
Introduction
Having a robust evidence base that is derived from high-quality research is imperative for professions within modern healthcare systems. The establishment of research agendas that codify priorities can assist healthcare professionals in evaluating and prioritizing the appropriate allocation of limited research resources.1 Whilst formal chiropractic research agendas have been established in North America and Europe,2–10 a comprehensive research agenda has not been formulated within the Australian context, although the need was identified well over a decade ago.11 A critical precursor informing the development of any such Australian chiropractic research agenda was the identification of the priorities held by practitioners, academics, and researchers along with an appraisal of research capacity and output of the Australian chiropractic profession.
Stakeholders and Funders
In Australia, several key stakeholders fund research in the chiropractic profession and some have published research agendas, strategies, and priorities. The Australian Chiropractors Association (ACA) is the largest funder of capacity building. It funds Chiropractic tertiary education, postgraduate and undergraduate scholarships, and research projects in Australia providing over $AUD3.3 million (updated funding total November 2022. To the best of our knowledge, totals were correct as of that time) since 2009.12 Other significant funders are the Australian Spinal Research Foundation (ASRF) ($AUD 891,229)13 and Chiropractic Australia (CA) through its Research Foundation (CARF)14 ($AUD 364,218).15 Of these organizations, the ACA published a detailed Research Summary and Strategic Research Opportunities in 2016,16 ASRF published a formal research agenda17 and CA has outlined a high-level description of research goals and general aspirational statements.18 ACA and ASRF update details of the research they fund in annual reports, newsletters and media releases.
Aims
The primary aims of this study were (a) to identify and compare the research priorities of Australian practicing chiropractors and academics across listed research domains, and (b) to seek their views on existing chiropractic research strategies. Concurrent objectives were to (i) collect survey-based data using a mixed-methods study design, (ii) analyse and synthesize the data so as to gain insight into the perspectives toward research, capacity for research activity and output, and funding secured by academics and researchers, and (iii) make recommendations for future research.
Methods
A detailed description of our aims and methods been previously published.15 The survey instrument was developed via an iterative process that initially built upon an exhaustive search of the chiropractic research priority literature from which items were aggregated and distilled. Senior clinicians, academics, and researchers in the chiropractic field were also consulted to identify further items that should be considered for inclusion and to pilot test the survey.
The study used a mixed-method research (MMR) design19–23 and collected data using an online survey portal24 reported in accordance with mixed-methods reporting guidelines.25 The theoretical framework of the study is best described as a convergent mixed-methods design within an advocacy/participatory construct.19 This type of research may facilitate an action agenda for reform where it provides a voice for participants and a space for debate and discussion to facilitate change.26 The convergent design is the most common and well-known MMR design, and was previously known as the ‘concurrent triangulation design’.27
The finalized questionnaire was a self-administered multi-dimensional instrument comprising 5 main research categories. These domains were: basic science; conditions; sub-groups; interventions; and public health/health services. In addition, the questionnaire included items such as research funding, support for existing research agendas, and provided scope for suggestions for future research and comments in open text boxes. The survey also explored research output, barriers, time allocation, engagement perspectives, interdisciplinary collaboration, and research funding secured by academics and researchers. The survey was emailed to practicing Australian chiropractors who were members of the Australian Chiropractic Research Network (ACORN), a practice-based research network database (n=1680) and to academic/researchers employed at 4 Australian university-based chiropractic programs (n=220) in early 2019. We used the STROBE cross-sectional checklist to inform the project.28
Participants were invited to provide descriptive commentary and suggestions in text boxes at the end of each main section of the survey, with responses coded using content analysis. Both quantitative and qualitative methods were implemented during the same timeframe and with equal weight, the purpose being to obtain different but complementary data on the same topic. The intent was to bring together the differing strengths of quantitative methods (sample size, trends, generalization) with those of qualitative methods (details and deeper perspectives). This design was used since we wanted to directly integrate, compare and contrast quantitative statistical results with qualitative findings.29
