moustafa and colleagues has definitively determined that extension traction corrects spine alignment, whereas many other physiotherapy modalities do not.16 Regarding the confounding issue of upper extremity adjustments, further research needs to answer precisely our theory of cervical spine alignment as representing as the ‘first crush’ in this disorder. Future research should investigate the role of cervical hypolordosis/kyphosis in the etiology of CTS.
CONCLUSION
Biomechanically a deviated cervical spine posture lengthens the spinal canal and exerts pathologic stresses onto the cord and nerves; consequently, further nerve irritation via upper extremity positions/movements may elicit outright neurologic symptoms consistent with carpal tunnel and related syndromes. We suggest treatment for carpal tunnel syndrome to be aimed at restoring normal cervical spine alignment as to remove the ‘first crush’ in this double crush syndrome. Further, routine assessment by radiography is recommended as a standard screening protocol for this disorder as it may offer a definitive etiology and is not harmful.