INTRODUCTION
Vocal cord palsy as the result of recurrent laryngeal nerve involvement is described in the literature in concert with mediastinal diseases. This may include, but is not limited to, a variety of neoplastic, inflammatory, and vascular condition.1 The most common cause of VCP as a result of recurrent laryngeal nerve compression is malignant tumors.2 However, dysfunction of the vocal cords have also been described secondary to endotracheal intubation.3
Interscalene blocks and general anesthesia are indicated for use during shoulder surgery.4 Although considered safe and effective, these anesthesia techniques are not free of complications. Specifically, supraglottic airway devices need to be used to help manage airway obstruction in patients undergoing general anesthesia. These devices are generally regarded as safe; however, some complications associated with their use have been described.5 Recurrent laryngeal nerve (RLN) injury is the most common traumatic neurolaryngological lesion.6 Acute injury to the RLN may lead to vocal cord paralysis (VCP) of the ipsilateral side, severe dysphonia to complete paralytic aphonia, and aspiration of food and drink into the trachea.6 Recurrent laryngeal nerve (RLN) injury [without injury to the superior laryngeal nerve (SLN)] is the most common traumatic neurolaryngological lesion. The acute effects are immediate flaccidity of the ipsilateral vocal fold, loss of abduction and adduction, severe dysphonia to complete paralytic aphonia, and, frequently, aspiration of food and drink into the trachea. This article reviews the function of the four intrinsic laryngeal muscles innervated by the RLN and the individual effects of RLN transection on these muscles. Following acute denervation, the subsequent progression is either chronic denervation or nerve regeneration with laryngeal muscle reinnervation. Four possible scenarios are discussed here: complete reinnervation with synkinesis, partial reinnervation with synkinesis, mixed RLN injuries, and no reinnervation (complete paralysis). Electromyography may eventually assist the laryngologist in establishing these diagnoses, but currently not enough normative data exist for confirming laryngeal synkinesis unequivocally in every case. Treatment is generally by Teflon injection, medialization thyroplasty, arytenoid adduction procedures, or reinnervation by nerve transfer. The author’s preference is nerve transfer, insofar as the quality of resultant phonatory voice, in his hands, has been superior to the other techniques.VCP is a common symptom for a number of diseases; it may also be due to neurogenic or mechanical fixation of the cords themselves.7 The most common cause of VCP as a result of recurrent laryngeal nerve compression is malignant tumors.2 The functional capabilities of the vocal cords include the ability to breathe, swallow, and phonate effectively. VCP may also be asymptomatic, in up to 40% of individuals.8 After diagnosis of VCP, the clinician should thoroughly examine the larynx and hypopharynx in addition to the structures around the course of the ipsilateral RLN. An RLN can be paralyzed anywhere along its pathway, from the brainstem to the inferior margin of the nerve. The right RLN extends below the brachiocephalic artery, whereas the left RLN travels through the aorticopulmonary window.4
This case report discusses a case of aphonia that developed after arthroscopic shoulder surgery for a torn rotator cuff tendon. Beach-chair patient positioning was used during the surgical process. Sedation included an interscalene block and general anesthesia. A tracheal tube was used to control the airway. This case also examines how the diagnosis of a RLN entrapment/compression may present and describes the treatment process used to restore proper vocal cord function and phonation.
CASE REPORT
A 55-year-old female had arthroscopic surgery to repair a right torn rotator cuff. During surgery she had general anesthesia and an interscalene block on the right side. The surgery lasted for 1 hour, and during it she was placed in the beach-chair surgical position. Following surgery, she awoke being very hoarse and what she described as “airy.” She indicated that it took a lot of air to create a sound. She requested ice chips to chew on and immediately started aspirating them. At that time, the medical team informed her that this was probably from the interscalene block and that the symptoms would eventually subside. She was in the post-anesthesia care unit (PACU) for about an hour after surgery and then moved to the hospital floor. The aspirations continued to worsen. In addition, she was having difficulty with phonation and struggling to consume liquids. Furthermore, she recalled having a very low post-surgical blood pressure (90/60 mm/HG) and heart rate (40bpm) after surgery. She indicated that this was much lower than normal. She was eventually discharged that same day with normal blood pressure and a heart rate of 55bpm; however, she still could not talk and continued aspirating.