Data analysis
Data were analyzed both quantitatively and qualitatively using standard methods and reported25 in accordance with mixed-methods reporting guidelines.24 Data were exported from the SurveyMonkeyTM platform into SPSS (V.24) for cleaning and statistical analysis. Required responses throughout the priorities section ensured minimal missing data and multiple responses from single participants were broadly managed using the de-duplication procedure for online surveys as described by Konstan et al.30 The integration and interpretation of data occurred simultaneously and with equal weighting during analysis after the close of the data gathering phase.25
Quantitative analysis
Participants were described by demographic characteristics using means and standard deviation (SD). Categorical data were descriptively analysed using frequency distributions and percentages, and continuous data analysed using the median and interquartile range (IQR) as data were not normally distributed. Differences between groups (academics vs. practitioners) in Likert scale responses (e.g., perceived research funding and resource allocation priorities) were assessed using the independent samples Mann-Whitney U Test. Comparisons of research priorities were tabulated based upon listed principal domains, sub-domain items and research-related areas and initiatives support for the chiropractic research strategies and priorities identified by listed chiropractic professional organizations. We used a Bland-Altman scatter plot to report agreement as a graphical method to compare mean differences (at 95% CI)31,32 where the differences between groups are plotted.31,33
Qualitative analysis
The free-text data were primarily analyzed via semantic coding34 and verbatim referential units in cases where the category was an exact match for the textual data. Content analysis allowed respondents to the survey to add relevant information which was not otherwise contained by categorical survey questions. In addition, content analysis would allow for the identification of other related domains which could be explored by future research in this area. Themes arising from the content analysis were intended to provide a more complete picture and enrich the interpretation of quantitative results. For the conventional content analysis, all open-text responses were initially read and coded under the survey domain headings in Microsoft Excel (Redmond, WA, USA). Conventional and summative content analyses of the qualitative data as described by Hseih and Shannon were undertaken by 2 researchers independently and then cross-checked by a third researcher.
The main purpose of collecting qualitative data in this survey was to identify surface-level details which broadened the scope beyond the quantitative categorical response format of the survey items and identifying additional domains of interest for future researchers to explore. In this sense, it is a descriptive content analysis rather than an interpretive thematic analysis. Discrepancies were resolved by mutual discussion until consensus was achieved.35
Results
The results are presented initially as the quantitative results covering the sample demographics, followed by the quantitative results, with reference to similarities and differences. The primary goal was for the quantitative data to offer insights, while the secondary goal was to determine if the qualitative results supported the quantitative results or not, thereby creating either convergence or separation for each measured domain.
The response rate from full time equivalent (FTE) academics was 44%, for casuals and part-time chiropractic academics 8%, and for ACORN database chiropractic practitioners, 21.5%.
Of the organizations listed, in our sample the Australian Chiropractors Association (ACA) was represented by 48.5% of academics and 73.2% of practitioners. The converse was true for Chiropractic Australia (CA) membership with 72.7% of academics and 21.8% of practitioners. The Australian Spinal Research Foundation (ASRF) had no academics and 26.8% of practitioners as members. 12.1% of academics and 8.5% of practitioners reported not being members of any of these organizations.36–38
Demographics and Membership
Practitioner participants were predominantly male (64.3%), mean age of 46±12.6 years and had been in chiropractic clinical practice for a mean duration of 20 years. Most were practicing in NSW or Victoria (53.2%) with participants from every Australian state and territory except the Northern Territory. Academics reported being in academia for a mean period of 13 years and had completed post-graduate study for 5 years. Most academic respondents (73%) held level A or B appointments, (i.e., Tutor/Associate Lecturer/Research Associate, Level B - Lecturer/Research Fellow), 36% were involved in clinical supervision, and 33% were concurrently in private clinical practice.
