
INTRODUCTION
There are increasing occurrences in institutions of higher learning where students attribute lower academic performance to mental issues like anxiety and depression. Traditionally, major depressive disorder is viewed as an illness in which depressive episodes are followed by periods of euthymic mood.1 Approximately 1 in 5 people will experience a major depressive episode at some point in their lives.2 A gene or a combination of genes that cause depression have not been identified by scientists. Patients with derpression show persistent neurobiological abnormalities.
Structural neuroimaging studies show that individuals with major depressive disorder may have relatively small hippocampi even while in remission.1 Patients may also present with volumetric abnormalities in other subcortical brain regions. These include the amygdala and ventral striatum, and in cortical regions, including the anterior cingulate cortex, orbitofrontal cortex and prefrontal cortex.1 However, stress is a commonly known precipitating factor for depression.2
Depressed individuals show poor memory for positive elements, potentiated memory for negative events, and impaired recollection. Even though these phenomena are poorly understood, they are clinically important. Stress can suppress hippocampal neurogenesis, inhibit dopamine neurons, and sensitize the amygdala.3 Dillion and Pizzagalli argue that these phenomena may impair pattern separation, disrupt the encoding of positive experiences, and bias retrieval toward negative events respectively, thus recapitulating core aspects of memory disruption in depression.3
Encouragingly, they also note that optogenetic reactivation of cells engaged during the encoding of positive memories rapidly reduces depressive behavior in preclinical models. Thus, many memory deficits in depression appear to be downstream consequences of chronic stress and addressing memory disruption can have therapeutic value.3
Aim of Review
This review aims to:
-
Analyze and summarize the correlation between anxiety, depression, and memory— a major component in academic performance.
-
Investigate the etiology of stress and depression.
-
Review consistent pathophysiological and neurobiological findings on the effect of depression and anxiety on memory and overall learning.
METHODS
Electronic databases were searched in April 2019 for relevant published research. Other publications were extracted in the early weeks of May 2019. We searched MEDLINE, Scopus, ISI Web of Knowledge, (Web of Science) PubMed, Google Scholar, and PsychINFO using keywords anxiety, stress, depression, learning, academic performance, amygdala, neurobiological, neurogenesis, hippocampus, and monoamines for 1997-2018. Conference proceedings, relevant journals and papers were hand-searched as well (Trends in Neurosciences, Annual Review of Psychology, Reviews in the Neurosciences, Journal of Psychiatric Research, International Journal of Clinical Practice) in consultation with college librarians.