The following morning, she awoke and took her first pain pill, which did enter the esophagus, though she aspirated the water. Her symptoms remained and a week later she was evaluated by an ENT medical doctor. He performed a flexible laryngoscopy with videostroboscopy. She was diagnosed with a left true vocal cord paralysis as a result of a left laryngeal nerve compression injury, possibly due to inflation of the intubation tube during surgery. However, there was no inflammation of the trachea from the intubation tube. Typically, tracheal edema and inflammation would be a normal result of a compression-like injury. That same day, she underwent a procedure for a collagen (Cymetra®) injection into her left vocal cord. The injection gave immediate relief for swallowing; however, it took 3 weeks for her to be able to generate any sort of sound distinguishable as a speaking voice.
Five weeks after surgery she had a follow-up appointment with the ENT. There was some vibration in her left vocal cord; however, she was told she still did not have any left vocal cord function. The ENT did inform her that she should not have any difficulty swallowing. However, she indicated that she was still experiencing periodic aspiration. There was no edema or any other signs of trauma to the trachea present.
Seven weeks after surgery she then came to our chiropractic clinic, having been referred by her physical therapist for evaluation and possible treatment of her vocal cord paralysis. Prior to that visit, the referring physical therapist consulted with us regarding her case. A possible working diagnosis was suggested that the patient had a recurrent laryngeal nerve entrapment as opposed to compression, thus leading to her vocal cord paralysis. At her initial chiropractic appointment, subjective findings included continued complaints associated with vocal cord paralysis. These included aspiration, difficulty with phonation, and hoarseness.
She was in no acute or apparent distress and was well nourished and well developed, standing 66" and weighing 130lbs. She did not have an antalgic gait. Her BP was 110/74, and her pulse was 62bpm. There were no neurological deficits detected in her upper and lower extremities. Right lateral bend of her cervical spine caused a pinching pain in the right side of her cervical spine, and right rotation caused pain in the insertion of the right levator scapulae. Left shoulder depression test also caused a pinching pain in the right side of her cervical spine. She had tenderness to palpation at C3 and along the left costovertebral joint of T1/first rib. There was reduced segmental motion at C3 and T1/first rib. Muscle spasm was palpated along the left side of her neck at the suboccipital muscles, posterior belly of the digastric muscle, sternocleidomastoid (SCM), anterior scalene and subclavius. Additionally, the posterior belly of the digastric muscle was also tender to palpation and she noticed tension in this muscle when trying to stretch it.
There was significant tight and tender musculature over the region that the left recurrent laryngeal nerve primarily courses at the digastric muscle, C3 segmental dysfunction, as well as a lack of tracheal edema and inflammation. This led to a working diagnosis of left RLN entrapment by the left posterior belly of the digastric muscle. Chiropractic care could was initiated to address myofascial and musculoskeletal dysfunction along the course of the left RLN. The treatment consisted of chiropractic manipulation, instrument-assisted soft-tissue mobilization, manual therapy, therapeutic ultrasound, and stretching exercises that the patient was to perform at home. High-velocity low-amplitude manipulation was directed at the segmental dysfunctions at C3 and T1/first rib. The instrument-assisted soft-tissue mobilization (IASTM) was performed using Graston instruments. The instruments were used along the myofascial regions overlying the course of the left RLN. The aim of this was to reduce any myofascial restrictions noted there. For the manual therapy, we first had the patient actively shorten the specific muscle being treated We applied a manual compression with the doctor’s hand, following the patient actively lengthening that specific muscle. Again, the aim of this was to reduce muscular spasm and myofascial restriction. Lastly, the at-home stretching exercises were for the left digastric muscle, bilateral suboccipital muscles, left sternocleidomastoid (SCM), left anterior scalene and left subclavius. She was told to stretch each muscle 3-5xday holding each stretch for at least 30 seconds. The posterior belly of the digastric muscle can easily be stretched if an individual puts his or her cervical spine into a protruded position, to also include mandible protrusion as if perorming an under-bite. Then to stretch a specific side, such as the left posterior belly of the digastric muscles, gently turn the head to the right while holding the cervical and mandible protrusion.
