

INTRODUCTION
Cervical kyphosis is the reversal of the normal lordosis. It has traditionally been described as a secondary spinal curve during early development but has been demonstrated to occur at 7.5-9 weeks in utero.1 Cervical kyphosis is associated with a barrage of symptoms, including headaches and neck pains2; these 2 symptoms are often related and coexistent.
Although headaches are a common experience- for example, tension-type headaches are the most common headache worldwide3 affecting greater than 40% of the population4- neck pain is also very prevalent and will affect up to 70% of the population.5 Those suffering from headache have a high chance of also suffering from neck pain, a 90% prevalence rate,5 particularly following motor vehicle collisions (MVCs).6
People involved in MVCs may experience cervicogenic symptoms even years after the initiating event.6 While ‘whiplash’ refers to neck sprain-strain injury caused by a sudden acceleration-deceleration movement of the head that is typical in MVCs, ‘late whiplash syndrome’ (LWS) refers to the collection of symptoms and disabilities seen more than 6 months after a neck injury typically resulting from a MVC.7 LWS is common in women between the ages of 21-40 years.7
Cadaveric studies show that a classic whiplash force to the cervical spine creates an S-shaped configuration, specifically causing an upper cervical spine flexion and a lower cervical spine hyperextension.8 At the moment of impact, damage to the involved tissues will occur, but we hypothesized9 that the instantaneous alteration of cervical alignment during a MVC will lead to a perpetual source of stress-strain spinal tissue trauma that ultimately leads to delayed recovery from whiplash-type events and to the classic lingering symptoms typifying post-concussion syndrome (PCS).
Identifying altered cervical spine structure in those suffering from whiplash is important as its correction may lead to successful outcomes. Ferrantelli et al.10 demonstrated complete symptomatic improvement in a 40-year-old male who had suffered whiplash. Treatment resulted in a 25° improvement in cervical lordosis and reduction of forward head posture after 64 sessions of Chiropractic Biophysics® (CBP®) technique11–13 over an 18-week period.10 Fortner et al.14 showed a 13° improvement in cervical lordosis in a 31-year-old female after 30 treatments over 5 months who had also suffered from whiplash; CBP treatment was given and the patient improved quickly.
We discuss the successful resolution of LWS featuring chronic headaches, neck pain, and many other bodily symptoms in a 29-year-old, 13-years following an MVC. Treatment involved CBP technique, and a 1-year follow-up was also reported.
CASE REPORT
On January 29, 2016, a 29-year-old mother of 3 sought care for severe headaches. She suffered from headaches since being involved in a rear-end impact MVC 13-years previous where she was diagnosed with ‘severe whiplash.’ At that time, she was treated by a physiotherapist as well as a chiropractor, for 3 months. The headaches persisted, and seeking a second opinion, she was again diagnosed with ‘severe whiplash.’ She claims the headaches have slowly worsened over the years.
On the numeric rating scale (NRS) for pain, she reported her neck pain to average a 5/10 (0=no pain; 10=worst pain ever) and an 8/10 at worst. Her headaches were reported to be 8/10 with dizziness and nausea, her upper back averaged 4/10, and her low back pain averaged 8-9/10. All these ailments were chronic and bothersome on a daily basis. The Headache Disability Inventory (HDI) revealed a score of 98%, where a score of >60 is considered a significant disability due to headaches.15 The Neck Disability Index (NDI16) indicated a score of 70%. The SF-3617 demonstrated several categories having extremely low scores (Table 1).
__post-treatment_(5_20_16)__and_follow-up_(3_4_17).jpg)
She also reported numbness in her feet and legs. The overall pain prevented her from being able to hold her infant. She also reported having cold fingers, right arm pain, tinnitus, difficulty digesting greasy foods, low energy, restless legs, cramping, irregular periods, and pelvic floor weakness.
She had limited muscular strength for cervical flexion (4/5), left cervical rotation (4/5), and left hip flexion (4/5 with pain). There was loss of pinwheel sensation perceived as dull in the right arm dermatomes C5, C6, C7, and C8. Positive orthopedic tests included Jackson’s, maximum cervical compression, Soto-Hall, Yeoman’s, and Hibb’s tests. Grip strength was 28lbs on the right and 29lbs on the left. Posture analysis18 revealed a flexed head position (+RxH), a high left shoulder (+RzT), a left posterior pelvis rotation (+RyP), and right translated pelvis (-TxP).