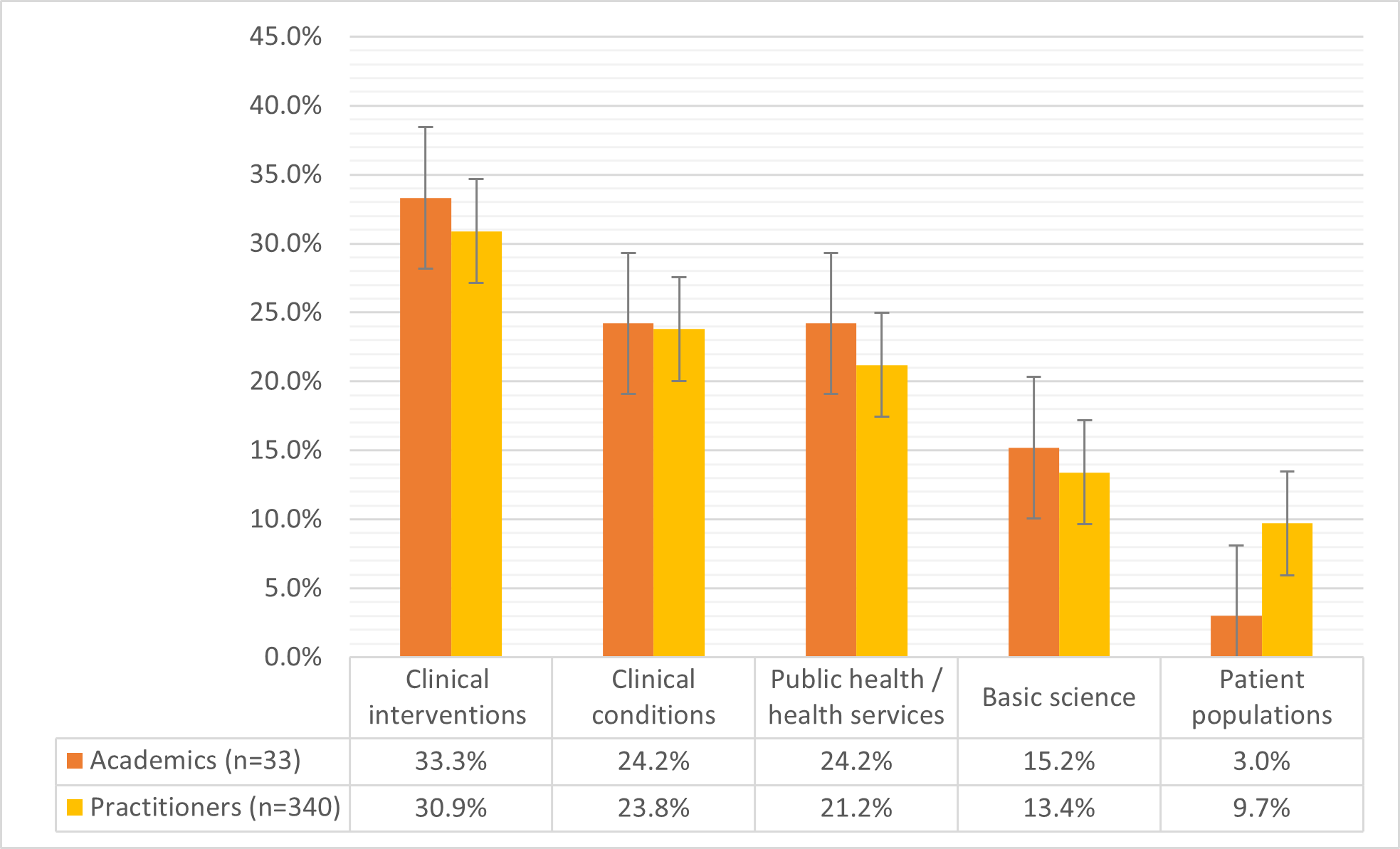
Domain item priorities
Quantitatively, there was broad agreement between the two groups across the majority (>90%) of domain items.36–38 The closest agreement and highest rankings were achieved for the ‘Clinical Interventions and Practice’ and ‘Conditions’ domains (Figure 1).

Quantitative disagreement was only observed within 2 specific domain items being patient sub-groups (infants) and chiropractic-specific techniques (Figure 2). Disagreement occurred outside of the main domains, including research agenda support and funding.

Open-text data comprised a narrower focus on musculoskeletal (MSK) conditions and opposition or reservations by academics and some practitioners toward the research agenda of those espousing traditional Chiropractic concepts and terminology.
Some practitioners were highly critical of the narrow focus and epistemological paradigm of Australian university-based research using students to provide interventions.
“Given that we are busy trying to emulate the gold standard of medical research when a lot of that has been found to be false or corrupt, I am not a great fan. It appears that the more research that is conducted the more we find that what we do doesn’t work and yet people still flock to chiropractors for the results that they obtain. Seems like we are looking in the wrong place. It irks me that research that shows that chiropractic has mediocre results was performed by chiropractic students.” (Practitioner 19)
Practitioners were ambivalent toward the traditional focus of the Australian Spinal Research Foundation and some also of the Chiropractic Australia Research Foundation.38
“I’ve been an ASRF donor and member for more than 25 years. I’m saddened by the decline in the Foundation in recent years. I don’t support CA’s research approach because of its narrow scope of focus on pain syndromes.” (Practitioner 100)
“ASRF should support high quality spinal research, but in reality, promotes dangerous outdated chiropractic dogma placing practitioners’ income over patients’ best interest.” (Practitioner 5)
Comments from both groups illustrate the strongly held views that characterise divergent factions of the profession. Some practitioners were also highly critical of Australian university-based research. Academics were of the view that MSK and spinal pain, for which some evidence already exists should be the priority of future research by chiropractors, building on what is known. Conversely, practitioners were of the view that future research should be directed across more areas, such as younger populations, basic science and non-MSK conditions.
