INTRODUCTION
Chronic musculoskeletal pain is prevalent among military veterans and is associated with significant health care utilization and high treatment costs.1–4 A recent systematic review found that 31% (95% CI, 34-57%) of veterans live with chronic pain, which is 1.5 times higher than the rate of chronic pain in the general civilian population.5,6 Chronic low back pain, in particular, is a leading cause of disability within the Department of Veterans Affairs (VA), affecting 25% of veterans.7
Despite high rates of health care utilization, a 2021 survey of 701 Canadian veterans living with chronic pain (45% response rate) found that only 33% were somewhat (27%) or very satisfied (6%) with their care.8 Moreover, studies assessing veterans’ treatment preferences for managing chronic musculoskeletal pain are lacking.4 Evidence suggests there may be a disconnect between treatments for chronic low back pain preferred by veterans, and those preferred by health care providers. In a 2021 study involving veterans with chronic low back pain and primary care providers from 5 VA medical centers in the US,4 veterans ranked massage, physical therapy, and chiropractic care as their most preferred treatment options. In comparison, primary care providers ranked physical therapy, medications (i.e., analgesics, muscle relaxants, and adjuvants such as anti-depressants or anti-convulsant drugs), and psychological therapies (e.g., cognitive behavioral therapy, acceptance-commitment therapy, or mindfulness training) as their most preferred treatment approaches.4 This suggests an opportunity to better align treatment preferences of patients with management by health care providers, which has been shown to improve outcomes.9,10
In the aforementioned 2021 survey of Canadian veterans,8 optimization of chronic pain management after release from the military was identified as a top research priority. The Chronic Pain Centre of Excellence for Canadian Veterans (CPCoE) was launched in April 2020 to support chronic pain research relevant to Canadian veterans.11 The mandate of the CPCoE is to build a knowledge transfer system with other institutions and community-based clinics, train and educate interdisciplinary healthcare teams, and develop evidence-based therapeutic strategies to improve pain management services for veterans living with chronic pain.
Aim
In collaboration with the CPCoE, the aim of our study is to examine Canadian military veterans’ use and preferences toward specific health care disciplines and treatment approaches for the management of chronic low back pain. Our findings will inform the design of future studies to optimize low back pain services to veterans and military personnel.
Hypothesis
We hypothesize that veterans living with chronic low back pain will report varying levels of use and preference toward health care disciplines and treatment approaches for managing chronic low back pain.
METHODS
Registration
Our study protocol was registered with the Open Science Framework (OSF) on January 12, 2023 and updated on February 6, 2023 (https://osf.io/pru92).
Study Design
We will use a convergent, mixed-methods study design,12 in which quantitative and qualitative (open-text) data are collected and analyzed concurrently. Both sets of data will be compared and combined (i.e., ‘triangulated’) to obtain a richer understanding of our cross-sectional survey findings.12
Data Collection Methods
We developed a 33-item English- and French-language questionnaire containing 24 multiple choice questions, 8 questions with response options on a Likert scale (i.e., 0 = “no pain/no disability”, 10 = “worst pain possible/complete disability”), and 3 open-ended questions (Appendix 1). The first part of the survey focuses on demographical and military-related variables, while the second asks about chronic low back pain characteristics, accessibility of low back pain services in the military, and personal experiences and attitudes toward health care disciplines and treatment approaches for the management of chronic low back pain. The survey was created by a team of epidemiologists, research methodologists and chronic pain experts, and was piloted by 2 veterans living with chronic low back pain for clarity and comprehensiveness, and to determine the time required for completion.13 We modified wording and structure of 2 questions (Question #'s 4 and 26) based on their feedback.
Sample Characteristics
Eligibility criteria
Eligible participants are Canadian military veterans living with chronic low back pain, defined as low back pain on most days or every day over the past 6 months.14 Two screening questions pertaining to military veteran status and chronic low back pain will be asked to confirm eligibility. Participants whose answers are contrary to any of the inclusion criteria aspects will be excluded and receive an exit prompt on the questionnaire.
Sample size and rationale
Our targeted sample size will be 300 veterans living with chronic low back pain. We believe that responses from 300 veterans will provide sufficient feedback to allow the 12 treatment approaches/health care disciplines presented in our survey to be ranked from most to least preferred. This number of responses should also allow us to adequately describe the demographic characteristics of our sample. Based on a previous survey with this study population,8 we expect a response proportion of approximately 23%. However, our sampling frame will include the entire population of CPCoE military veteran members (n = 1,681) to ensure that our sample size will be large enough to address our main objectives.
