



INTRODUCTION
Symptoms within the oral cavity can be attributed to numerous conditions and medical diagnoses, some of which give rise to very similar presentations. Due to the complexity of osseous, myofascial, and neurologic components to the orofacial region, a substantial list of differential diagnoses may be demonstrated. The clinical aspects of this report demonstrate a more atypical presentation for pain within the oral cavity. The following introductory information outlines the elements of the highest suspicion regarding the clinical presentation of the assessed patient condition.
Chronic orofacial pain may affect up to 7% of the population throughout an individual’s lifespan.1 Pain, changes in food consumption, temperature tolerance, or favoring one side of the mouth may be some of the reasons a patient initially presents with an orofacial concern. Some may not present to a healthcare specialist when symptoms arise because they are unsure of their options for care.2 A few significant pain-generating tissues to discuss include neurogenic or cranial neuropathies3–5 and those of musculoskeletal origin.6 While the list of conditions which may refer pain to the orofacial region can be daunting, taking a thorough history will help the clinician achieve a correct diagnosis.
Neuralgic pain has a paroxysmal quality, which is typically described as lancinating, electrical, shock-like, or jabbing.1,3,5 Patient’s typically report bouts of pain lasting from a few seconds to under a minute; they may even be woken from sleep. Diagnostic “nerve-blocks” in the setting of facial pain do not necessarily define the site from which the pain arises because of the overlap of cranial nerves V, VII, IX, X, which converge on the spinal trigeminal nucleus.1 Trigeminal Neuralgia (TN), also known as Tic Douloureux, is the most commonly discussed facial neuralgia.1,3,5 An essential feature of Trigeminal neuralgia is that objective signs of sensory loss cannot be demonstrated on examination4 and the presence of a trigger (shaving, wind hitting the face, eating, etc.).3–5 Another, less commonly discussed neuralgia, is that of the 9th cranial nerve: the Glossopharyngeal. The associated signs and symptoms may include localized or radiating pain from the throat4 as well as a higher prevalence of night pain that will awaken the patient.5 Burning Mouth Syndrome (BMS), another condition presenting with typical neuropathic pain patterns, has been shown to have a higher prevalence for post-menopausal women. Some hypothesize that decreases in estrogen levels may lead to weakness to the oral mucosal layer.7 Finally, oral neuralgias may present with an atypical or nonspecific presentation, ultimately giving rise to nonconforming neurologic symptoms. These symptoms may include some of those previously demonstrated, such as burning, stabbing, sharpness, or electrical shock-like within the oral cavity. Simultaneously, a series of craniofacial nerves could be the culprit such as the superior and inferior alveolar nerves, hypoglossal nerve, glossopharyngeal nerve, facial nerve, trigeminal nerve, and palatine nerves. It is up to the clinician to perform a comprehensive history and thorough examination to better determine the location of the presenting neuralgia and establish which orofacial nerve is the leading contributor.
Aside from organic disease of the oral cavity and neurological pain patterns, mechanical dysfunction within the joints of the jaw may refer to pain in the orofacial region. Temporomandibular disorder (TMD) is a common condition treated by chiropractors regularly and affecting a quarter of the general population.1,8,9 This may be caused by nocturnal bruxism, myofascial trigger points in the face and neck region, disc derangement, or otic symptomatology. History of muscle tenderness and/or cervicogenic headaches might be a result of trigger points referrals within the following muscles: temporalis, masseter, medial and lateral pterygoids, buccinator, upper trapezius, sternocleidomastoid, splenius capitis, and suboccipitals.8,9 Although not all of the above listed muscles refer pain to the orofacial region, a number of them do refer pain into the maxilla and upper teeth.6
Currently, there are many therapeutic interventions used for the presentation of orofacial pain. These include pharmaceutical interventions, rhizotomy, other surgical interventions, manual therapy, and/or co-management.1,3–5,10 When the diagnosis of neuropathic pain or neurology is made, a regimen of tricyclic antidepressants or carbamazepine are typically administered. Carbamazepine is the best studied treatment for classic TN and is deemed effective.1,5,10 Gabapentin has also been found to be clinically implicated in those worried about drug interactions or those worried about hepatic or renal toxicity.10 When it comes to surgical interventions; rhizotomy, or intended-nerve lesioning can be done 3 ways: through radiofrequency thermocoagulation which uses applied heat, mechanical ganglionic compression using an inflated apparatus, or chemical injections.1,10 Another commonly discussed surgical intervention is microvascular decompression, a major neurosurgical procedure that involves craniotomy and the removal or separation of various vascular structures.1,10 Manual trigger-point therapy may be beneficial for when identification of an active myofascial trigger-point as the pain-generating tissue has been made.6 Many psychosocial and behavioral disorders may begin to manifest in patients with chronic orofacial pain10,11 requiring a multidisciplinary approach for appropriate case management.