All papers that had potentially relevant information in their title and or abstract were obtained. Additional publications were extracted from reference lists.
Inclusion criteria were that the study examined the neurobiological effects of anxiety and or depression on academic learning and performance; the study had at least 1 outcome measure relating to the effects of anxiety and or depression on learning, memory, retention of knowledge, acquisition, retrieval; and, the study included students enrolled in higher institutions of learning.
The exclusion criteria were that the study did not report the effect of anxiety and or depression on learning; the study sample was on elementary school learners, middle school aged children, or the aging population; and the study focused on current trends, rise, and treatment of depression.
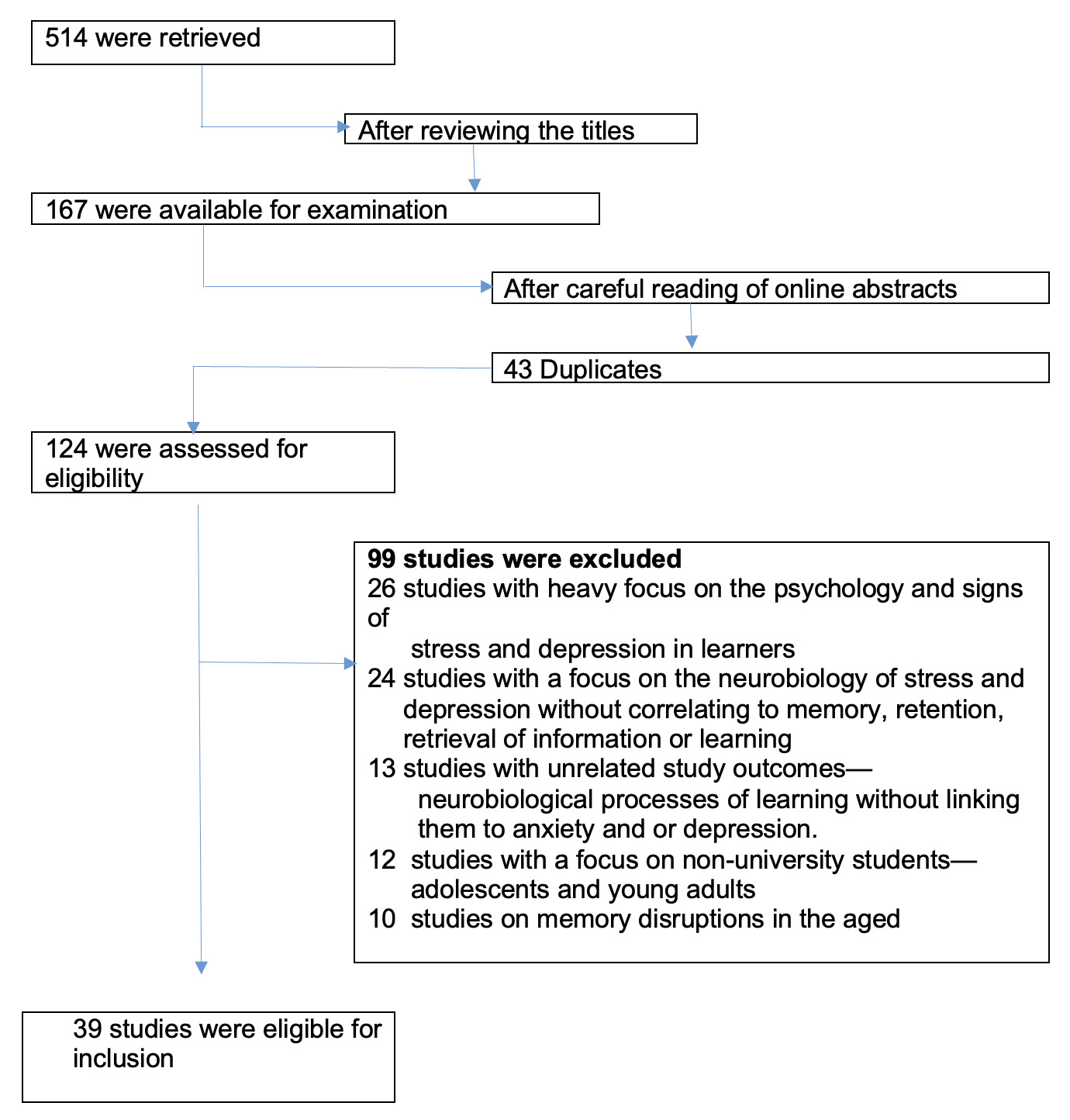
Our search yielded 514 citations. However, after examining the titles, abstracts (for studies whose abstracts were available) and reference lists for the related articles, 167 were retrieved for examination. 43 were found to be duplicates.
After reading the articles carefully and thoroughly, an additional 99 articles were excluded because the studies had a heavy focus on the psychology and signs of stress and depression in learners (26 studies), studies had a focus on the neurobiology of stress and depression without correlating to memory, retention, retrieval of information or learning (24 studies), studies had unrelated study outcomes— neurobiological processes of learning without linking them to anxiety and or depression (13 studies), studies had a focus on non-university students— adolescents and young adults (12 studies), or the studies looked at memory disruptions in the aged (10 studides).
Findings included were regarded as important and significant because they were confirmed by several studies where different methodological approaches were implemented.
The remaining 39 articles were included and evaluated for quality. (Figure 1)
DISCUSSION
1. Analysis and summary of the correlation between anxiety, depression, and memory— a major component in academic performance.
This section of the review aims to identify the neurobiological mechanisms that have arisen to explain the concept.
General Overview of Anxiety and Depression
This section of the review aims to define terms and to create an understanding of anxiety and depression.
The American Psychological Association (APA) defines anxiety as an emotion characterized by feelings of tension, worried thoughts and physical changes like increased blood pressure.4
Anxiety disorders include disorders that exhibit features of excessive fear and anxiety. They include related behavioral disturbances like panic attack. Anxiety disorders put an individual in a state of fear—the emotional response to real or perceived threat and anxiety—the anticipation of future threat.