Survey Administration
An invitation to participate in the survey will be sent to all 1,681 Canadian Armed Forces veterans who have signed up to support chronic pain research with the CPCoE for Canadian Veterans.11 The invitation for participation letter will be sent via the veterans’ e-mail addresses and will explicitly detail the intent of the survey. Those that do not agree to participate will not be sent the survey but will still be included in the denominator for the calculation of the survey’s response rate. Those that agree to participate will be asked if they wish to complete the survey in English or French, and online or by hard-copy. Once a language choice is provided, participants will receive an e-mail containing a link to access the online questionnaire in their language of choice, built using LimeSurvey (LimeSurvey GmbH, Hamburg, Germany).
For participants that request a hard-copy of the survey, a paper-based version will be mailed to them along with a return envelope with pre-paid postage. If it is necessary to fax the survey, it will be faxed electronically to the participant using RingCentral (RingCentral Inc, Belmont, California, U.S.), and will come with a toll-free fax return number to return completed surveys. Both the faxed and electronic version of the survey will contain a disclosure letter that provides details on the intent of the study. Upon completion of the survey, participants can voluntarily declare whether or not they would like to receive the results of the study.
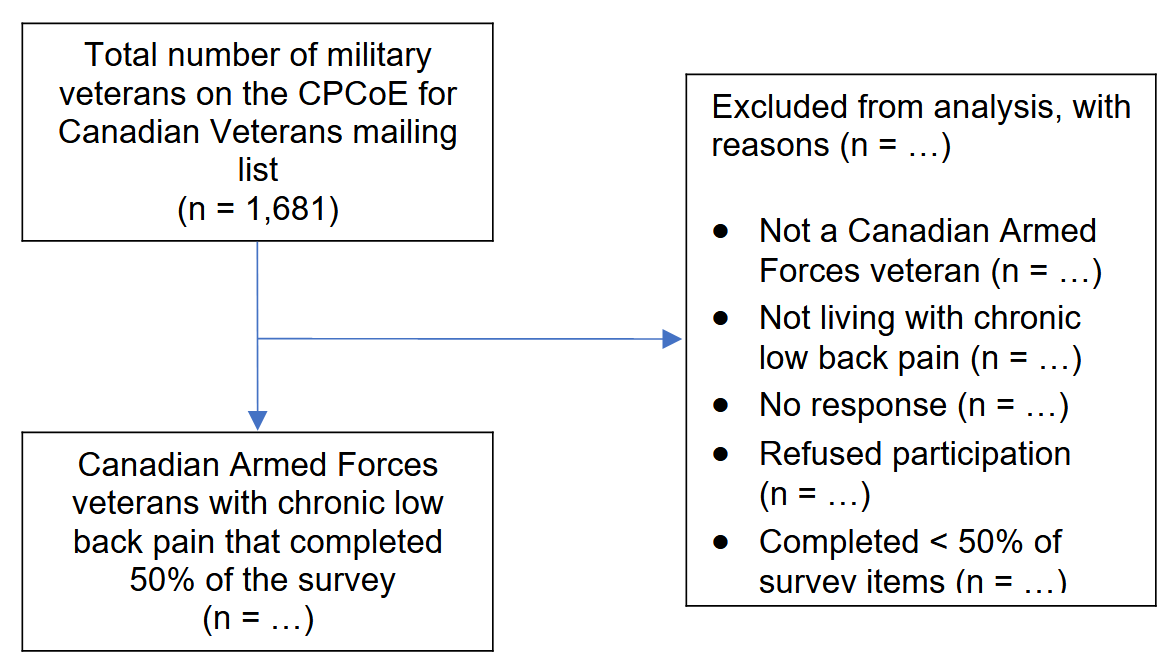
Two reminder e-mails will be sent to participants after periods of 4 and 8 weeks from the start date of survey distribution, after which the participants will no longer be contacted. Participants will have from mid-February 2023 to end of May 2023 to complete the survey. We will enable LimeSurvey’s online “cookie” feature to prevent repeated participation of respondents. A flow diagram of our survey administration is provided in Figure 1.
