Chronic pain is epidemic within the United States, and low back pain (LBP) is known to affect up to 70-80% of the population at some point.1 Chronic pain is among the leading causes of disability within the United States, costing an estimated $635 billion annually, with chronic low back pain (CLBP) as one of the leading contributors to that cost.2 Over the years, treatments of chronic pain and CLBP have varied; however, in the early 1990’s the prescribing of opioids for chronic non-cancerous pain became common. Aggressive marketing strategies and over-prescribing of now-known addictive opioids has led to the current opioid crisis within the United States. With 66% of veterans reporting pain and 9% reporting severe pain they are an at-risk population for suffering from chronic pain and potential opioid use disorder.3 Many measures continue to be implemented to address the current opioid epidemic.
However, long-term opioid therapy (LTOT) persists as a common treatment method for chronic pain, despite evidence that LTOT for chronic pain comes with increased risks and with limited evidence supporting its long-term effectiveness.4 Recent guidelines in 2017 from the American College of Physicians (ACP) state that initial treatments for CLBP should consist of non-pharmaceutical treatments that consist of exercise, multidisciplinary rehabilitation, acupuncture, mindfulness, CBT, yoga or spinal manipulation.5 In 2003 guidelines from the Department of Veterans Affairs (VA) and Department of Defense (DOD) emphasized non-opioid treatments as the first line approach to the treatment of chronic pain.6 The VA has continued measures to reduce the risk of LTOT among veterans. In 2013, the VA implemented their Opioid Safety Initiative aimed at improving the safety of opioid prescriptions.7 Research on non-opioid pain management continues to be an area of growing interest. One article recently published in the Journal of Pain Medicine aimed to assess the opioid use among veterans of recent wars who received VA chiropractic services. Results showed that veterans were more likely to receive an opioid prescription at 90, 60 and 30 days prior to initiating chiropractic care than they were to receive an opioid prescription at 30, 60 and 90 days after initiating chiropractic care.8
Currently, there is a unique population of patients who are currently treated with LTOT, who are trying to be safely tapered from opioids. Manual therapies such as spinal manipulation, myofascial release etc. supplemented with active exercise may be the best approach to safely tapering patients from LTOT while addressing their chronic pain.
This current case report is interesting because it involves the chiropractic management of a post-operative patient with FBSS who was undergoing LTOT for his pain. There is currently no case-report or study that reports the chiropractic management of a post-surgical pain patient treated with LTOT. This paper aims to demonstrate that manual therapies such as HVLA spinal manipulation can be both safe and effective for treating post-surgical spinal pain and can assist in safely tapering patients from LTOT.
CASE REPORT
A 70-year-old male veteran presented to the VA Chiropractic clinic with chronic radiating low back pain, as well as pain at the cervicothoracic junction (CTJ). He had a surgical history of lumbar laminectomy in 2005 and cervical fusion from C3-C7 in 2014. He also had a medical history of alcohol dependence in current remission as well as PTSD and depression previously requiring hospitalization.
He was previously treated with a limited trial of physical therapy consisting of only passive modalities, including moist heat with electrical-stim/ultrasound over 9-visits without any significant relief. In addition to the trial of physical therapy treatment for his CLBP and CTJ pain he had been prescribed a course of LTOT primarily consisting of hydrocodone since 2011.
His primary healthcare provider determined that the risks outweigh the benefits and implemented a plan to safely taper him from his LTOT. He was referred to the chiropractic clinic to help manage his chronic pain while being tapered from the LTOT. At his initial visit to the chiropractic clinic he was taking 10mg of hydrocodone 3 times daily for a total dose of 30mg of hydrocodone that had recently been reduced from 10mg hydrocodone 4 times daily. He feflt that he was unable to “stay positive without opioids” and that without opioids he was unable to work and notes difficulties with activities of daily living without daily opioid medication. His pain level at that visit was rated 6/10, with his typical pain being rated as a 6/10, pain at its best was a 5/10 and 10/10 at its worst. His baseline Back Bournemouth Questionnaire (BBQ) was a 48/70 while taking 10mg of hydrocodone 3-4x daily.