“Our best research is in low back pain. We need to focus on neck pain and headaches now.” (Academic 8)
“I would like us to focus for the short term on being the masters of musculoskeletal medicine, whilst still not forgetting our roots and building a basis to be able to adequately defend our more philosophical roots.” (Practitioner 244)
“The vast majority of Australians would struggle to believe that a baby could be born with anything other than a perfect spine! A good study on the incident rates of poor neck motion or posture in infants… would go a long way to giving justification for assessing and managing spine problems in babies.” (Practitioner 177)
Responsibility to Fund Research
Both groups quantitatively agreed that professional associations, the Australian Spinal Research Foundation (ASRF), Chiropractic Australia Research Foundation (CARF), and universities with chiropractic programs all had a responsibility to allocate funding and resources to support chiropractic research. While 72.7% of academics agreed it was the responsibility of the ASRF to fund research, this was countered by the finding that 70% of academics strongly reject the research priorities and strategies of the ASRF.36 Both groups agreed that the Australian Spinal Research Foundation (ASRF) and Chiropractic Australia Research Foundation (CARF) have a responsibility to allocate funding and resources to support research.
Some practitioners however disagreed that their membership organizations should be substantial funders of research since they have other roles to fulfil;
“The ACA perform many functions that require funds, so I don’t expect all their money to go towards research at the expense of advocacy and member services. Field practitioners who are members are already paying for this contribution so shouldn’t have to fund further research themselves unless they wish to by way of contributing to a research organisation or program like ACORN.” (Practitioner 245)
Perspectives Toward Research
There were significant differences between academics and practitioners with respect to statements regarding traditional chiropractic terminology such as ‘subluxation’ and ‘philosophy’, journals, professional independence and MSK research. Practitioners were more supportive of traditional perspectives than academics for these concepts.
“Biomechanical dysfunction must include detailed examination also of the soft tissues - myofascial trigger points, Chiropractic subluxation must be placed in historical context and properly redefined using words such as “dysarthria” etc. Much work to be done yet.” (Academic 30)
“I find it an interesting bias that a survey of chiropractors for chiropractors’ research interest doesn’t mention the word subluxation until the final series of questions. I would be concerned if this survey is used by what Villanueva-Russell describes as educational elites shifting the milieu of the academic and research directions away from what the majority of practitioners in the field do in practice.” (Practitioner 210)
Publication Output
Of academics, 39.4% reported publishing between 1-5 papers (average <1 per year) in the preceding 5 years while around a quarter reported not publishing any. Around 65% of academics had published <1 paper/year. Only 2 academics reported publishing over 20 papers in the previous 5 years while 3 practitioners reported publishing 20 or more papers in the same time frame. Just under 9% of field practitioners reported they had published a scientific paper in the last 5 years. Similar patterns were reported for books and scientific conferences. Case studies were the type most published by practitioners.
“I would submit more case studies if I knew of a platform where they would be useful and integrated into the evidence base.” (Practitioner 117)
Barriers and Time Devoted to Research
Academics reported spending, on average, 25% of their time on research while practitioners reported 7%. Of academics reporting no publications in the last 5 years, nearly 20% reported spending a significant proportion of time currently engaged in research. Both groups reported a desire to spend significantly more time on research. Time and financial support were reported as the greatest barriers to research activity. Multiple practitioners expressed interest in being involved in research and publication and the desire for direction and assistance.
“I would happily write case studies on patients if I had some sort of template or guidance as to how to go about it correctly.” (Practitioner 284)
Collaboration and Funding
The majority of academics reported not having secured any funding for research with 3 academics reporting having secured Category 1 (NHMRC) funding in the preceding 5 years. The 2 most reported sources of secured funding were university funding and category 3. Of academics, just over quarter reported self-funding their research.
In this mixed-methods study we found convergence of the quantitative and qualitative results across many of the domains measured, be they agreement or disagreement between the two groups measured.