.png)
Figure 1.Survey administration (CPCoE = Chronic Pain Centre of Excellence).
Ethical Considerations
The Hamilton Integrated Research Ethics Board at McMaster University waived an ethics review for our survey based on its research development nature.15 All survey responses collected in this study will be reported as aggregate data without any participant identifiers.
Statistical Analysis
Measured variables
Participants will be asked to report a number of demographic characteristics, as well as military- and chronic low back pain-related variables (see Appendix 1, Question #‘s 1 to 25 and 27 to 32). We will also measure the mean ranking of veterans’ preference for each health care discipline for management of low back pain (Appendix 1, Question #26). In order to create this variable, each preference ranking for a given health care discipline will be assigned a number from 1 to 12 in descending order of preference. For example, a ranking of “1” corresponds to “most preferred” while a ranking of “12” corresponds to “least preferred.” Then, for each healthcare discipline the responses will be added up and divided by the total number of responses to retrieve a mean preference ranking. In addition, we will calculate the proportion of times that each health care discipline has been given a top-3 ranking (i.e., rank #1, 2 or 3), and the proportion of times that each healthcare discipline has been given a bottom-3 ranking (i.e., rank #10, 11 or 12). This will be determined by collapsing the above 12 preference rankings into 4 ordinal categories (1 = ranking #'s 1 to 3; 2 = ranking #'s 4 to 6; 3 = ranking #'s 7 to 9; 4 = ranking #'s 10 to 12), and then counting the number of times each health care discipline has been given the corresponding designation and dividing by the total number of responses per category. Participants will also be asked 2 open-ended questions about why they ranked their top and bottom 3 choices as their most and least preferred health care disciplines, respectively.
Primary analysis
All data will be populated into a de-identified Microsoft Excel database and organized for effective data analysis. Frequencies will be generated for all collected data. Categorical variables will be presented as frequency and percentage. Continuous variables will be presented as mean and standard deviation when normally distributed, and median and inter-quartile range when not. Listed health care disciplines (Appendix 1, Question #26) will be ranked in order of most to least preferred based on mean/median endorsement (Table 1). Categorical rankings of health care disciplines will also be displayed graphically with bar charts. All data analyses will be performed using SPSS V.28.0.1.0 (IBM SPSS Statistics).
Table 1.Canadian military veterans’ attitudes toward specific health care providers for the management of chronic low back pain
| Health Care Discipline |
Mean (SD)/Median (IQR) Preference Ranking a |
Overall Top 3 Ranking
n (%) |
Overall Bottom 3 Ranking
n (%) |
| 1. Family doctor |
X |
X |
X |
| 2. Physiatrist b
|
X |
X |
X |
| 3. Orthopedic surgeon |
X |
X |
X |
| 4. Neurosurgeon |
X |
X |
X |
| 5. Nurse |
X |
X |
X |
| 6. Physiotherapist |
X |
X |
X |
| 7. Chiropractor |
X |
X |
X |
| 8. Occupational therapist |
X |
X |
X |
| 9. Registered massage therapist |
X |
X |
X |
| 10. Acupuncturist/TCM practitioner |
X |
X |
X |
| 11. Mental health professional (e.g., psychologist) |
X |
X |
X |
IQR = inter-quartile range, SD = standard deviation, TCM = Traditional Chinese Medicine.
a The central tendency and measure of spread (i.e., SD or IQR) will depend on the data distribution.
b A physiatrist is a physician specializing in physical medicine and rehabilitation.
Thematic analysis
A thematic analysis12 will be conducted on the open-ended response questions (Appendix 1, Question #'s 26 and 33). Two independent reviewers will evaluate written responses and a coding strategy will be developed through discussion. We expect that after several rounds of coding written comments, clusters of sub-themes under themes will emerge. We will only code sub-themes that appear in at least 2 surveys. Any disagreements will be resolved through discussion to establish consensus. Illustrative quotes will be selected from the open-ended responses, guided by a consensus on informativeness and representativeness among the reviewers (Table 2).