During the course of her care, 10 treatments were given over the course of 2.5 months. Treatment was initiated at 2x/week, then tapered to 1x/week and eventually tapered to once every 3-4 weeks. At her last visit, she reported that she was doing well and was discharged from active care. This fell over the holiday season and she later told us that no family member noticed a difference or change in her voice. She was no longer aspirating, even with thin liquids, and was back to singing, her passion. Her vocals were no longer raspy or hoarse. She felt her singing voice had more range and reported that she now only struggled with the middle octave but could hit her high and low notes. Finally, she indicated that she was still doing her digastric muscle stretch but felt that there was nothing left to stretch. At her last examination, we noted only very mild tightness in her left digastric, subclavius, SCM and anterior scalene muscles. The C3 segmental dysfunction was absent and only a mild T1/first rib segmental dysfunction existed. The musculoskeletal components were addressed, and we agreed that she would come in only as needed.
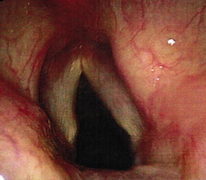
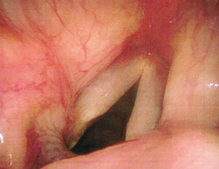
Approximately 7 months after her initial visit with the ENT, she had a follow-up appointment. Laryngoscopy with videostroboscopy was performed and the findings demonstrated complete return of function to her left vocal cord, with both cords working in tandem. (Figures 1 and 2) There was no physical evidence that she ever had an issue and was given a 100% return to function diagnosis.


DISCUSSION
CT imaging will not directly allow the clinician to visualize the Vagus nerves or RLNs. Therefore, it is important for clinicians to know the expected courses diagnosing RLN pathology. The RLN is clustered within the Vagus nerve as it exits the nucleus ambiguous in the medulla of the brainstem. The Vagus crosses the lateral cerbellomedullary cistern and exits the base of the skull through the pars vascularis of the jugular foramen. It is located within the dural sheath shared with the spinal accessory nerve.9 The superior ganglion of the Vagus nerve is situated within the jugular foramen and houses the vagal parasympathetic and sympathetic cell bodies. It is not directly involved in skeletal muscle control. Conversely, the inferior ganglion, which is right below the jugular foramen, is the site of departure for the pharyngeal branches and the superior laryngeal nerve, both of which provide muscular innervation. The pharyngeal divisions provide motor fibers to the pharyngeal plexus. These supply the pharyngeal muscles and palate, including the uvula.10 The pharyngeal plexus is also the home to sensory branches of the glossopharyngeal nerve and vasomotor sympathetic fibers from the superior cervical ganglion. The superior laryngeal nerve provides motor fibers to the cricothyroid and superior pharyngeal constrictor muscles.11 Extracranially, the Vagus nerve, still carrying the RLN, descends through the neck posterolateral to the internal carotid arteries within the carotid sheath and is located posteromedial to the adjacent jugular vein.