Discussion
This is the 5th paper in a series describing and reporting the results of a survey of Australian chiropractors, practitioners, academics, and researchers and contains a summary of results previously reported in detail. The mixed-method design of this study unearthed many valuable insights. Readers will note we previously published quantitative and qualitative data separately that indicate there is more agreement than disagreement, with a core cluster of agreed topics, between academics and practitioners with respect to their priorities for future research topics and perspectives.36–38 If one were to rely solely on quantitative results however, one could conclude the two groups were effectively congruent. It is only when the voices of both groups are heard via the open text data that the challenges of developing a truly collegial research agenda in any roadmap for the future become apparent. The divergence evident among the various sectors of the profession has been well described for many years and the qualitative data confirm that these divisions show little sign of fading. That said, the core agreements could be areas of negotiation and compromise, for which there is seemingly good scope. When contemplating reasons for the observed differences, we previously noted that academics would be expected to have a greater grasp of the complexities of research, the limitations, and challenges inherent in obtaining funding, and what research already exists. Practitioners who are not researchers are not expected to deeply appreciate these issues. On the other hand, practitioners are concerned about people they encounter in everyday practice leading to their prioritization of future research in more categories than academics.36
Funders of Australian Research on Chiropractic Topics
We previously identified a small number of organizations that support and fund chiropractic research in Australia. Their efforts appear fragmented and divided, lacking collegiality and sometimes transparency. There is clearly scope for cooperation between chiropractic research funding organizations and optimization of research activity to generate and implement a consensus research agenda. If a compromise and consensus research agenda were achieved, then ASRF funding may become acceptable to academics since, over the 45 years of its existence, the organization has funded over 250 projects worth in excess of AUD$2.8 million.39 Academics seeking scarce funds may consider the benefits of collegiality to access this resource. Any agenda should be duty-bound to align with the needs and evolution of the chiropractic profession and the community’s health priorities within a modern healthcare landscape. Naturally, individual organizations identify and allocate research funding based on their own discretion. The results of this study suggest that Australian chiropractic research organizations and researchers could at least interact, tolerate, and cooperate to identify and develop a workable research agenda. Research on topics of value and meaning to the chiropractic profession has value in the context of the broader public health landscape given the features of the burden of disease among people who consult chiropractors.40,41 Such a research agenda would ipso facto, include research related to primary health, the sector in which chiropractic is embedded. A common research agenda would thus, depend on the appetite for cooperation among all stakeholders.
Capacity and Output
The average publication rate per year for Australian chiropractic academics in the PubMed database has previously been found to be low when compared to other health disciplines.42,43 No studies have previously recorded publication data for field practitioners in Australia. Thus, the assumption may have been that research output across the entire chiropractic profession was also low. This is the first time the publication output and capacity, indeed the interest and desire to participate in research among Australian field practitioners has been investigated. Unfortunately, among academics, there was little improvement since 2013 when the average yearly publication rate for academics was reported as 0.62.42
We identified questions over scarce resource allocation which ostensibly warrant attention by heads of university programs given some academics reported no publications in the previous 5 years, while, by their own description, spending significant time engaged in research. It is possible the discrepancy in the response to this question could lie partially in the estrangement of the 2 concepts of ‘time for research’ and ‘research output/publications,’ where time assured for research activity in job descriptions do not correlate with actual research activity. It is possible that academics, in their reporting, have revealed an uncoupling of these two concepts in their daily work.44 In any event, if matching of ‘time for research’ and ‘research output’ among academics is the goal, then changes in workload and work allocation may need to occur at a management level.
It appears there are a small number of ‘high performers’ in terms of output among academics lifting the overall publication metrics. Interestingly, several field practitioners reported publishing as many papers (<20) as the higher performing academics, however we did not record journal rankings of these publications. This concentration of publications among a small proportion of authors is not unique to the chiropractic profession. Broadly, scientific publishing exhibits a significant distribution gap where 75% of scientists produce only one or two papers in their lifetime, contributing to a quarter of all published papers. A tiny fraction, the top 1.2% of scientists, prolifically produce over 50 papers, making up a quarter of all scientific publications.45–47
We note the emergence of new ‘players’ in the chiropractic educational and research space in Australia. The monopoly of chiropractic education in Australia by the 4 universities is currently being challenged by the privately operated Australian Chiropractic College (ACC) based in Adelaide, South Australia.48 Recently there has also been an emergence of a ‘hub’ for post-graduate doctoral research of chiropractors at Southern Cross University which does not currently have a chiropractic program.49
Practitioners as clinician researchers
Around 9% of field practitioners reported publishing a scientific paper although journal ranking (quality) was not quantified. This would appear to be a potential resource that could be accessed to facilitate increased future output, possibly in collaboration with unpublished and underperforming academics. Engagement and capacity building is ostensibly possible for the ‘pool’ of practitioners who have indicated an interest in research to participate in ‘research as a hobby’. Participation could improve overall capacity and open pathways other than clinical practice for the ‘clinician researcher’.50,51
Journals, Conferences and Symposia
Currently Australasia has 2 journals supported by member organizations, CA and ACA. Of these, (Chiropractic and Manual Therapies) is Quartile 1 (top 25%), Medline listed.52 The Chiropractic Journal of Australia has had somewhat of a checkered history, narrowly escaping being defunded in the recent past and has seen its Scopus listing slip to Quartile 4 in recent years.53 Recently a new journal has appeared in the region, The Asia Pacific Chiropractic Journal (Asia-Pac J Chiropr). It has focussed on case-studies, and contributions from field practitioners and serves as a forum for disseminating traditional Chiropractic dialogue, describing itself as 'The friendly home of chiropractic clinical science for the world’s Quiet Chiropractors’.54 In our study we noted passionately held views by academics, and some practitioners, toward ‘organization supported’ journals reflecting their personal allegiances. Each of the membership organizations and the ACC conduct annual scientific conferences and symposia. Some of our respondents reflected on the challenges of motivating practitioners to attend these events in their current forms, serving as a salutary signal to member organizations.