Table 2.Summary of thematic analysis findings from open-ended survey responses
| Theme a |
Sub-Themes a |
No. of Endorsements |
Exemplary Quotation |
| Question #26: Top 3 choices for most preferred health care discipline (n = …) |
| X |
X
X
X |
X
X
X |
X
X
X |
| X |
X
X
X |
X
X
X |
X
X
X |
| Question #26: Bottom 3 choices for most preferred health care discipline (n = …) |
| X |
X
X
X |
X
X
X |
X
X
X |
| X |
X
X
X |
X
X
X |
X
X
X |
| Question #33: Final survey comments (n = …) |
| X |
X
X
X |
X
X
X |
X
X
X |
| X |
X
X
X |
X
X
X |
X
X
X |
a The number of themes and sub-themes displayed in Table 2 are for illustrative purposes and will be determined following data analysis.
Mixed methods analysis
Our quantitative and qualitative results will be integrated using joint display (Table 3), contiguous narrative, and weaving approaches.16 We will use the qualitative findings to illuminate the statistical findings from the survey, and draw upon both sets of data to come to a set of conclusions (i.e., ‘meta-inferences’).12
Table 3.Joint display of quantitative and qualitative survey results
| Variable |
Quantitative Results |
Representative Quotations |
Meta-Inferences |
| 1. X (n = …) |
X |
X |
X |
| 2. X (n = …) |
X |
X |
X |
| 3. X (n = …) |
X |
X |
X |
| Etc. |
X |
X |
X |
Missing data
Questionnaires with > 50% missing data (i.e., $\geq \ $17 items) will be omitted from all analyses.8
Reporting
We have reported our study protocol, and will report our final results, in accordance with the Checklist for Reporting of Survey Studies (CROSS)17 and the Good Reporting of A Mixed Methods Study (GRAMMS) guidelines.18
DISCUSSION
This will be the first study to conduct a mixed-methods, needs assessment survey on Canadian veterans’ experiences and attitudes toward health care providers and treatment approaches for the management of chronic low back pain. Our findings will inform the design of future studies to optimize low back pain services to veterans and military personnel. Of particular relevance to the chiropractic profession, we will also seek to determine whether our sample of Canadian veterans had previous access to chiropractic care while in the military; whether they used such services and, if so, what their experiences were; and whether they feel chiropractic care should be available at military bases for actively serving members of the Canadian Armed Forces.
Chiropractic services were first included in the US military health care system in 1995, beginning as a 5-year feasibility and health services evaluation project at 13 military bases.19 In 2000, the development of permanent chiropractic services and benefits for uniformed service members was approved by US Congress, and chiropractic services are now provided at more than 60 US military facilities across the country.19 There is evidence from several studies to support the inclusion of chiropractic care in the US military health care system.20–22 In 2 recent randomized controlled trials involving active-duty military personnel,21,22 those receiving chiropractic care and usual medical care showed statistically significant greater improvements in low back pain intensity,21,22 function,21,22 strength,22 endurance,22 satisfaction,21,22 and analgesic use21 compared to those allocated to usual medical care alone. There is preliminary evidence supporting inclusion of chiropractic services in the Canadian Forces Health Services delivery system.23,24 At present, however, chiropractors cannot become commissioned officers in Canada, there are no chiropractic services available on any military base in Canada, and the Canadian Armed Forces currently reimburse approximately $1 million CAD/year for service members, who have received authorization from an on-base physician, to travel off-base to receive chiropractic care (personal communication, Dr. Markus Besemann, Head of Rehabilitation Medicine, Canadian Forces Health Services).25
Strengths and Limitations
Strengths of our study include pre-testing of our survey questionnaire, providing our survey in Canada’s two official languages (English and French), use of both closed- and open-ended response options, integrating our quantitative and qualitative datasets in a mixed methods design, and reminders to potential participants to increase our survey response rate. Our study will also have limitations. First, our sample will not include former members of the Royal Canadian Mounted Police, who are also veterans. Second, our survey participants will be veterans that have expressed an interest in research and a willingness to be included in a mailing list maintained by the CPCoE for Canadian Veterans which may introduce selection bias. Third, we do not query survey participants about whether they are seeking, or have been granted, disability benefits for low back pain, which could influence responses. Last, there may be a lower participant response to the qualitative (open-text) questions in our survey because participants will already be asked to answer several items in the quantitative portion of the questionnaire.
Knowledge Translation
The results of our survey will be disseminated via a peer-reviewed publication and conference presentations, and provided on the CPCoE website.