Anxiety disorders differ from one another in the types of objects or situations that induce fear, anxiety, or avoidance behavior, and the associated cognitive ideation. Under this category, we have separation anxiety, selective mutism, specific phobia, social anxiety disorder (social phobia), panic disorder, agoraphobia, generalized anxiety disorder, and substance/medication-induced anxiety disorder.4
A major depressive episode is characterized by a low mood or an inability to experience pleasure (anhedonia), or both, for more than 2 weeks, combined with several cognitive and vegetative symptoms and the occurrence of distress or impairment. A diagnosis of major depressive disorder can be made if a person suffers at least 1 such episode (without ever experiencing mania). However, most people with major depressive disorder have multiple episodes.1
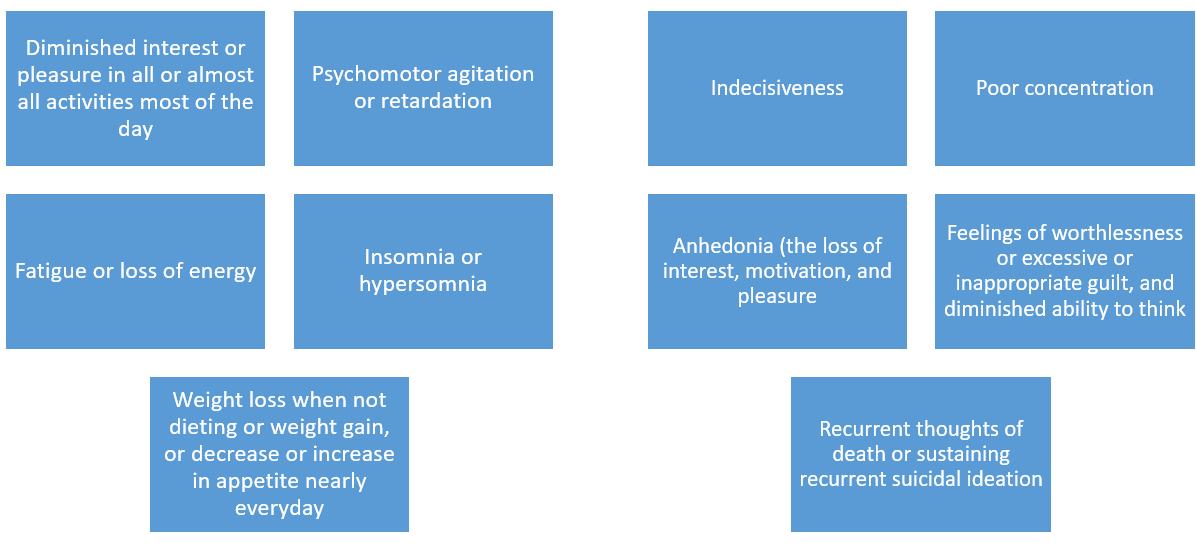
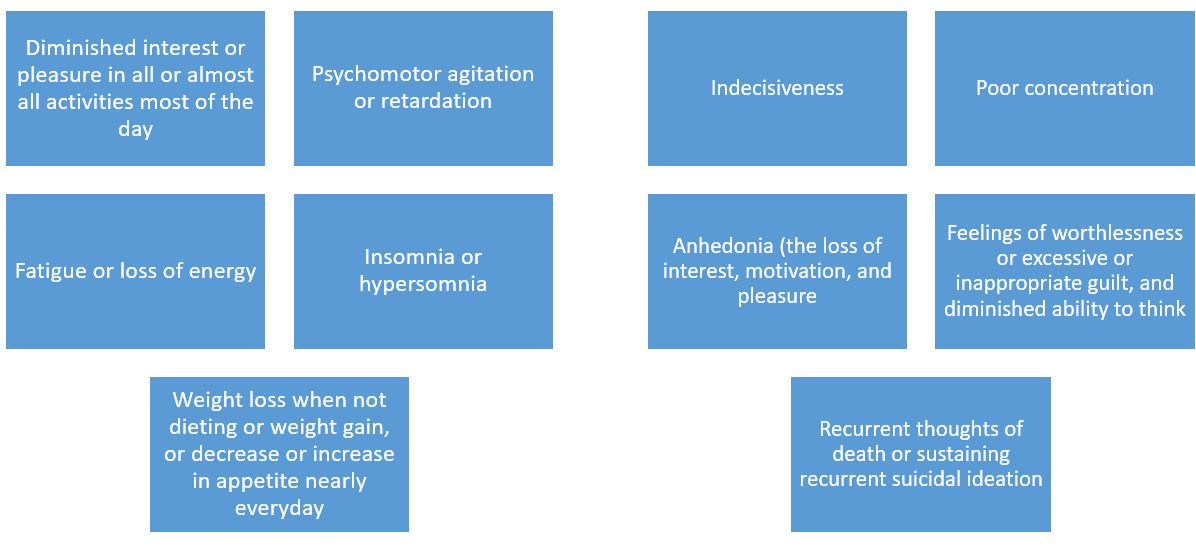
What signs and symptoms can you expect in a student who is battling depression?
