

INTRODUCTION
Spondylolisthesis is the general term for the displacement (in any direction) of a vertebra in relation to the segment immediately below; a retrolisthesis is specifically the posterior displacement of the superior vertebra in a functional spinal unit. The incidence of spondylolisthesis in the general population is about 5-7%.1
There are many causes of spondylolisthesis, including congenital, degenerative, traumatic, pathologic, iatrogenic, and isthmic. The last refers to a defect of the pars interarticularis, which then results in an anterior translation subluxation over time (anterolisthesis), and most commonly occurs at L5-S1 followed by L4-5.2 Although most research has been conducted on anterolisthesis,3 spondylolisthesis subluxations in general are associated with back pain, central canal stenosis, and lateral recess or foraminal stenosis.2
The quantification of spondylolisthesis is best made from the lateral lumbar radiograph, using George’s line1 or posterior tangent lines,3 which are lines drawn along the posterior vertebral body margins of the affected and inferior segment. Although the ideal alignment is no translation offset (0mm), a translation offset measurement of 4.5mm or greater is considered pathologic in the neutral position in the lumbar spine.4
Typical treatment for spondylolisthesis includes surgery when there is neurologic involvement. Non-surgical treatment of spondylolisthesis includes pharmacological intervention, activity modification and/or physiotherapy exercises for symptomatic patients5 as well as spinal manipulation. Non-surgical structural correction of spondylolisthesis is virtually non-existent, and specifically for retrolisthesis there is no effective non-surgical treatments. The only literature we could locate was a single case report by Fedorchuk et al.6 who reported the correction of a grade 2, L4-5 anterolisthesis. An initial 13.3mm anterolisthesis was reduced to 2.4mm after 60 treatments over a period of 45 weeks by CBP traction methods as well as spinal manipulation and exercises.
The purpose of this case is to describe the reduction of multiple retrolistheses and increase in lumbar lordosis in a male with back pain.
CASE REPORT
A 32-year-old male had mild, recurrent low back pain (LBP) as well as middle back and neck pain. The pains were aggravated after sitting too long or by bending forward. On average, the pains were scored a 6-7/10 on a numerical pain rating scale (NPRS: 0=no pain, 10=worst pain ever), and an 8/10 when at its worst, reported to be at the end of the day. The patient scored a 34% on the Oswestry Low Back Pain Disability Questionnaire [ODI7]. The patient had not experienced previous spinal trauma or injury.
Range of motion assessment showed generalized, mild limitation for the lumbar and cervical areas. Palpation demonstrated tightness along the paraspinal muscles bilaterally, in the lumbar and cervical spinal areas. Other orthopedic tests were normal or unremarkable; there was no neurologic involvement.
Radiographic assessment was performed and images were analyzed using the PostureRay system (PostureCo., Inc., Trinity, FL, USA). This system uses the Harrison posterior tangent (HPT) method to measure the sagittal plane images. The HPT method incorporates lines drawn contiguous with the posterior vertebral body margins, enabling quantification of intersegmental relative rotation angles (RRAs) at each vertebral level, an overall regional lordosis (i.e. L1-L5) or absolute rotation angle (ARA), as well as intersegmental translation values (i.e. for the measurement of spondylolisthesis). This method has been shown to be repeatable and reliable8,9 as has standing posture.10
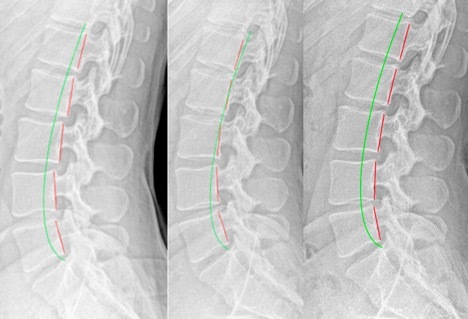
The notable findings in the lumbar spine included a congenital fusion of L5-S1 (Figure 1). There an increased lumbar lordosis L1-L5 ARA of 47.1° (vs. 40° normal11,12) as well as multilevel retrolisthesis subluxations at every level from T12-L1 to L4-5 (Table 1). Notably, pathologic measures of retrolisthesis (i.e. ≧4.5mm4) involved L1-2 (4.5mm), L2-3 (5.9mm), L3-4 (5.2mm), and L4-5 (4.7mm) intervertebral joints.