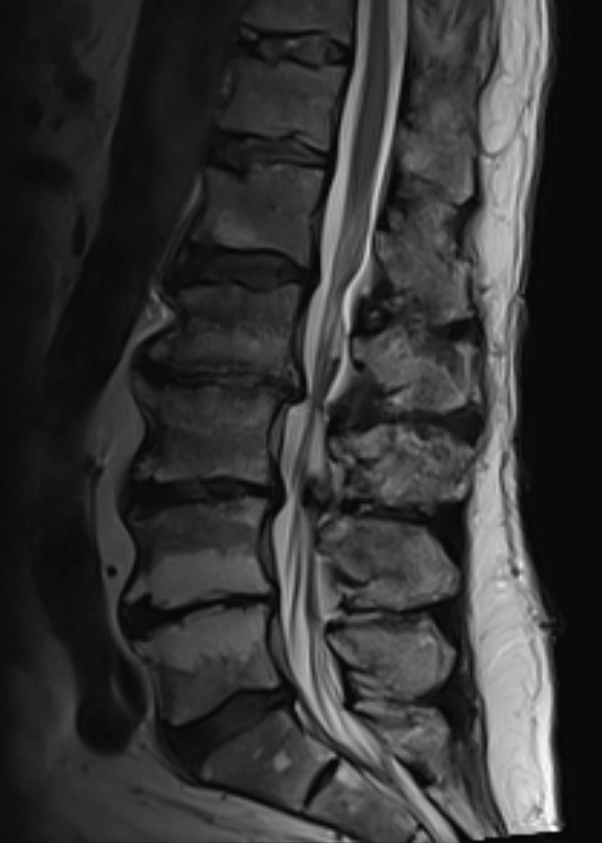
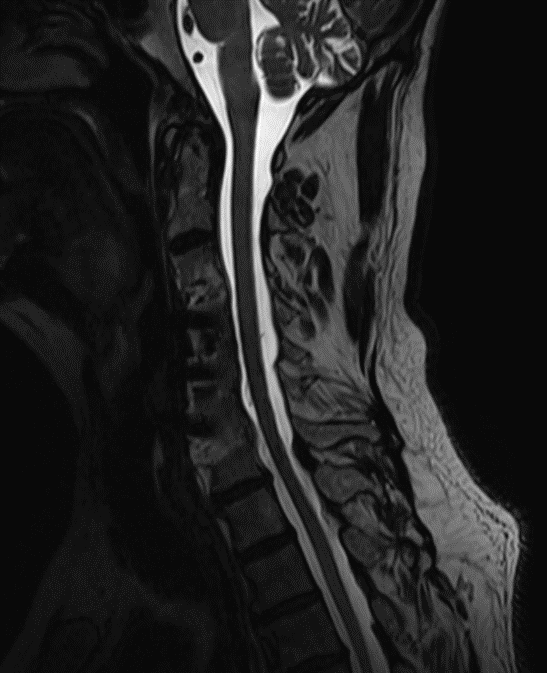
MRI (see figures 1 and 2) revealed moderate diffuse degenerative disc disease without canal stenosis with overlapping facet arthritis with associated neural foraminal stenosis. Patient presented overall neurologically intact without any neural tension signs present on exam. He did note some numbness and tingling into the right upper and lower extremities, active lumbar range of motion was limited into flexion and was provocative to LBP. Orthopedic testing revealed seated Kemp’s Test with facet loading was provocative for right-sided low back pain, while manual SI compression was unremarkable. Yeoman’s with shearing of the sacroiliac joints was unremarkable.


His initial visit consisted of myofascial release to the lumbar and thoracic paraspinal musculature. We then performed HVLA spinal manipulation to the CTJ, and thoracic spine as well as drop-table manipulation of the sacroiliac joints. We gave him a foam roller and educated him on its use to help increase his mobility of the thoracic spine. Stretches for his upper trapezius, levator scapula and rhomboids were provided. Following the treatment, he reported a 0/10 pain score and noted that the pain into his right upper and lower extremities was no longer present. He stated, “I can’t remember moving my neck this good.”
At his 1-week follow-up, he denied any significant post-treatment soreness or adverse reactions. He reported “I have been feeling really good, you guys really brought me a long way.” He stated “I am able to bend down and touch the floor now, before I couldn’t reach down and pick up a quarter and feel a lot looser.” He reported compliance with his self-care stretching with reported relief. He stated that his pre-treatment pain was now 4/10. Following treatment, which again consisted of myofascial release to the lumbar and thoracic paraspinals and HVLA to the CTJ, thoracic spine as well as drop technique to the sacroiliac joints, he reported a post treatment pain score of a 2/10.
At his 3rd visit he reported low back pain with resolution of his lower extremity radiating symptoms with full and non-painful lumbar range of motion. He reported some mild tingling into his right upper extremity. Pre-treatment pain was rated as a 5-6/10. He noted that he continued to use his foam roller daily with good relief. His opioids were reduced to 10mg of hydrocodone 2x daily. Prone press-ups were added to his self-care routine.