Depression4 is evidenced through those factors listed in Figure 2.
Academic Learning here refers to the acquisition of knowledge, skills, values, and behaviors that improve and shape a learner. It is the ability to engage cognitive functions for the acquisition, use, retention, storage, transformation, and retrieval of information to improve performance at different levels. Academic Performance refers to the measurable achievements for students in various categories (Google) as evidenced by their Grade Point Average (GPA), national examinations, and graduation rates.
Correlating Neurobiological Mechanisms
Khakpai and Zarrindast defined anxiety as that unpleasant physiological state in which an overreaction to a situation occurs. They noted that different brain regions are involved in the modulation and expression of anxiety, including the amygdala, the hippocampus, and frontal cortex.5
Contrarily, multiple sources of evidence support a role for diminished dopaminergic neurotransmission in major depression. The physiological alterations underlying reduced dopamine (DA) signaling could result from either diminished DA release from presynaptic neurons or impaired signal transduction, either due to changes in receptor number or function and/or altered intracellular signal processing.6
2. Etiology of stress and depression
Exactly what do individuals with anxiety and depression experience that can affect their academic performance?
There is evidence of excessive amount of brain activity that results from fear and the fight or flight response. Such increased activity can cause the sympathetic nervous system (SNS) to increase. Increased sympathetic activity can cause the amygdala to work overtime. This also leads to fear. When the amygdala, the part of the brain that gets involved in the SNS, is unable to stop firing, obvious physical signs become evident. These include increased heart rate, increased blood pressure, tense muscles, sweaty palms, and dizziness. Memories can trigger this part of the brain causing it to fire too much as well.7–9
Depressed individuals typically show poor memory for positive events, potentiated memory for negative events, and impaired recollection.3
Kastner et al found that focusing attention at a particular location had the power to change brain baseline activity levels in different regions of the human visual cortex without the introduction of a stimulus.10
Our perception derives from the interaction between incoming sensory stimulation and endogenous factors linked to task goals, expectations, and memories. Selective attention comprises the functions that prioritize and select relevant information from the incoming sensory stream based on these endogenous signals and, thus, is an essential building block of cognition.11 Modern studies in neurology now point us away from the long-standing notions that long sustainable signals were required to pre-activate neurons based on receptive fields matching spatial locations. Instead, now we know that anticipatory controls are adaptive, dynamic and even flexible. The signals are therefore not plain passive reproductions of memory matrixes. The signals are active elements with a high potential to promote adaptive behavior.11
These great phenomena are of common public interest and at the heart of those seeking to understand the impact of mental disorders on different aspects of life. Clinically important as they are, they are still vaguely understood.
The key question still remains, how do these phenomena correlate to learning and academic performance?