Intervention and Outcome
Treatment was aimed at increasing the lumbar lordosis by using CBP technique protocol.13–15 Lumbar extension traction was performed for the purpose of reducing the multilevel retrolistheses. Extension traction stretches the ligamentous tissues causing creep relaxation and plastic deformation.16,17 These methods have been shown to increase lumbar lordosis in several clinical trials18–22; more specifically, they have been shown to reduce spondylolisthesis.6 Lumbar spinal manipulation as well as mechanical massage laying supine on a PowerPlate whole-body vibration platform23 (Performance Health Systems, Northbrook, IL, USA) was also performed to provide pain relief. Treatments were given at a frequency of approximately 3 times per week for the duration of care. An approximate 1-year follow-up was also performed.
Results
The patient was re-assessed and reported all pain to be significantly reduced; the LBP was completely resolved even after prolonged sitting and forward bending. There was an increase in overall cervical and lumbar flexibility to within normal limits. Score on the ODI was 14%. Radiographic assessment showed a reduction of retrolisthesis subluxations, the T12-L1 reduced to 1.6mm (vs. 2.3mm), L1-2 reduced to 1.4mm (vs. 4.5mm), L2-3 reduced to 3.4mm (vs. 5.9mm), L3-4 reduced to 3.0mm (vs. 5.2mm), and L4-5 reduced to 3.4mm (vs. 4.7mm). The overall lumbar lordosis remained stable (-49.6° vs. -47.1°).
A 13-month follow-up assessment was performed. During the 1-year time frame, the patient received infrequent ‘maintenance’ treatment sessions, approximately twice per month, but had not been in for treatment 3 months prior to this assessment. He stated that he was well and the original neck and back pain were relatively stable, being minimal with only a mild stiffness noted after prolonged sitting. ROM for cervical and lumbar spine was normal. Score on the ODI was 0%. Radiographic assessment revealed that the lumbar spine had remained stable; the previous retrolistheses also remained non-subluxated (<4.5mm), measuring -0.6mm, -2.1mm, -2.4mm, -2.5mm, and -4.1mm for the T12-L1 to the L4-L5 vertebrae, respectively. The lumbar lordosis remained stable at -46.9°.
DISCUSSION
This case demonstrates the resolution of LBP and the reduction and correction of multilevel Grade I retrolistheses in a patient who received CBP treatment. These results were accomplished non-surgically and over a period of 14-weeks that also coincided with improvements in disability and flexibility. Stability of the structural correction and symptomatic improvements remained at a 13-month follow-up.
Since our patient did not have neurologic involvement, and with the retrolistheses only qualifying as a category Grade I translation (0-25% translational offset), surgery was not an option.24,25 For non-surgical treatment options, exercise is generally the treatment of choice for retrolistheses.26 Exercise programs however, do not reduce the translational offset but are aimed at strengthening the abdominal and core torso muscles. As mentioned, the only case we were able to locate documenting significant non-surgical correction of spondylolisthesis was by CBP methods and reported an 11mm reduction of an L4-5 anterolisthesis nearly a year of care.6 Our case therefore, is the second case documenting a significant reduction of lumbar spondylolisthesis, as our patient showed multilevel retrolistheses reduced after 36 treatments over 14 weeks.