Our case report depicts a patient who presented for chiropractic management of atypical hard-palate pain. This report will illustrate the initial presentation to the outpatient clinic, as well as the evidence-informed decisions that were determined when devising a case management program. The principle focus of this paper is to describe and discuss an atypical palate presentation and the chiropractic interventions utilized to achieve outcome goals.
CASE REPORT
History
A 76-year-old male had a chief complaint involving tooth and oral pain. When prompted, he pointed to a portion of the hard-palate, just posterior to the left lateral incisor and canine. He explained an insidious onset beginning for the first time about 2 years prior. He stated that he had been taking medications such as acetaminophen-codeine, Orajel, oxcarbazepine, and duloxetine with some palliative results. The aforementioned medications were administered through multiple visits over 2 years through several providers. Hot and cold foods or beverages had been provocative; any physical touch to the area also increases the pain. The quality was described as a continuous ache with occasional throbbing and sharpness without any associated radiation. The severity was
rated as an 8/10 on average on the Numeric Pain Rating Scale (NPRS). He had seen multiple healthcare practitioners for this complaint, including primary care physicians, physician assistants, dentists, and multiple neurologists, largely not finding any beneficial remedies or therapies. The patient denied any red flags suggestive of visceral or emergency pathology, such as dizziness, diplopia, dysarthria, dysphagia, drop attacks, ataxia, nausea, numbness, or nystagmus.
Prior to presenting to the university chiropractic clinic, the patient had two previous appointments with the acupuncture clinic within our university outpatient facility, with minimal therapeutic benefits. While receiving interventions within the acupuncture division, he was recommended to schedule an appointment within the chiropractic clinic. The patient’s past medical history, familial history, and social history were only remarkable for early signs of dementia that was being monitored by other professionals and routine dental work including dental caps across the upper row of teeth; otherwise, the rest of the patient’s complete history was not pertinent to the presenting complaint.
A 10-point NPRS was administered upon the first encounter; 0 indicating no pain, and 10 being unbearable, excruciating, pain. His hard-palate pain averaged 8/10 throughout the 2-year history. The clinical outcome assessment tool of a Patient-Specific Functional Scale (PSFS) was also utilized with 2 questioned activities: “direct pressure or tongue contact over the site of pain” and “consumption of hot/cold foods or beverages.” The PSFS also uses a 10-point scale when assessing the specific activities outlined by the patient; 0 indicating the patient can perform the activity without pain or irritation and 10 indicating the patient cannot perform the activity at all. Regarding both of the questioned activities, the patient rated both as an 8/10 on average.
Due to the anatomic location and neurologic quality of the presenting complaint, involvement of the greater palatine nerve was considered. At the initial chiropractic encounter, the diagnosis of chronic, continuous, greater palatine neuralgia regarding the teeth and central portion of the hard-palate in an otherwise healthy 76-year-old male was rendered. Competing differential diagnoses for the history included the following: Burning Mouth Syndrome, neuropathy (trigeminal, glossopharyngeal, or palatine), and herpetic infection.3–5,7 BMS was considered as our 2nd leading differential, following specific neuropathy, due to the nonspecific neurologic presentation within the oral cavity. Ultimately, the pinpoint, precise, location outlined by the patient within the oral cavity gave the impression of a specific neuralgia as opposed to nonspecific BMS.
