



INTRODUCTION
Harrington rods are titanium or stainless steel spinal implants used to treat spinal instabilities or spinal deformities, such as severe scoliotic curves. Typically, Harrington rod fusion surgery is performed with few side effects,1–3 but occasionally complications occur. Such complications may include hypertonicity in the spinal musculature, acceleration of degenerative changes of the spine, or various neurological symptoms.1,2
Scoliosis is a lateral curvature of the spine that is most commonly observed between the ages of 10-to-14 years of age.4 In the case discussed here, the patient had a cervicothoracic curve, which is an uncommon scoliosis presentation.5,6 The most common course of treatment for scoliosis is watchful waiting and a spinal rehabilitation program.7 This type of treatment is recommended when the curve is 0-20° degrees.7,8 For curves of 20-40°, observation and exercise are typical parts of the treatment plan along with bracing protocols.7 A curve greater than 40° is considered a surgical case due to the risk to other bodily functions.7,8
Migraines are a type of chronic and recurrent headache affecting one side of the head.4,9,10 Migraines frequently manifest in a clinical setting with symptoms of nausea, fatigue, and sensitivity to light.9 Many patients take daily medications to ease their pain and symptomatology. Chiropractic care is an alternative form of treatment for individuals with migraine.9
The literature has limited information about Harrington rod fusion surgery as a risk factor for migraines; however, decreased range of motion and muscular hypertonicity may affect the length and severity of a migraine.4 This case report demonstrates the need for future research using spinal manipulation combined with myofascial release and rehabilitative exercises for patients with Harrington rod fusions who have migraine headache.
CASE REPORT
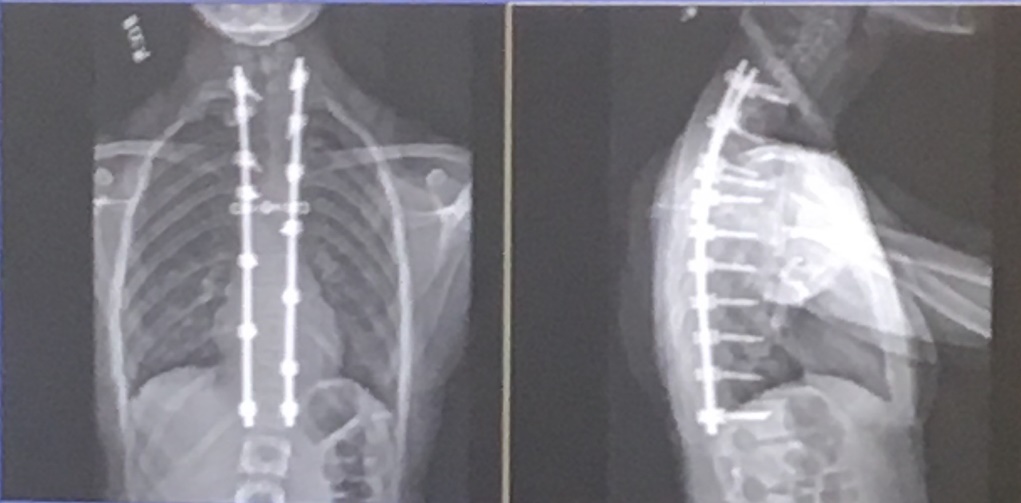
A 20-year-old female sought care for a chief complaint of daily migraines, which were diagnosed by her primary care provider shortly after she received a Harrington rod fusion of her lower cervical and entire thoracic spine to correct a cervicothoracic scoliosis at the age of 13-years-old (Figure 1). The surgery was followed by a rehabilitative course of physical therapy.

She reported that she had previously received a course of chiropractic care, limited to only spinal manipulative therapy, which yielded temporary relief from her migraines. She then sought other treatment options for her migraines, including multiple over-the-counter non-steroidal anti-inflammatory (NSAID) medications, which provided her only minimal relief.
During the initial examination, her active range of motion was decreased bilaterally during rotation and lateral bending, indicating sternocleidomastoid and scalene muscle involvement. Her pain increased with resisted range of motion testing during O’Donoghue’s test. Passive ranges of motion were within normal limits for all cervical motions and no discomfort was reported, decreasing the probability of ligamentous damage. Soft tissue palpation revealed hypertonicity in both the sternocleidomastoid and scalene muscles bilaterally. End-feel motion palpation of the cervical spine through flexion, extension, rotation, and lateral flexion found decreased motion of the second cervical vertebra, most limited in right rotation.
Myofascial release in the form of manually stripping along the direction of hypertonic fibers while passively lengthening the muscle was performed to decrease hypertonicity of the cervical musculature.11 (Figures 2-5)




Diversified spinal manipulative therapy in the supine position was applied to the second cervical vertebra in the direction of right rotation in order to restore motion. She displayed an immediate increase in cervical ROM following treatment and reported relief from the tension she had experienced in her cervical spine and head. We gave her recommendations for a home-based self-stretch regimen of the sternocleidomastoid and scalene musculature, and encouraged her to perform these activities 3-to-5 times per day, holding for 30 seconds. Follow-up sessions involved 1 treatment per week, over a total of 6 weeks. A re-evaluation was performed at the 6th treatment. She reported her migraine occurrence had diminished from once daily to once per week over the first 2 weeks of treatment, and at the time of reevaluation she had experienced no migraines for the past 3 weeks.
DISCUSSION
Although chiropractors may shy away from adjusting a patient with Harrington rods, we would urge the profession to examine these patients from a qualitative biomechanical approach.12 A patient with Harrington rods may have extreme movement restriction, and when the surgery is performed at a young age will undoubtedly have effects on overall growth and development. This patient was an active 13-year-old who previously participated in many sports, ranging from gymnastics to jujitsu. After surgery, she was instructed to stop all activity and to be cautious with any movement for the rest of her life. Not only did this restriction affect her musculoskeletal system over time but it also affected her mental health. Increased stress and decreased quality of life have been linked to migraine occurrence.13 Such surgeries can lead to an increased progression of degenerative changes within the area of fusion as well as compensatory instability of the areas above and below the fusion.4 Compensatory instability can lead to hyperactivity and overuse syndromes of the surrounding musculature, which is the proposed headache mechanism in our patient.7
Taking the above into consideration, we decided this patient should not only be treated with spinal manipulation and myofascial release, but should also begin increasing her level of activity. To this end, a biomechanical assessment was conducted.12 With a goal of increasing cervical range of motion, and understanding that the rods would limit that possibility within the segments affected, treatment began with myofascial release as seen above.
Qualitative biomechanics is structured on the idea that we must first have the quality of the desired movement and then we begin to have the quantity, or the desired activity.12 In this case, it was necessary to address the overactivity of the cervical musculature and restriction of the upper cervical spine, then begin to ensure an appropriate amount of mobility for the patient.
Limitations
This case report is limited in scope and daily migraine headache is not a typical clinical presentation of cervicothoracic scoliosis.
CONCLUSION
While a large amount of research on idiopathic scoliosis in teenagers exists, this case offers an uncommon presentation. Through the use of myofascial release on hypertonic muscles, chiropractic adjustive therapies, and rehabilitative stretches, relief of migraine following a fusion of the cervicothoracic region demonstrated in this case provides an incentive for further research into the potential benefits of chiropractic care patients with Harrington rod fusion.
CONSENT
Written consent for publication was obtained from the patient.
COMPETING INTERESTS
The authors declare that they have no competing interests.