Role of the Funding Source
The Chronic Pain Centre of Excellence for Canadian Veterans had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; or decision to submit the manuscript for publication.
Conflict of Interest
The authors have no conflicts of interest to declare.
Acknowledgements
The authors wish to thank Drs. Christine Goertz, Robert Kerns, Anthony Lisi, Markus Besemann and Graeme McBride, as well as the CPCoE for their feedback and assistance in designing the survey instrument for this study.
Disclaimer
This study was funded by the Chronic Pain Centre of Excellence for Canadian Veterans. Dr. Emary is a postdoctoral fellow in the Michael G. DeGroote National Pain Centre at McMaster University and is supported by research grants from the NCMIC Foundation and the Canadian Chiropractic Research Foundation outside of the submitted work. Dr. Busse is supported, in part, by a Canadian Institutes of Health Research Canada Research Chair in the prevention and management of chronic pain. All authors have no competing interests to declare.
Appendix 1. Copy of the English version of the survey instrument.
Treatment Preferences of Canadian Military Veterans living with Chronic Low Back Pain
[Insert date]
Dear [First Name],
The Chronic Pain Centre of Excellence (CPCoE) for Canadian Veterans is working with Dr. Peter Emary, a postdoctoral research fellow under the supervision of Dr. Jason Busse, Director of Research for the CPCoE. In collaboration with the CPCoE, a study is being conducted on Canadian Veterans’ use and preferences toward health care providers and treatment approaches for the management of chronic low back pain.
This study will be used to make recommendations to health care providers and to help researchers design studies on providing better low back pain services to military personnel.
Following this cover page is a 33-question survey which should take between 15 to 20 minutes to complete. These questions are based on previous research of Veterans living with chronic low back pain, as well as feedback from Canadian Veterans and chronic pain experts. Prior to the actual survey, there are two questions to assess your eligibility for completing the survey.
If you have any questions or concerns at any point regarding the survey, please contact Peter Emary through e-mail at emaryp@mcmaster.ca.
Thank you very much for your time and assistance.
Sincerely,
Peter Emary, DC, PhD
Postdoctoral Fellow, Michael G. DeGroote National Pain Centre
McMaster University
Screening Questions
We would like to first ask you two questions to determine your eligibility for completing the survey.
- Have you previously served in the Canadian Armed Forces?
Yes
No
II. Do you currently live with chronic low back pain?
Chronic low back pain is defined as low back pain on most days or every day over the past 6 months.
Yes
No
Demographic Questions
1. What is your gender?
□ Female
□ Male
□ Other: _____________________________
□Prefer not to answer
2. What is your age?
□18 to 24
□25 to 34
□35 to 44
□45 to 54
□55 to 64
□65+
3. What branch(s) of the military did you serve in (check all that apply)?
□Royal Canadian Navy
□Canadian Army
□Royal Canadian Air Force
□Canadian Special Operations Forces Command
□Other: _____________________________
4. What was your final rank in the military?
□Officer
□ Warrant Officers Petty Officer and Senior Non-Commissioned Officer
□Junior Non-Commissioned Member
□Other: _____________________________
5. What component(s) of the military were you a part of?
□Regular Force
□Primary Reserve
□Primary Reserve – Cadet Organizations Administration and Training Service
□Primary Reserve – Canadian Rangers
□Other: _____________________________
6. Which of the following best describes the primary focus of your occupational specialty (*) in the military?
□ Operational or Combat-related
□ Operational support (i.e., Non-operational or non-combat related positions that assisted operational or combat-related forces to deliver their mission)
□ Institutional support (i.e., Non-operational or non-combat related positions that were not involved in assisting operational or combat-related forces directly; e.g., base/wing positions, support for educational institutions)
□ Other: _____________________________
* What was your specific trade? (e.g., infanteer, IT technician, medical assistant, combat engineer, etc.)