Attempting to answer this question, I investigated different supporting theories as discussed below.
Mechanisms of Memory Disruption in Depression and Anxiety
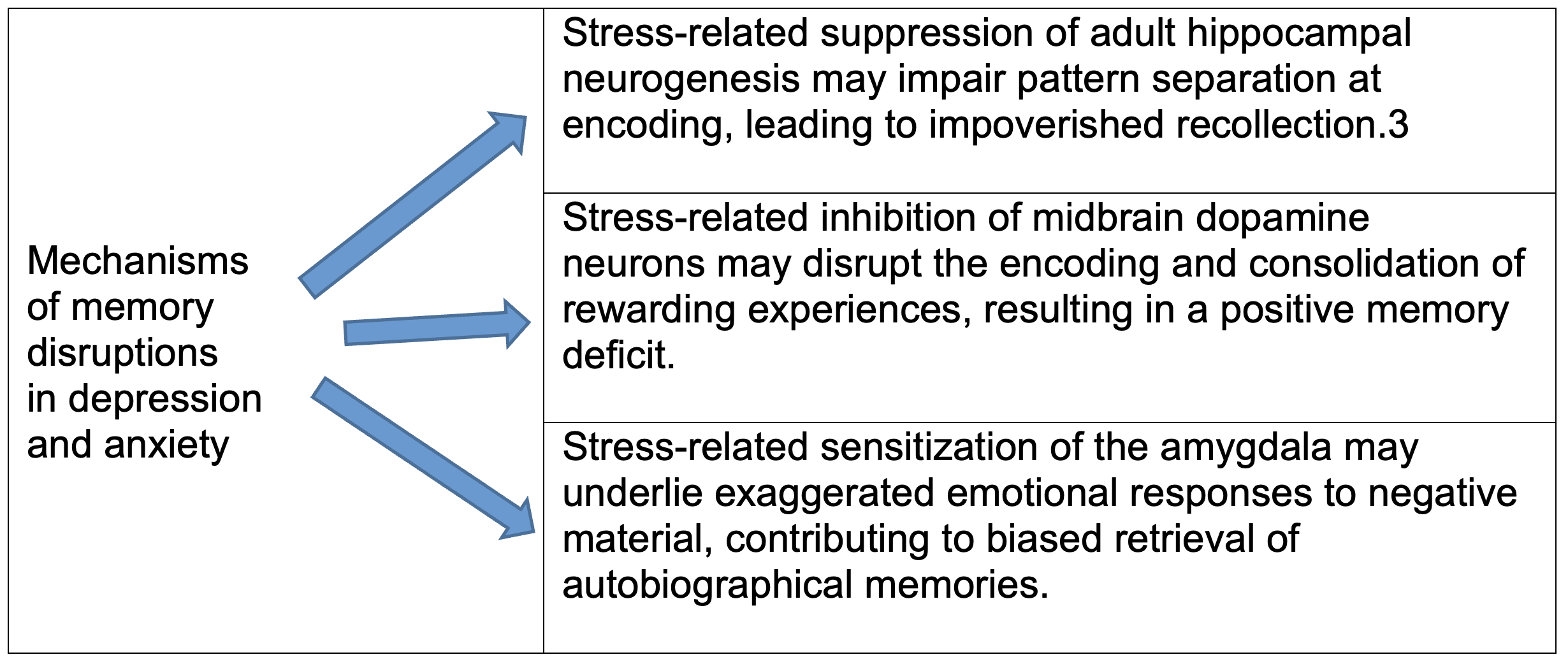
Studies show that stress can suppress hippocampal neurogenesis, inhibit dopamine neurons, and sensitize the amygdala. Dillon and Pizzagalli argue that these phenomena may impair pattern separation, disrupt the encoding of positive experiences, and bias retrieval toward negative events, respectively, thus recapitulating core aspects of memory disruption in depression. However, they encouragingly see that, optogenetic reactivation of cells engaged during the encoding of positive memories rapidly reduces depressive behavior in preclinical models. Thus, many memory deficits in depression appear to be downstream consequences of chronic stress and addressing memory disruption can have therapeutic value.3
Stress can trigger depressive episodes in humans and chronic stress elicits depressive phenotypes, including memory impairments. While focusing on the link between specific consequences of chronic stress and particular aspects of memory disruptions in depression, they proposed the important findings seen in the table below (Figure 3). They saw that the hippocampal neruogenesis was suppressed in depression, and that suppression was ameliorated by antidepressants.3

Even though depression is a heterogeneous disorder that encompasses several pathophysiologies and is not easy to single out specific mechanisms of its cause, the reduced hippocampal volume in individuals suffering from depression has become a reliable structural finding in psychiatric imaging. Meta-analysis shows a 4-10% bilateral reduction.12–14
There is evidence suggesting that major life stress, in addition to precipitating depression, can lead to structural remodeling of the hippocampus via activation of glucocorticoid receptors, which are abundant in this brain region.15 There are MRI studies which indicate that the number of prior major depressive episodes are inversely correlated with hippocampal volume and reduced stress perception.16
Effect of Depression on Memory and Performance
Kizilbash et al reported that depressive symptoms (without anxiety) had an adverse effect on immediate recall of new information and the total amount (but not rate) of acquisition; however, retrieval and retention were unaffected.17 Conversely, high levels of anxiety did not have significant detrimental effects on any aspect of memory functioning assessed including immediate recall, total amount acquired, retention, and retrieval of novel information. However, when depression was compounded by anxiety, there was not only an adverse effect on immediate recall and amount (but not rate) of acquisition, but also on the retrieval of newly learned information. They concluded that the presence of comorbid anxiety may, in part, account for the variability in previous research findings regarding the effects of depression on memory functioning.17
When combined, study findings indicate that when anxiety exists comorbidly with depressive symptoms, there is variability in memory performance evident in depressed individuals. Their cognition remains unaffected. It was hypothesized that the presence of depression or anxiety, individually, would hinder some aspects of memory performance, but that memory deficits would be most apparent in individuals with coexisting symptoms of depression and anxiety.