Retrolisthesis is an indication of segmental instability and leads to future degenerative processes.27–30 In fact, “A retrolisthesis hyperloads at least one disc and puts shearing forces on the anterior longitudinal ligament, the annular rings, nucleus pulposus, cartilage end plates and capsular ligaments. The bulging, twisting and straining tissues attached to the endplates pull, push and stretch it. It is worsened with time, gradually becoming irreversible.”26 This is precise mechanism for the development of degenerative joint disease. Thus, reducing mild or early spondylolisthesis may help in early treatment to prevent LBP and future degenerative processes in those affected. In fact, evidence suggests that it may be more feasible to achieve better long-term success by providing early (and effective) treatment for spinal subluxation when diagnosed in younger patients and/or when the deformities are less severe, as logically, over time, these spinal conditions will worsen.31–35
Since spondylolisthesis is a cause of back pain and arthritis, and since it can only be diagnosed via radiography, radiology is indicated when it is suspected.34–38 The challenge is, of course, that it is rarely suspected, thus indicating that treatment may not take its presence into account.
With regard to the idea that better imaging for spondylolisthesis may be CT, Giles et al., found that when categorizing pathology incidence comparing X-ray and CT, for those having retrolisthesis, “true lateral plain X-ray film revealed a sensitivity and specificity of 100% for bulge/protrusion.”29 Thus, it is crucial to understand that retrolisthesis has concomitant disc pathology, and general exercises for LBP may not be necessarily advised; more specific treatments, as used in this case, aimed at reducing the olisthesis may be more appropriate and effective. More research efforts into evaluating whether these traction methods are routinely effective at reducing retrolisthesis subluxations is warranted.
Clinical papers do describe non-surgical treatment of lumbar retrolisthesis; for example, by Alcantara et al.39 and Paulk and Harrison.40 In both these cases, patient symptomatology improved dramatically in a patient with retrolisthesis; however, neither reported reductions in the retrolisthesis malalignment.
In the Paulk paper,40 extension traction led to an increased lumbar lordosis but did not have an effect on the L5 retrolisthesis, as observed in their Figure 2. Whether the structural reduction of retrolistheses resulted in the pain relief cannot be ascertained from this case; however, spinal traction methods are definitively known to change structural spine alignment,18–22 and there are undoubtedly long-term consequences from ‘non-surgical treatment’ versus ‘non-surgical reduction’ in treating retrolisthesis.
One retrospective paper described a ‘34% reduction’ of retrolisthesis by Gonstead chiropractic manipulative therapy.41 It must be noted that although statistically significant, the reported reduction was only 1.12mm. As stated by the authors: “Even though a relative change in position had been demonstrated, what significance does this convey to the patient and or his/her management?”41 The authors also stated that if 34% reduction proves to occur in larger retrolisthesis subluxations (>5mm), this will likely prove to be more clinically meaningful. In the present case, the magnitude of retrolistheses was substantial enough to reduce the translational offset deformity to below the pathological threshold (<4.5mm). We believe that structural correction to retrolisthesis subluxation is best for long-term patient outcomes, as the sooner a displacement can be structurally reduced, the less time for concurrent deterioration and degenerative processes to evolve.27–30
Limitations to this study includes the obvious reporting of a single case. As discussed, this case, along with the work of Fedorchuk et al.6 provides initial evidence indicating a new approach to treating spondylolistheses. The stability of retrolistheses reductions found at the 13-month follow-up also was a strength of this report. The presence of spondylolisthesis, it seems, may now have a non-surgical treatment that is specific to the translational offset and may ultimately be the treatment of choice. More research into the CBP technique approach is warranted to further verify and validate this approach and its ability to reduce spondylolisthesis.
CONCLUSION
This case illustrates that early lumbar spine (grade 1) retrolistheses are amenable to correction via non-surgical means. This is the second case in the literature showing spinal traction successfully reducing lumbar spondylolisthesis. While we cannot definitively say that the structural reduction of retrolistheses resulted in the pain relief, there are undoubtedly, long-term consequences from merely ‘non-surgical treatment’ versus ‘non-surgical reduction’ in treating retrolisthesis.
Conflict of Interest
PAO is a paid consultant to CBP NonProfit; DEH teaches chiropractic rehabilitation methods and sells products to physicians for patient care as used in this manuscript.