Full spine radiographic assessment was performed including an anteroposterior (AP) and lateral cervical, thoracic, and lumbar series. All radiographs were digitized and analyzed using the PostureRay system (New Port Richey, FL). This system uses the Harrison posterior tangent method for lateral spine images,19,20 and the modified Risser-Ferguson method for AP spine images.20 These mensuration methods are repeatable and reliable, as is posture.19–21
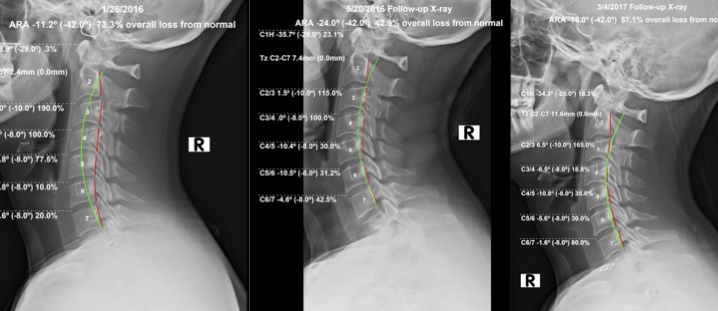
The lateral cervical spine view revealed an S-shaped alignment with an upper cervical kyphosis and lower cervical lordosis (Figure 1). The C2-C3 relative rotation angle (RRA) measured +9.0°; the normal angle of this joint should be 7-9° of extension.22 The overall cervical C2-C7 alignment absolute rotation angle (ARA) measured -11.2° (negative indicates extension), where normal is -31° to -42°.23–25 The atlas plane line (APL) was -28.9° (normal= -24° to -29°,23,24 and the forward head translation (+TzH) was within normal limits (WNL) at 2.4mm (normal 0-15mm23,24).

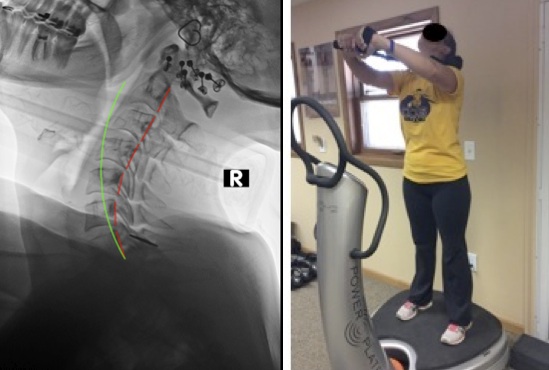
Stress films were performed to determine the flexibility of the cervical spine in extension, while the patient was performing a neck extension exercise (Figure 2) and while laying on a Denneroll® (Wheeler Heights, Australia), a firm rounded block (Figure 3). These films were deemed sufficient to recommend CBP cervical spine protocol12,13 as the patient could tolerate cervical extension.


She was treated with CBP protocol12,13 at a frequency of up to 3 times a week over 15-weeks, receiving 36 treatments before being reassessed (1/26/16 - 5/20/16). She was given neck extension exercises with resistance using the ProlordoticTM neck exerciser (Circular Traction, Huntington Beach, CA) while standing on the PowerPlate® (Northbrook, IL) while in the office (Figure 2). Other exercises included single leg stands and Russian twists on the PowerPlate. She was also prescribed 100 daily neck extension exercises to be performed at home.
In-house, Pope 2-way cervical extension traction26 was performed starting at 15lbs progressing to 25lbs for 20-minutes duration (Figure 3). She was also prescribed cervical Denneroll traction27,28 for home use starting at 5-minutes progressing up to 20 minutes daily with a mid-cervical placement (Figure 3). She was adjusted manually with the cervical spine in extension as well as with a hand-held adjusting instrument (Arthrostim®: Impac Inc., Salem, OR) into the upper cervical spine while having the neck extended in the prone position. She reported no pain caused by the treatment throughout her program and consented to the publication of these results including all images.
Outcome
She was re-examined. Right grip strength improved to 34 lbs., Soto-Hall was negative, Hibb’s test was negative bilaterally, Yoeman’s test was negative bilaterally, right pelvic translation was reduced, left head flexion reduced as well, all cervical ROM was improved to normal, cervical flexor strengths were 5/5, left cervical rotators were 5/5, right hip flexor was 5/5, dermatomes of right C5, C6, C7 and C8 were improved to normal using pinwheel sensation. The NDI score was 24% and the HDI was 40%. The SF-36 was not given. She had performed 15 in-office treatment sessions. She statedthat she had been diligent with the daily home routine.
Following her 36th treatment session, she was reassessed. She reported her neck pain to have improved by 90%, her headaches with dizziness and nausea resolved but still had occasional mild headaches, her low back pain improved 70%, the numbness in her feet and legs as well as her upper back pain had fully resolved. She also reported that her cold fingers, tinnitus, and restless legs had fully resolved, her cramping and irregular Periods had resolved, while the difficulty to digesting greasy foods, her low energy, and weak pelvic floor had each improved 80%.
Disability questionnaires revealed a score of 10% on the NDI and a score of 4% on the HDI. The SF-36 revealed a significant improvement in all categories with a minimum of 30 points improvement (out of 100) in each category (Table 1).
Upon physical examination, all orthopedic tests were now normal other than the patient reporting minimal but localized pain on maximum bilateral cervical compression. Her grip strength had improved 6 lbs on the right.