The results of the same study revealed that depressive symptoms (without anxiety) have an adverse effect on immediate recall of new information and the amount (not rate) of acquisition, but not on retrieval or retention (long delay free recall and recognition hits, respectively). However, symptoms of anxiety (without depression) did not have a significant deleterious effect on any aspect of memory functioning assessed.17
3. Pathophysiological and neurobiological findings on the effect of depression and anxiety on memory and overall learning.
The Implication of the Amygdala
According to Palazidou, (2012) the amygdala is involved in recruiting and coordinating cortical arousal and neuroendocrine response to underdetermined (surprising and ambiguous) stimuli as well as in emotional learning and memory.18 Dillon and Pizzagalli3 have noted that autobiographical memory retrieval in depression is overgeneral. Rather than recalling specific episodes, depressed adults tend to retrieve ‘categorical’ memories – summary accounts that lack defining details. This is noteworthy because overgeneral memory predicts a longer course of illness, possibly reflecting its relationship to impaired executive function and problem-solving deficits. And as already noted, memory in depression is biased toward negative material. The amygdala displays a hyperactive response to negative autobiographical memories in depressed adults, adults in remission, and even adults at high risk of depression. They concluded their study by saying that the relationship between depression and memory is bidirectional: depression affects memory, but memory problems likely exacerbate depression. A bias to repeatedly retrieve painful memories could clearly sustain a depressive episode, and failure to encode and consolidate positive memories could reinforce the anhedonia that (putatively) disrupted those processes in the first place.3
The hippocampus and the amygdala are essential components of the neural circuitry mediating stress responses. The hippocampus, which provides negative feedback regulation of the stress response, is particularly vulnerable to degenerative changes caused by chronic stress. Unlike the hippocampus, relatively little is known about how stress affects the amygdala and the nature of its role in the stress response. Chronic stress can cause contrasting patterns of dendritic remodeling in neurons of the amygdala and hippocampus.3
Multiple sources of evidence support a role for diminished dopaminergic neurotransmission in major depression. The physiological alterations underlying reduced dopamine (DA) signaling could result from either diminished DA release from presynaptic neurons or impaired signal transduction, either due to changes in receptor number or function and/or altered intracellular signal processing.3
In summary, a convergence of findings points to disrupted adult hippocampal neurogenesis in depression as well as links between depressive symptoms and impaired pattern separation for neutral material.
The Mediating Role of Monoamines
Investigations into the neurobiology of major depressive disorder traditionally focused on the monoamine neurotransmitters serotonin and norepinephrine. The monoamine hypothesis initially posited that depressed individuals are likely to have low levels of these neurotransmitters because various antidepressant drugs acutely increase their levels.19
Gregor Hasler, writing on the pathophysiology of depression, noted that most of the serotonergic, noradrenergic and dopaminergic neurons are located in midbrain and brainstem nuclei and project to large areas of the entire brain. This anatomy suggests that monoaminergic systems are involved in the regulation of a broad range of brain functions, including mood, attention, reward processing, sleep, appetite, and cognition. The monoamine-deficiency theory posits that the underlying pathophysiological basis of depression is a depletion of the neurotransmitters serotonin, norepinephrine or dopamine in the central nervous system.20