Physical Examination
The patient demonstrated a mild postural anterior head carriage with some anteriorly translated shoulders bilaterally; otherwise, there were no other notable postural changes or gait abnormalities. There were no visual distortions, abrasions, scars, swelling, or deformities of the face. Palpation of the skull revealed no tenderness or palpable masses. Palpation of all head and cervical lymph nodes was within normal limits, with all assessed nodes being non-tender and nonpalpable. His facial expressions and testing of CN XI were intact and void of abnormality or rigidity. Pupils were equal, round, and reactive to light with no indications of nystagmus or loss of vision through fields of gaze and peripheral assessment. Palpation and transillumination of the maxillary and frontal sinuses and other associated structures of the face/skull were non-tender and non-contributory. Palpation of the throat, trachea, thyroid, and associated structures of the mouth and throat were largely within normal limits. Visual inspection of the area of complaint did not elicit any abnormalities, lesions,
abscesses, cuts, abrasions, burns, or masses. Sustained palpation and percussion of the teeth and the area of complaint, over the hard-palate, did increase the pain and complaint. Other aspects of facial and oral palpation were non-tender or not non-replicative of the patient’s CC. Subsequent facets of the patient’s full physical including a heart, lung, abdominal, motor reflex, and sensory neurologic exam were unremarkable or notable for abnormalities or any areas of inclusion towards the overall complaint or pathology.
Orthopedic examination began with active range of motion testing across the cervical spine in 6 planes, yielding no motion deficits or areas of provocation. Foraminal Compression test, Jackson’s Compression test, and Maximal Foraminal Compression test were negative for pain provocation or complaint replication. A Valsalva test was administered and found to be non-painful and noncontributory. Relevant soft tissue examination across the cervical and facial regions, including the mandibular and cranial structures, was unremarkable and overall unprovocative. Osseous temporomandibular joint palpation and spinal segmental testing across the occiput and cervical spine did not reveal any tender segments, but asymptomatic articular restrictions were present.
Management
The working diagnosis of chronic greater palatine neuralgia was largely the clinical suspicion following a complete history and examination. This suspicion of palatine nerve involvement stems from the nerve-related symptomatology through branches of the Trigeminal Nucleus and Pterygopalatine (PP) Ganglion, which innervate the hard-palate across the intra-oral maxilla and palatine bones.
The management plan was to be rendered 2 times per week for a total of 4 weeks. Due to inclement weather an additional week was added. Evidence-informed office care incorporated a multi-modal series of chiropractic manipulations, manual therapies, physiotherapies, and nutritional recommendations. High-velocity-low-amplitude chiropractic manipulative therapy was applied to the upper cervical segments of C1-C3 to reduce any potential Trigeminal Neuralgia association.12,13 Craniofacial manual therapies and the utilization of a model 1 chiropractic Activator manipulative tool were applied in an off-label approach over the areas of the frontal and maxillary sinuses to provide correlative motion across the surrounding connective and bony structures. Also, manual suture mobilization was used with a sustained shearing pressure across the Sagittal Suture. (See Figures 1-3)
_utilization_across_the_frontal_sinus.jpeg)
_utilization_across_the_zygoma_and_maxillary_sinus.jpeg)

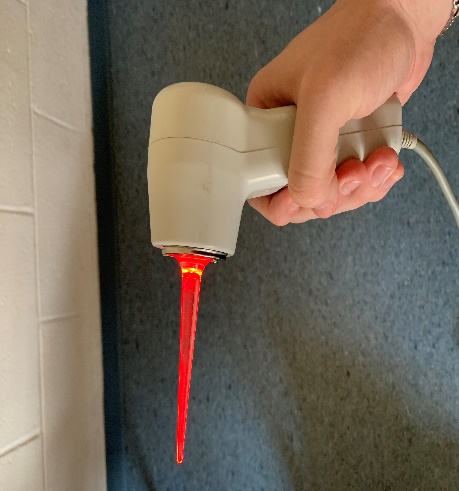
Each encounter was largely centered around the application of low-level laser therapy (LLLT) executed externally over the features of the Trigeminal Nucleus, PP Ganglion, Stellate Ganglion and the intra-oral cavity – over the site of pain.14–16 (See Figures 4 and 5)


The administered laser therapy was conducted via an MR4 laser system, manufactured by Multi Radiance Medical (Solon, OH). The specification of the apparatus itself for therapy was a preset dosage chosen at a setting of “semi-medium” depth for a pulse frequency of 500Hz; all for a total therapy length of 4 minutes over the targeted locations. At the initial encounter, it was also recommended to the patient to begin a regimen of oral supplements including Magnesium, Vitamin A, and a B Vitamin complex to decrease any associated nerve inclusion and to aid the integrity of the oral mucosa.17,18
Outcome
At the initial follow-up encounter, the patient reported no reductions or changes regarding the complaint; the quality and severity remained unchanged and the patient continued to express severe discomfort. Therefore, in the ensuing visits the trial of chiropractic care outlined within the management plan was carried out unaltered.