On the right, the vagus nerve descends with the carotid artery sheath into the upper mediastinum. The right RLN exits from the vagus nerve anterior to the subclavian artery and courses posteriorly under the artery at the level of the brachiocephalic bifurcation. It has a short mediastinal course, traversing obliquely toward the right tracheoesophageal groove over the surface of the apical parietal pleura.12
The course of the left Vagus nerve descends with the carotid artery sheath into the mediastinum before descending anterolateral to the thoracic aorta. The left RLN exits the vagus nerve at the level of the Aortic Arch, then passes posteromedial beneath it. This then traverses through the aorticopulmonary window posterior to the ligamentum arteriosum. At that time it ascends vertically through the superior mediastinum to reach the tracheoesophageal groove.12 The RLNs enter the larynx just behind the cricoarytenoid joints and give the intrinsic laryngeal muscles their nerve innervation. The cricothyroid muscle is the only intrinsic laryngeal muscle not supplied by the RLN, with the motor function directly from the superior laryngeal branch of the Vagus nerve.13 The posterior cricoarytenoid muscle is the main vocal cord abductor and is innervated from the ipsilateral RLN. Paralysis of the posterior cricoarytenoid results in anteromedial subluxation of the arytenoid cartilage. This results in medicalization of the posterior aspect of the vocal cord. This is responsible for many of the CT signs of VCP. During normal respiration, this is the only intrinsic laryngeal muscle capable of separating the vocal cords. Thus paralysis leads to the inability to abduct the vocal cords on the ipsilateral sides.3
The incidence of postintubation vocal cord paralysis is thought to be around 10-15% of all vocal cord paralysis.3 A retrospective review revealed that intubation injuries accounted for 15% of all bilateral vocal cord immobility and 7.5% of unilateral immobility.14 However, this study did not differentiate between recurrent laryngeal nerve paralysis and cricoarytenoid fixation.14 Another review estimates that 10-15% of all cases of vocal cord paralysis occur after endotracheal intubation.15 The RLN is particularly susceptible to injury during surgical procedures. Thyroidectomies, carotid endarterectomies, and anterior surgical approaches to the cervical spine are all common iatrogenic causes of VCP.16 The RLN is also prone to injury secondary to central venous catheter placement and median sternotomy due to its more lateral placement and oblique course. Upper lobectomies and cardiac surgery also place the RLN at risk of injury.17
The current mechanisms for immobile vocal cord after intubation are either due to mechanical injury by dislocation or subluxation of arytenoid joints or direct nerve injury.18 Our case was void of dislocation or subluxation or arytenoid joints. The anterior ramus of the recurrent laryngeal nerve is vulnerable to compression between the thyroid cartilage and endotracheal tube cuff about 6-10mm below the cords.19,20 The increase in cuff pressure compresses the vasa nervosus, leading to ischemic injury of this branch. The involvement of the anterior ramus of the RLN, which most often supplies the adductors of the cords, accounts for the cords being fixed in a paramedian position. However, there is a wide variation in the distribution of the anterior and posterior branches of the RLN. Other suggested mechanisms causing RLN injury during endotracheal intubation are hyperextension during intubation and movement of the endotracheal tube through the cords during intubation, which compresses the nerve.18,21 As noted here, there was no damage during the trans-nasal scope, possibly eliminating mechanical injury. Additionally, the patient was not diagnosed with arytenoid cartilage dislocation or subluxation.
Other mechanisms also need to be considered for potential causes of VCP. Arthroscopic shoulder surgeries are typically done in 1 of 2 positions, either the beach-chair position of the lateral decubitus position. While the lateral decubitus position has been linked to the potential of peripheral neuropraxia, brachial plexopathy, direct nerve injury, and airway compromise, the beach-chair position has been associated with cervical neuropraxia, pneumothorax, and the potential for end-organ hypoperfusion injuries.22 There are increased anesthesia concerns with the patient in the upright beach-chair position. This is because the sympathetic nervous system is responsible for increasing vascular resistance and mean arterial pressure (MAP), while reducing cardiac output to maintain cerebral perfusion. Under general anesthesia, there is more difficulty responding or compensating for this.23 The beach-chair position may also lead to cerebral hypoperfusion, which is recognized and a catastrophic complication.24 Cervical hyperextension and rotation and lateral bend can decrease vertebral artery flow, resulting in infarcts in the distribution of the posterior cerebral artery.24 Furthermore, Park and Kim documented a case series of neurapraxia hypothesized to have been caused by malposition of the head and neck in the beach chair position resulting in excess pressure on superficial nerves.25 They reported neurapraxia of the lesser occipital nerve in 1 case and neurapraxia of the greater auricular nerve in another case. Both of those nerves are superficial and vulnerable due to their anatomic location. The possible cause of palsy was from compression resulting directly from change and rotation of the head and neck during surgery.