Conversely, Marije, Sanjav, and Dennis reported that one polymorphism that may moderate the interactive effect of the serotonin transporter polymorphism and psychosocial stress is located in the gene that codes for brain-derived neurotrophic factor. This growth factor plays a major role in the birth, survival and maturation of brain cells during development. Brain-derived growth factor is important for cell growth and for allowing changes in the synapses between neurons (synaptic plasticity) throughout life. Brain-derived neurotrophic factor contributes to these processes primarily by activating DNA-binding factors that stimulate gene transcription.21 Supporting this phenomenon is Martinowich, who noted that during brain development, this cyclic process promotes outgrowth, synapse formation and survival of serotonin neurons, and the eventual innervation of multiple brain regions. The ability of the serotonin system to adapt and change in response to various stimuli continues to be influenced by brain-derived neurotrophic factor throughout life.22
Postmortem studies have found low levels of brain-derived neurotrophic factor in the hippocampus and prefrontal cortex of symptomatic depressed patients.23 Patients with major depressive disorder have low levels of brain-derived neurotrophic factors.24
Foundations recovery network reported that individuals with depression may be unable to complete tasks that require high motor and cognitive skills. They may feel confused, scatterbrained, overwhelmed or easily frustrated. Even basic everyday tasks become difficult. Depression impairs cognitive functioning. This mental health issue interferes with healthy thought processes and impacts a person’s ability to concentrate and make decisions. It changes the brain, and many people with depression find they frequently experience memory problems and have trouble remembering events or details.25
Correlating Hippocampal Neurogenesis, Depression, and Learning (Memory)
In 2006, Dyrbye and his colleagues saw the need for large, prospective, multicenter studies to identify personal and training-related features that influence depression, anxiety, and burnout among students and explore relationships between distress and competency.26 Newer studies are showing that depression has a neurobiological basis and is associated with functional and structural brain abnormalities.18 The hippocampus plays a fundamental role in learning and memory.27 It is a brain area where neo-neurogenesis is known to continue in the mature brain in animals and man, therefore making it a high capacity area for neuroplasticity.28,29
Benfenati noted that the major and most distinctive feature of the nervous system is the astonishing ability to adapt to the environment and to improve its performance over time and experience. This peculiar property is collectively referred to as “plasticity.” Neural plasticity represents the basis of the higher brain functions such as learning and memory or, conversely, that the built-in property of neural plasticity allows experience to shape the nervous system both functionally and structurally.30
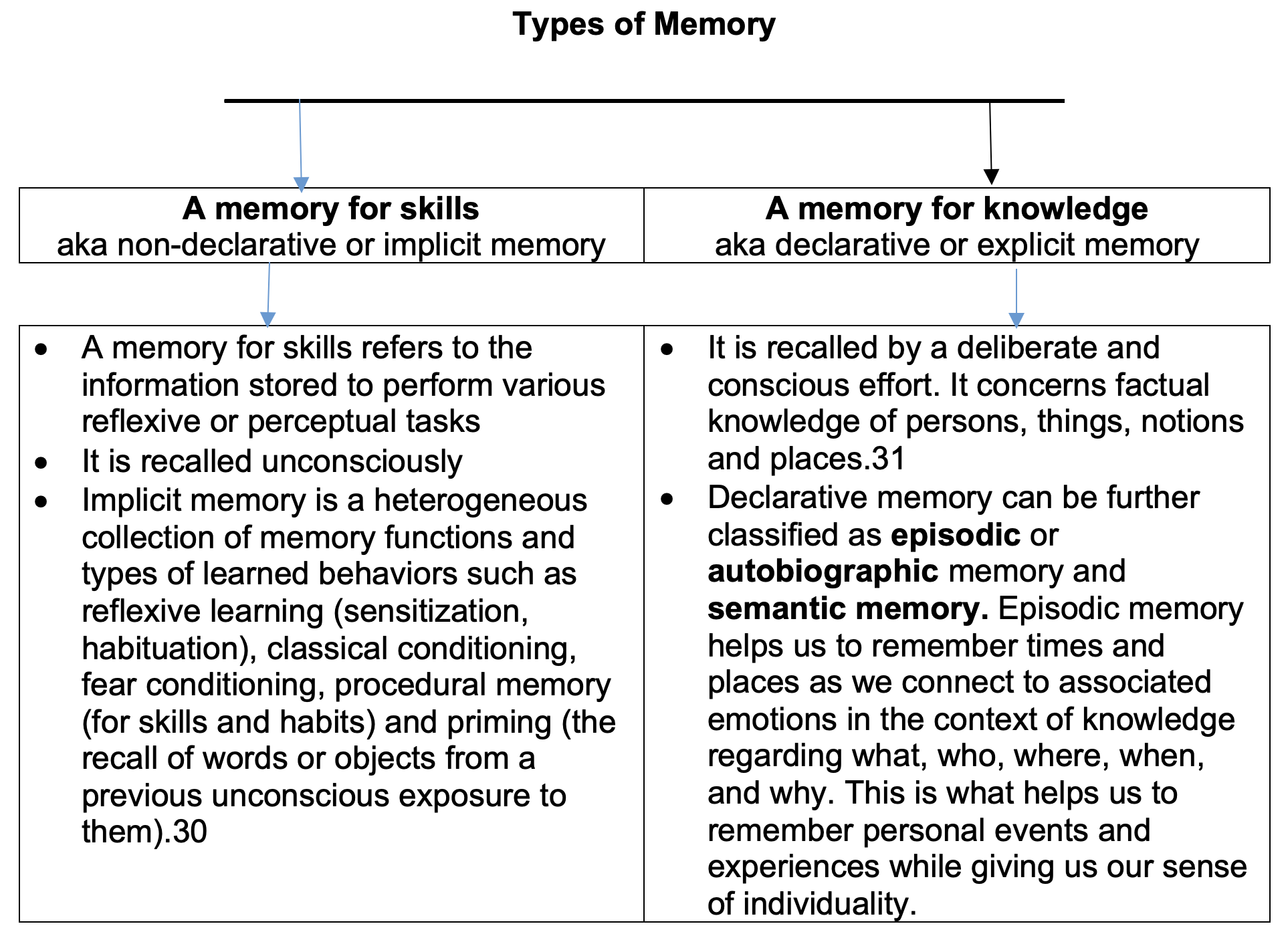
Neurogenesis and Memory (Figure 4)
Episodic memory allows us to remember personal events and experience and, being a link between what we are and what we have been, gives us the sense of our individuality. Semantic memory however, is that long-term memory portion that processes concepts and ideas. It is the memory of facts and concepts not necessarily drawn from personal experiences. Autobiographical memory and semantic memories merge with time. Brenda Millner with the famous H.M. case proved that multiple memory systems involve distinct brain areas and exhibit distinctive features.