Visually, she had improved posture, now having only a high left shoulder (+RxT) and a left head tilt (–RxH). A lateral cervical x-ray showed dramatic improvement in increasing lordosis (C2-C7 ARA: -24° vs. -11.2°), the forward head position was slightly increased (TzH: +7.4mm vs. +2.4mm), but still WNL, the APL increased to -35.7°. The C2-C3 segmental angle was reduced from +9.0° to +1.5°, not yet normal but improved by 7.5°. Again, she reported to have continued to perform her daily home prescribed routine.
On March 4, 2017, approximately 13 months after the initial assessment, a follow-up assessment was performed. The patient had just given birth two weeks prior; there were no significant exam findings associated with her recent childbirth other than her increased weight. She reported feeling well and rated her pain levels in her neck and low back to be a 1/10 on average and scored a 10% on the HDI and a 6% on the NDI. Her SF-36 scores (Table 1) were at or improved (4 attributes) as compared to her last results (May 20, 2016) and overall each of the 8 attributes scored greater than the normative data indicating she was healthy in all of them.
Physical examination indicated that all ROM for cervical and lumbar areas were WNL and all orthopedic tests were negative. A lateral cervical radiograph (Fig. 1) indicated her alignment values had regressed slightly with only 8 treatments over that timespan. The cervical C2-C7 ARA was -18°, the +TzH was 11.6mm, the APL was -34.3°, and the RRA between C2-C3 was +6.5°. She confessed to only being casually compliant with her home exercises and neck traction (approx. 3x/week) throughout her pregnancy.
DISCUSSION
This report documents the successful outcome in a 29-year old patient with LWS, including chronic headaches and neck pain, 13-years following an MVC. Use of CBP technique protocol increased the overall lordosis and reduced the excessive kyphosis between C2-C3, restoring the cervical alignment closer to normal/ideal.22–25
Oakley and Harrison9 propose that symptoms persisting following those experiencing LWS and having a cervical hypolordosis/kyphosis may have a direct relationship. The MVC causes the whiplash, the whiplash causes the kyphosis,8 and the persisting kyphosis will contribute to persistent symptoms.2 To break this chain, one needs to restore the physiologic lordosis. We feel that our patient’s initial presenting cervical alignment was in an upper kyphosis position due to the previous whiplash experienced years prior, since this is a typical traumatic spinal buckling pattern induced during whiplash.8
The structural correction of cervical lordosis is an emerging evidence-based practice within surgery and manual therapies. Contemporary cervical spine surgical approaches attempt to preserve and/or re-establish the cervical lordosis29,30 for superior patient outcomes, in terms of both the avoidance of neurologic symptoms,31,32 as well as preventing adjacent segmental spinal disk disease.33,34
Advances in CBP technique involving cervical extension traction methods have demonstrated consistency in the non-surgical structural re-establishment of cervical lordosis in symptomatic patients in several clinical trials.26–28,35–38 CBP is a full-spine and posture rehabilitation approach to correct poor posture and deviation of normal spinal alignment through incorporating mirror image® exercises, spinal adjustments, and traction procedures.11–13
These trials26–28,35–38 have demonstrated that in 30-60 treatments over 2.5-3.5 months, an improvement of up to 18° in cervical lordosis may be achieved. All these trials were multimodal rehabilitation programs aimed at improving the cervical lordosis using cervical extension traction methods as well as other manual procedures. Theoretically, as outlined by Oakley et al.12 and clinically demonstrated in the case by Ferrantelli,10 treatment of this nature may continue until the desired magnitude of cervical lordosis is re-established.
The fact that the long-term follow-up showing our patient was quite well despite having the cervical spine alignment values slightly regress, may indicate there may be a threshold of tolerance for the body. In other words, if there is more regression of these values, her symptoms may again escalate toward her initial symptomatic pain scores. It would be prudent now that she gave birth to treat her more frequently to provide more correction to the cervical spine, since she only received 9 treatments over the 9.5 months following her initial intensive 15 weeks, where she received 36 treatments. That provided the initial correction to her posture. Also, the fact that she was pregnant between her 2 last assessments (5/20/16 - 3/4/17) may indicate that during pregnancy, due to hormones, the spine may have become looser and this may have resulted in the slight regression of her cervical posture, although the overall alignment still remained significantly better than how she initially came in (1/29/16).
The findings resulting from the treatment in this case are obviously limited by the fact it is only a single case. Another limitation is that multiple treatments were given to the patient. Exercise39 as well as manipulation to the spine,40–42 however, has not been proven to routinely correct structural spine alignment, and is most likely due to the extension orientation of the cervical traction that causes ligamentous creep deformation.43
CONCLUSION
Our case suggests that correcting cervical lordosis by Chiropractic BioPhysics methods, in those with late whiplash syndrome and cervical kyphosis, may alleviate the symptoms typically experienced by those suffering from previous whiplash.