___________________________________
7. How many years did you serve in the military?
□ Less than 5 years
□ 5 to 10 years
□ 11 to 15 years
□ 16 to 20 years
□ 21 to 25 years
□ 26 to 30 years
□ More than 30 years
8. How many years has it been since you released from the military?
□ Less than 5 years
□ 5 to 10 years
□ 11 to 15 years
□ 16 to 20 years
□ More than 20 years
9. What was your province or territory of residence at the time of release from the military?
□ Ontario
□ Manitoba
□ Quebec
□ Nova Scotia
□ New Brunswick
□ Prince Edward Island
□ Newfoundland and Labrador
□ Saskatchewan
□ Alberta
□ British Columbia
□ Yukon
□ Northwest Territories
□ Nunavut
□ Other: _____________________________
10. What is your current province or territory of residence?
□ Ontario
□ Manitoba
□ Quebec
□ Nova Scotia
□ New Brunswick
□ Prince Edward Island
□ Newfoundland and Labrador
□ Saskatchewan
□ Alberta
□ British Columbia
□ Yukon
□ Northwest Territories
□ Nunavut
□ Other: _____________________________
11. What best describes your current region of residence?
□ Urban (in the city)
□ Rural (in the country)
□ Suburban (mixed-use or residential area, existing either as part of a city area or as a separate residential community within commuting distance of a city)
□ Other: _____________________________
12. What best describes your current gross income level?
□ Below $25,000
□ $25,000 to $49,000
□ $50,000 to $59,000
□ $60,000 to $79,000
□ $80,000 to $99,000
□ $100,000 to $150,000
□ More than $150,000
□ Prefer not to answer
13. Which of the following best describes your race or ethnicity?
□ Asian – East (e.g., Chinese, Japanese, Korean)
□ Asian – South (e.g., Indian, Pakistani, Sri Lankan, Indo-Caribbean/West Indian)
□ Asian – Southeast (e.g., Malaysian, Filipino, Vietnamese, Cambodian)
□ Asian – West (e.g., Afghan, Israeli, Saudi Arabian, Iranian, Turkish)
□ Australasian – (e.g., Australia, New Zealand, New Guinea, Melanesia)
□ Black – Africa (e.g., Ghanaian, Kenyan, Somali)
□ Black – North America
□ Black – Caribbean Region (e.g., Barbadian, Jamaican)
□ Hispanic
□ Indigenous (e.g., Inuit, First Nations, Non-Status Indian, Metis, Indigenous person from outside Canada)
□ Latin American (e.g., Argentinean, Chilean, Salvadoran)
□ White/European (e.g., English, Italian, Portuguese, Russian)
□ Prefer not to answer
□ Do not know
□ Other: _____________________________
14. What is your highest formal education level?
□ High School
□ College Degree
□ University Degree
□ Other: _____________________________
15. What best describes your current relationship status?
□ Single/Never Married
□ Married
□ Common law
□ Separated
□ Divorced
□ Widowed
□ Chronic Low Back Pain Section
The following questions seek to understand when your chronic low back pain originated, how much it impacts your day-to-day life, what treatments you have received and are currently using for your chronic low back pain, which health care providers you prefer to see for treatment of your chronic low back pain, what treatments were available to you while serving in the military, and if you feel other treatments may have been helpful.
There are no right or wrong answers. Please answer based on your own experiences and opinions.
- Impact of chronic low back pain
16. How many years have you lived with chronic low back pain?
□ 6 months to 1 year
□ 1+ to 5 years
□ 5+ to 10 years
□ 10+ to 20 years
□ 20+ years
17. Over the past week, on average, how would you rate your chronic low back pain?
No pain Worst pain possible
0 1 2 3 4 5 6 7 8 9 10
18. Over the past week, how much has your chronic low back pain interfered with your daily activities (housework, washing, dressing, walking, climbing stairs, getting in/out of bed/chair)?
No interference Unable to carry out activity
0 1 2 3 4 5 6 7 8 9 10
19. Over the past week, how much has your chronic low back pain interfered with your ability to take part in recreational, social, and family activities?
No interference Unable to carry out activity
0 1 2 3 4 5 6 7 8 9 10
20. Over the past week, how anxious (tense, uptight, irritable, difficulty in concentrating/relaxing) have you been feeling?
Not at all anxious Extremely anxious
0 1 2 3 4 5 6 7 8 9 10
21. Over the past week, how depressed (down-in-the-dumps, sad, in low spirits, pessimistic, unhappy) have you been feeling?
Not at all depressed Extremely depressed
0 1 2 3 4 5 6 7 8 9 10
22. Over the past week, how have you felt your work (both inside and outside the home) has affected (or would affect) your chronic low back pain?