According to Benfenati, explicit memory needs an intact medial temporal lobe (hippocampus), while implicit memory systems are integrated at various levels in the central nervous system including reflex pathways, striatum, cerebellum, amygdala and neocortex.30
Blackemore and later Pitternger noted the difference in the learning phase, the consolidation, and the recall of memories. Whereas implicit memory, like riding a bike may take time, explicit memory like learning a page of literature takes shorter times. Nonetheless, while explicit memory fades relatively fast in the absence of recall and refreshing, implicit memory is much more robust and may last for all our life even in the absence of further practice.31,32
Yau found that hippocampal neurogenesis and dendritic plasticity support running improved spatial learning and depression like behaviors in stressed rats. The dentate region of the hippocampus is a neurogenic region that has undergone extensive investigation as researchers have sought to understand the functional integration of new neurons into existing circuits.33
Exercise and antidepressants increase the hippocampal neurogenesis that is associated with improved cognitive function.34 Dendritic complexity of hippocampal neurons and neurotrophic factors are also increased by exercise.35,36 However, chronic stress decreases the proliferation of hippocampal cells.37 Stress causes dendritic atrophy.38 Stress also impairs cognitive performance.39
The investigation of the effects of stress on depression, learning and memory by Yau et al showed that running restored spatial learning to normal levels and decreased depression-like behavior in rats. The effects of running were associated with restored hippocampal neurogenesis and enhanced dendritic plasticity. They concluded that the findings suggested that enhanced dendritic plasticity and restored hippocampal neurogenesis, which represents structural plasticity of the hippocampus—an important requirement for maintaining hippocampal function.32
Many studies link spatial learning and neurogenesis. They show that numerous multiplying cells are required to acquire new information. Such studies find that higher baseline level neurogenesis is linked with better performance in the learning phase even though it does not affect probe trial performance.40 Such studies are supported by findings, which suggest that cognitive deficits appear when there is a decrease in the number of new hippocampal cells.41 Investigators show that exposure to psychosocial stressors decreases proliferation and neurogenesis in the adult hippocampus.42–44
There is an association between improved hippocampal function—improved spatial learning and decreased depression-like behavior and structural changes in the hippocampus—restored hippocampal neurogenesis in the dentate region and reversed dendritic remodeling.32 Cell proliferation in adult hippocampus is decreased by inescapable stress.45
Strengths and Limitations
Most studies focused on the neuroscience of memory. More studies will be necessary to delineate the interaction and correlation between stress, depression, and neurobiological mechanisms that affect academic performance. Such works could enhance understanding and give clarity on contrasting information on the effect of stress and depression on cognition, retrieval and retention of knowledge and the bidirectional relationship between depression and memory: depression affects memory, but memory problems likely exacerbate depression. Further studies could investigate whether or not management of anxiety or depression among students resulted in enhanced academic performance.
CONCLUSION
There is still slow progress on neuroscientific research correlating anxiety, depression, memory, and learning. However, the majority of available studies show that stress triggers depressive episodes in humans and chronic stress elicits depressive phenotypes, including memory impairments.
Most studies show that stress suppresses the adult hippocampal neurogenesis and impairs separation at encoding, leading to impoverished recollection. Stress impairs cognitive performance.
ACKNOWLEDGEMENTS
I thank Dr. John Hart for his input in editing an early draft of this manuscript, Amy Carson for her input in editing the final manuscript, and Pat Calhoun and Chandra Placer for their help in finding journals and retrieving pertinent information.