At the 4th follow-up encounter, he began to note reductions in his pain. He then mentioned the complaint to be “less bothersome” and was now an “on and off” problem rather than a continuous issue, as noted on all of the previous encounters. Within the following visits, the patient always explained the complaint to be bothersome; however, the frequency, severity, and quality were mentioned to be lessening. Throughout the 5-week course of care, the management plan was unaltered, and visit frequency and patient compliance remained consistent until the reassessment evaluation.
At the reassessment evaluation, his PSFS and NPRS produced values of 8/10 at the initial encounter and later yielded values of 6/10 respectively. The re-evaluated values for the PSFS and NPRS represented a difference of 25%. He had a mild reduction in pain, chronicity, and continuous involvement regarding the presenting oral complaint following the 5-week trial of chiropractic interventions. The elicited diagnosis remained appropriate throughout the course of care and applicable changes were made regarding the encounter frequency within the management plan.
Following the 5-week course of intervention, formulated goals in accordance with the given outcome assessments and the Minimal Clinically Important Difference (MCID) were met; however patient satisfaction was not reached. Due to the patient’s disposition regarding the therapeutic outcomes, he was offered alterations to the plan frequency. The therapeutic benefit was not significant enough for his satisfaction. The patient was hoping for greater benefit from the administered therapies despite the quantitative goal satisfaction and opted to conclude therapy.
Originally, following therapy cessation, he was going to be scheduled for a one-month follow-up phone interview, however the patient returned 2 weeks after concluding therapy with an exacerbation of symptoms. The patient then described the pain to be greater than previously exhibited at any of the prior patient encounters. It was then our recommendation to begin therapy again, keeping with the original management plan that demonstrated quantitative benefit and offer avenues for co-management. However, the patient’s return for continued care following the prior request for therapy cessation did not extend past 2 additional visits. Again, the patient opted out of therapy following the second returning visit and did not return again. Co-management began with another trial of therapy within the acupuncture clinic, a consult with a local maxillofacial surgeon, and imaging centering around the palate in the form of a 3D Cone Scan.
DISCUSSION
Clinical Rationale
Due to the unique nature of the presenting complaint, available literature was reviewed to determine therapeutic conduct. Literature regarding the treatment protocols for this specific complaint is lacking; therefore, obtainable research was compiled to formulate a clinical rationale. Low-level laser therapy (LLLT) was administered across the aforementioned sites largely with the intention of minimizing patient pain.14,16 However, the plausibility for the intervention to reduce sympathetic inclusion, decrease any neurologic association, and/or initiate tissue healing within the oral cavity was also a motivation.16,19 Chiropractic manipulative therapy was administered across the upper cervical segments of C1-C3 with the intention of reducing any potential contribution from the upper cervical nerve roots that ultimately lend fibers to the trigeminal nucleus and pterygopalatine ganglion, as illustrated in reports of trigeminal neuralgia management through chiropractic interventions being beneficial. The plausibility of chiropractic manipulative therapy being successful towards pain reduction of any trigeminal neuralgia largely stems from the likelihood of chiropractic manipulation separating the cervical lateral canals to further relieve any vertebral pressure contributing to the first three cervical nerve roots.12,13,19 A series of other manual therapies over the craniofacial region were also incorporated into the management of this case. Sustained manual shearing of the Sagittal Suture was conducted with contacts over either side of the parietal and frontal bones of the cranium. Additionally, the utilization of a chiropractic Activator tool was applied across the aspects of the frontal and maxillary sinuses bilaterally, along with manual, digital, mobilizations over those contacts. The aim of these manual therapies was to presumably mobilize the surrounding bony and soft tissue structures across the aforementioned complexes with a focus to decrease any potential pain contribution from sympathetic or parasympathetic influences across the craniofacial anatomy.20–27 Combining all of the subsequent interventions was aimed to limit the neurologic inclusion of the palatine nerves across the hard-palate and decrease the pain severity and frequency over the course of care.