Have made it no worse Have made it much worse
0 1 2 3 4 5 6 7 8 9 10
23. Over the past week, how much have you been able to control (reduce/help) your chronic low back pain on your own?
Completely control it No control whatsoever
0 1 2 3 4 5 6 7 8 9 10
B. Treatments and health care providers used (or currently using) for chronic low back pain
24. Which of the following treatments have you received, at any time, for your chronic low back pain? (choose all that apply):
Over-the-counter medications:
► Examples: Tylenol, Advil □ tried in the past □ currently using
Opioid medications:
► Examples: Codeine, morphine, hydromorphone, tramadol □ tried in the past □ currently using
Adjuvant medications:
► Examples: Anti-depressants (e.g., duloxetine, amitriptyline), anti-
seizure drugs (e.g., lamotrigine, gabapentin, carbamazepine) □ tried in the past □ currently using
Non-steroidal anti-inflammatory drugs (NSAIDs):
► Examples: Naproxen, celecoxib □ tried in the past □ currently using
Topical agents:
► Examples: Capsaicin, lidocaine □ tried in the past □ currently using
Muscle relaxants:
► Examples: Baclofen, tizanidine □ tried in the past □ currently using
Cannabis:
► Examples: Inhaled, oral □ tried in the past □ currently using
Injections or other interventional procedures:
► Examples: Nerve blocks, epidural or corticosteroid injections, muscle/trigger point injections (e.g., lidocaine, botox), ultrasound infusion/administration of medications (e.g., lidocaine, ketamine), nerve denervation (e.g., radiofrequency ablation) □ tried in the past □ currently using
Low back surgery:
► Examples: Spinal laminectomy, discectomy, foraminotomy,
nucleoplasty, spinal fusion, artificial disc replacement □ tried in the past □ currently using
Physiotherapy:
► Examples: Exercise therapy, stretching/mobilization, traction, TENS
(Transcutaneous electrical nerve stimulation), low-level laser therapy, therapeutic ultrasound □ tried in the past □ currently using
Chiropractic care:
► Examples: Spinal manipulation/ “adjustment”, flexion-distraction therapy (i.e., spinal decompression/manual traction), soft-tissue massage/stretching, advice on exercise/ergonomics □ tried in the past □ currently using
Psychotherapy:
► Examples: Pain neuroscience education program/chronic pain management course, family or group therapy, cognitive-behavioural therapy (individual or group), acceptance and commitment therapy, mind-body therapy (e.g., mindfulness/meditation), biofeedback □ tried in the past □ currently using
Complementary and alternative medicine (choose all that apply):
Naturopathic treatment/homeopathic remedies: □ tried in the past □ currently using
Acupuncture: □ tried in the past □ currently using
Registered massage therapy: □ tried in the past □ currently using
Osteopathy: □ tried in the past □ currently using
Other: _____________________________ □ tried in the past □ currently using
Other treatment(s) not covered above: _____________________________ □ tried in the past □ currently using
□ Not applicable (I have never received treatment for my chronic low back pain)
25. Which health care providers have you seen for your chronic low back pain, at any time? (check all that apply):
□ Family doctor
On a scale of 0-10, how satisfied were you with the care provided? ___ (0 = not at all satisfied, 10 = completely satisfied)
□ Physiatrist (a physician specializing in physical medicine and rehabilitation)
On a scale of 0-10, how satisfied were you with the care provided? ___ (0 = not at all satisfied, 10 = completely satisfied)
□ Orthopedic surgeon
On a scale of 0-10, how satisfied were you with the care provided? ___ (0 = not at all satisfied, 10 = completely satisfied)
□ Neurosurgeon
On a scale of 0-10, how satisfied were you with the care provided? ___ (0 = not at all satisfied, 10 = completely satisfied)
□ Nurse
On a scale of 0-10, how satisfied were you with the care provided? ___ (0 = not at all satisfied, 10 = completely satisfied)
□ Physiotherapist
On a scale of 0-10, how satisfied were you with the care provided? ___ (0 = not at all satisfied, 10 = completely satisfied)
□ Chiropractor
On a scale of 0-10, how satisfied were you with the care provided? ___ (0 = not at all satisfied, 10 = completely satisfied)
□ Occupational therapist
On a scale of 0-10, how satisfied were you with the care provided? ___ (0 = not at all satisfied, 10 = completely satisfied)
□ Registered massage therapist