The 4th visit, approximately 2 months after initiating care, he reported a 7/10 pain score; however, he noted that he was down to 15mg total of hydrocodone, 1 10mg in the morning and half a pill in the evening. This is half of what he was taking when he began chiropractic care. He continued his self-care routine and denied symptoms into the extremities. At this visit, flexion-distraction was also incorporated into the treatment eliciting a favorable response.
At his 5th visit, he had an increase in the numbness in his right upper extremity and noted numbness in the 3-5th digit of his hand. After examination it was determined that he was experiencing the numbness due to a trigger point in the shoulder musculature. We provided him with a Theracane to perform at-home ischemic compression.
At the next visit he now had an acute exacerbation of his left upper back and shoulder. He rated the pain 10/10 with difficulty in all cervical ROM. Moist heat was applied to the affected area and then HVLA manipulation to the CTJ. He reported a significant decrease in pain following the treatment, with improved ROM.
A re-evaluation was performed at the 7th visit. We continued with RS Medical unit, Theracane foam rolling, prone press-ups and stretching routine. His neck pain was 6/10 while his LBP was a 7/10. He had now completely tapered from opioids for 3 weeks. He did report some fear-avoidance of physical activity due to no longer having opioids. His BBQ was at 49/70 without the use of any opioids. Treatment consisted of myofascial release as well as flexion-distraction and HVLA to the CTJ and the thoracic spine. He continues to follow up with the chiropractic clinic every 3-6 weeks to help manage his chronic pain.
DISCUSSION
In addition to opioids, spinal surgery has become common management of chronic neck and LBP. Over the past 2 decades the rates of lumbar spine surgery have steadily increased despite the prevalence of low back pain remaining steady over the past 2 decades.9 Reoperation rates for lumbar spine surgery are between 17- 28% at 11 years post-operation, fusion vs laminectomy respectively.9 With the steady increase of spinal surgery over the past 2 decades, there will also be an associated increase in patients who suffer from failed back surgery syndrome (FBSS). FBSS, described as persistent or recurrent pain after spinal surgery, occurs in up to 10- 40% of patients who undergo low back surgery.10 Currently, the clinical guidelines on the management of FBSS remain unclear although there is some evidence supporting the use of spinal manipulation and or mobilization post-surgically. However, the evidence supporting spinal manipulation and or mobilization post-surgically is currently limited to only case reports and case series, the largest of which described chiropractic management consisting of Cox Flexion Distraction Protocol for 32 post-surgical lumbar spine patients through a retrospective case series. Of the 32 patients in the case-series, 30 reported a decrease in their pain score. Across all surgical groups the average pain score was 6.4 at presentation and was reduced to 2.3 on average after an average of 14 treatments over 63 days. No patients reported an increase in pain with treatment, and only 2 reported no change. There were no adverse effects reported.11 Coulis and Lisi described the chiropractic management of 3 postoperative spine patients with various manual therapies including high-velocity low-amplitude manipulation (HVLA). Two of the 3 patients had underwent low back surgery, of which 1 patient had an L-5 laminectomy, left L4-5 nerve root decompression and right L5-S1 nerve root decompression while the other had L3-L5 laminectomy. A 3rd patient had undergone surgical fusion of the cervical spine from C3-T3. One low back pain patient was treated with HVLA spinal manipulation and flexion/distraction while the other low back pain patient was treated with just flexion distraction. The cervical spine pain patient was treated with HVLA of C1-C2 and T3-T6. Both LBP patients reported improvements in pain and or function of 50%. The cervical pain patient reported typically 33% reduction of pain. They reported no adverse reactions.12
CONCLUSION
Due to decades of over-prescribing opioids for the treatment of chronic pain there is a clear opioid crisis within the United States. Although major steps have been taken in safely prescribing opioids moving forward, it is less clear how to handle patients on LTOT. Guidelines suggest individual tapering plans geared toward the patient to safely taper them from their LTOT. However, these guidelines offer little guidance in exactly how to accomplish tapering LTOT patients from daily opioids. This case, while limited as a case report, aims to offer some clinical insight into the means of safely tapering a patient from LTOT through integrative care including spinal manipulation and active rehabilitation.
The continued increase in the prevalence of back surgery for managing chronic pain FBSS will also likely continue to rise. As opioid use for chronic pain declines, it is important to explore novel approaches for managing FBSS. This case suggest that manual therapies, including manual spinal manipulation, can be both a safe treatment option for FBSS. This case appears to be unique because it addresses the challenges of managing both a LTOT patient being tapered from daily opioid use who also has FBSS.
A trial of chiropractic care with supplemental at-home active rehabilitation was able to help a postsurgical spinal pain patient who was also being safely tapered from long-term opioid therapy.