Outcome Analysis
Following the consideration of both outcome assessments at the initial encounter, goals were established. These goals included decreasing the pain within the oral cavity from an 8/10 on average to a 6/10 regarding the NPRS, and to decrease the dysfunction scores within the PSFS from an 8/10 to a 7/10; also, decreasing the amount of pain via direct contact over the area of complaint and discomfort from hot/cold foods or beverages on the PSFS questionnaire all over the course of the 4-week care plan.
The NPRS was chosen over other pain assessments such as the visual analog scale (VAS) for a few reasons; largely for its ease-of-use when being administered upon each encounter regarding the patient’s oral complaint and simple interpretation regarding the statistical data. It is also as sensitive as the VAS when interpreting the quantitative standards; simultaneously, there have been less failure rates regarding the NPRS over the VAS due to higher incidences of both patients and clinicians misunderstanding the usage and interpretation of the outcome itself.21
The nature of the patient’s presenting complaint was not directly relevant to most outcome assessments within our outpatient facility; therefore, the Patient-Specific Functional Scale was ultimately rendered. The PSFS allowed us to generate specific patient activities or qualities that were directly precise to the aspects of this unique complaint. The PSFS remained relevant throughout this case and has been shown to be both a valid and reliable outcome amongst older populations.22 Both the NPRS and PSFS were re-administered at the conclusion of the prescribed care plan to determine patient progression and/or if changes to the overall management plan were warranted.
In order to quantitatively validate our patient’s progression and comprehensively analyze the administered outcome assessments, the determined numerical values and elicited goals needed to be statistically compared to the MCID provided for each outcome assessment tool. The MCID is a numerical value that is used alongside respective outcome assessment tools to quantitatively show if a patient is progressing beneficially at a clinical minimum. Meaning, most outcome assessment tools are tied to a specific numerical value determined by the MCID to illustrate a patient’s progression, if any. For example, the NPRS is correlated to an MCID value between 1 and 223,24; therefore, the patient would have to give a value of at least 1 point less on the 0-10 scale to quantitatively show that he or she has received therapeutic benefit at the most minimal level. The same is true with respect for the PSFS; yielding an MCID value of 2 points.25,26 For our clinical case, the average values of 8/10 for each outcome assessment were later decreased to a 6/10 within each assessment at the reassessment date, giving clinically important difference of 25% regarding the exhibiting pain and discomfort of the presented complaint. This documented decrease of 25% concerning the utilized outcomes satisfied the MCID values for each respective outcome. With the outcome statistics being compiled, our clinical and quantitative goals were ultimately met. The 25% decrease in the patient’s symptomology lends to the notion that the administered interventions can be therapeutically beneficial for such an atypical complaint presentation. However, despite the quantitative reduction in the patient’s presentation, his satisfaction towards progression was not achieved, and he later opted to discontinue therapy.
Limitations
The described benefits to this case may not be analogous to other presentations regarding oral or hard-palate symptomology. The unique nature of this complaint may prove to be challenging when administering the described interventions within this case to other similar presentations. Furthermore, the atypical presentation of the patient’s condition gave rise to a more intuitive management of the suspected diagnosis as specific evidence is lacking with regards to chiropractic management. Simultaneously, the greatest attribution to the patient’s improvement cannot be definitively stated due to the complexity of the presenting complaint and the theoretical application of the given interventions. Largely, the greatest limitation experienced throughout was a substantial lack of published literature regarding the nature of this complaint and therapies to be applied to lessen the presenting deficits. Our aim was to try and fill this void within the literature by demonstrating the clinical avenues taken and the rationales for each when going about therapy for this complaint. Subsequently, it is understood that many more studies regarding examination, diagnosis, and therapy pertaining to such a presentation will need to be conducted in the future to better evaluate the relationships between chiropractic interventions and oral neuralgias.
CONCLUSION
This case report presented the approaches to the diagnosis of chronic, atypical, greater palatine neuralgia regarding the hard-palate. Following a 5-week course of chiropractic interventions including, chiropractic manipulative therapy, manual craniofacial therapies, nutritional supplementation, and low-level laser therapy, a 25% reduction in the elicited pain and dysfunction was later determined. Quantitative goals were achieved, however patient satisfaction was not attained. The patient opted to conclude therapy following the 5-week course of care, but later returned to our outpatient facility after 3 weeks of therapy cessation to continue the previously administered interventions.
Funding Sources and Conflicts of Interest
No funding sources or conflicts of interest were reported for this study.