On a scale of 0-10, how satisfied were you with the care provided? ___ (0 = not at all satisfied, 10 = completely satisfied)
□ Acupuncturist/Traditional Chinese Medicine practitioner
On a scale of 0-10, how satisfied were you with the care provided? ___ (0 = not at all satisfied, 10 = completely satisfied)
□ Mental health professional (e.g., psychologist)
On a scale of 0-10, how satisfied were you with the care provided? ___ (0 = not at all satisfied, 10 = completely satisfied)
□ Others (please list): _____________________________
On a scale of 0-10, how satisfied were you with the care provided? ___ (0 = not at all satisfied, 10 = completely satisfied)
□ Not applicable (I have never seen a health care provider for my chronic low back pain)
C. Attitudes toward specific health care providers for chronic low back pain
26. Which health care providers do you most prefer to see for treatment of your chronic low back pain? (1 = most preferred, 12 = least preferred):
(1) Family doctor □ (1-12)
(2) Physiatrist (a physician specializing in physical medicine and rehabilitation) □ (1-12)
(3) Orthopedic surgeon □ (1-12)
(4) Neurosurgeon □ (1-12)
(5) Nurse □ (1-12)
(6) Physiotherapist □ (1-12)
(7) Chiropractor □ (1-12)
(8) Occupational therapist □ (1-12)
(9) Registered massage therapist □ (1-12)
(10) Acupuncturist/Traditional Chinese Medicine practitioner □ (1-12)
(11) Mental health professional (e.g., psychologist) □ (1-12)
(12) Others (please list): _____________________________ □ (1-12)
□ Not applicable
► For your top 3 choices above (i.e., those you rated as being #1, 2 and 3), can you explain why you most prefer to see these health care providers for treatment of your chronic low back pain?
► For your bottom 3 choices above (i.e., those you rated as being #10, 11 and 12), can you explain why you least prefer to see these health care providers for treatment of your chronic low back pain?
D. Accessibility of low back pain services in the military
27. When during your military career did you begin experiencing low back pain?
□ Before military service
□ During military service
□ After military service
28. During your military service, which health care providers did you see on base for low back pain treatment? (check all that apply):
□ Not applicable (I did not experience low back pain while in the military)
□ Family doctor
□ Physiatrist (a physician specializing in physical medicine and rehabilitation)
□ Orthopedic surgeon
□ Neurosurgeon
□ Nurse
□ Physiotherapist
□ Chiropractor
□ Occupational therapist
□ Registered massage therapist
□ Acupuncturist/Traditional Chinese Medicine practitioner
□ Mental health professional (e.g., psychologist)
□ Others (please list): _____________________________
29. During your military service, which health care providers did you see off-base for low back pain treatment? (check all that apply):
□ Not applicable (I did not experience low back pain while in the military)
□ Family doctor
□ Physiatrist (a physician specializing in physical medicine and rehabilitation)
□ Orthopedic surgeon
□ Neurosurgeon
□ Nurse
□ Physiotherapist
□ Chiropractor
□ Occupational therapist
□ Registered massage therapist
□ Acupuncturist/Traditional Chinese Medicine practitioner
□ Mental health professional (e.g., psychologist)
□ Others (please list): _____________________________
30. Which health care providers do you believe should be available on base for low back pain treatment? (check all that apply):
□ Family doctor
□ Physiatrist (a physician specializing in physical medicine and rehabilitation)
□ Orthopedic surgeon
□ Neurosurgeon
□ Nurse
□ Physiotherapist
□ Chiropractor
□ Occupational therapist
□ Registered massage therapist
□ Acupuncturist/Traditional Chinese Medicine practitioner
□ Mental health professional (e.g., psychologist)
□ Others (please list): _____________________________
31. Do you feel that your low back pain, when it first started, was treated effectively?
□ Yes □ No □ Unsure
32. Do you feel that more treatment options or better access to care when your low back pain first started may have prevented it from becoming chronic?
□ Yes □ No □ Unsure
E. Final comments
33. Are there any other comments you would like to share regarding your experiences with managing your chronic low back pain?
_____________________________
End of Survey
Thank you for your time!
If you have any further questions, please contact Dr. Peter Emary at: emaryp@mcmaster.ca