Although there literature demonstrating neurapraxia involving the RLN from the beach-chair position, Mullins et al. did report a case of hypoglossal nerve palsy after arthroscopy of the shoulder and open repair of the rotator cuff performed with the patient in the beach-chair position.26 Although the true cause of this palsy was not confirmed, an alteration in the neck position during the surgery may have allowed the nerve to become compressed beneath the angle of the mandible.22 Two additional cases of hypoglossal nerve palsy were reported after a change in trunk position converting from an arthroscopic to an open procedure in the beach-chair position.27 Due to the close proximity of the hypoglossal nerve and the RLN behind the angle of the mandible, it is possible that compression here could lead to compression on not only the hypoglossal nerve, but also the RLN and the Vagus nerve. Our patient also had spasms in her left digastric muscle, which is at the angle of the jaw.
Considering the decrease in blood pressure after the patient’s surgery, it is a possibility that the Vagus nerve may have been irritated during the surgical process as well. Anatomically, this entire case study might be that of a Vagal nerve entrapment or compression injury verses a RLN entrapment. However, as previously mentioned, there are anesthesia concerns when patients are in the beach-chair position and this could have led to the drop in her blood pressure.18 Regardless of the exact cause of the drop in blood pressure, it should be noted that the RLN is grouped within the Vagus nerve until it branches off. Diagnostically, if CT imaging for VCP did not show a causative lesion, making the distinction between a proximal vagal neuropathy and a RLN neuropathy in isolation is important for directing further management and imaging. This can be attempted by observing the effect of the pharyngeal constrictor muscles and uvula. Both structures are innervated by the pharyngeal plexus. Paralysis of the proximal portion of the vagus nerve can affect both the pharyngeal motor branches and the RLN. Therefore, in addition to findings of VCP, proximal involvement can manifest on CT as dilation of the ipsilateral orophyarnx, thinning of the pharyngeal constrictor muscles and uvular deviation away from the side of causative lesion.25 Unfortunately, throughout the course of care we did not observe the effect the pharyngeal constrictor muscles had on the uvula nor did our patient have a CT.
In regards to the resolution of symptoms, post-intubation recurrent laryngeal nerve paralysis (RLNP) is known to have a favorable prognosis.1 In fact, Yamada et al reported recovery of vocal fold mobility in 13 of 19 patients, or 68.4%.28 However RLNP of unknown caused has a less favorable prognosis with recovery rates of 29.5% (18 of 61 patients).29 Furthermore, Yamada et al also documented that vocal fold movement recovered completely in 6.4% (36 of 564 patients) with RLNP of various causes who were followed up over 6 months after onset.28 Kawamura et al. reported that 33.3% (37 of 111 patients) who were followed over 6 months after onset showed a certain degree of improvement in vocal fold movement within 3 months.29 Never-the-less, the rest of the patients with unilateral RLNP require appropriate treatment for hoarseness.
Limitations
There are several limitations possible. First, the treating clinician arrived at a working diagnosis of a left recurrent laryngeal nerve entrapment vs. a compression injury, thus treating the surrounding anatomy that would likely entrap the left RLN. The left-sided vocal cord paralysis could in fact have been a RLN compression injury and resolved over the course of time. However, it is still possible that if the injury was a true compression injury, inflammation of the left RLN would also manifest as an entrapment. Second, the patient underwent a collagen injection into her left vocal cords. It is unknown if the collagen injection or the provided treatment by us led to her response to care. Finally, the results could be due to the normal course of this condition.
CONCLUSION
Vocal cord palsy following intubation is a described condition but also thought to be a very preventable complication. Attention to technique is of utmost importance. However, there is a possibility that vocal cord palsy might not be due to a true RLN compression, rather a RLN entrapment. This entrapment could be manifested by the duration and position of the patient’s head and neck during her surgery, possibly placing tension through the lateral cervical paramusculature. Regardless, the importance of this case suggests plausible treatment to the entrapment site(s) of the RLN to help resolve vocal cord paralysis. More studies are needed to demonstrate effectiveness of treatment.