An Australasian Conference?
While collating data for this study we found it a challenge to locate credible sources to allow triangulation [the use of multiple methods or data sources in qualitative research to develop a comprehensive understanding of phenomena22], for example of research output and funding. While we have previously recommended convening an Australian Chiropractic-related Research Agenda Conference (36 37), we are mindful of the challenges inherent in attempting this. An ‘umbrella’ agenda that can be agreed upon by the divergent groups within the profession would be difficult to achieve. Broadly speaking these groups are demarcated by (1) Spinal pain/MSK focus; rejection of traditional chiropractic specific nomenclature; restricted scope; and strict adherence to a fairly narrow definition of ‘(MSK) evidence-based practice’. (2) Wellness/well-being focus beyond spinal pain; acceptance of traditional chiropractic nomenclature/concepts; broad scope; ‘evidence informed (N-MSK)’; willing to consider all levels of evidence whilst placing relatively greater emphasis on practitioner experience; and patient needs/values. Such a conference to garner broad agreement and collaboration would be an ideal aspiration, however, this may be akin to achieving a unified field theory.
A Research(ers) Register and Resource
A more pragmatic achievable aspiration than a common research agenda may be establishing an international chiropractic focussed research database register and repository. This could initially be at least conceptually modelled along similar lines to the existing Physiotherapy Evidence Base (PEDro)55 which is based at the University of Sydney in collaboration with Neuroscience Research Australia (NeuRA).
The PEDro Partnership ‘functions as a non-profit organization to facilitate evidence-based physiotherapy through consultation with professional organizations, purchasers of physiotherapy services, providers, registration and licensing authorities, teaching programs, and consumer groups’.55 Such a resource could store researcher profiles including output, funding secured, rate evidence, and even connect researchers and funders among many other functions. Resources exist that could be aggregated, adapted, and expanded to include these aspects to facilitate more efficiency in the chiropractic research and education space.56–58 In our view, such a resource would be best situated within an institution or the World Federation of Chiropractic (WFC) and funded and logistically supported internationally by member organizations. A recent initiative that is relevant to acknowledge that could contribute is the emergence of the Chiropractic Educators Research Forum (CERF).59 CERF is “A place for chiropractic educators to engage in research and the scholarship of discovery, integration, application, teaching, and engagement”. Its mission is “To build scholarship and research capacity for chiropractic educators throughout the world.”
Developing such a resource we suggest may even require convening an International Chiropractic Research Agenda Conference (‘I CRAC’). Notwithstanding, we recognize the challenges of convening such a conference given the fractured political landscape in the profession. Such an initiative must include all stakeholders such as regulators, educational institutions, accreditors, professional organizations, practitioners, and research funders. Ideally also included would be other stakeholders such as practitioners, chiropractic students, consumers, insurers, third-party payers, health system administrators, and possibly government and health departments. In a ‘post-COVID-19’ world, such physical conferences may become less commonplace, and the process may be ‘virtual’ or ‘hybrid’. Advances in technology facilitate the use of a modified Delphi type process over multiple stages which may be informed by data such as those been presented in this series of papers.
This project was conducted as a sub-study within the ACORN-PBRN. The ACORN-PBRN project continued producing legacy publications even after the cessation of funding by ACA in 2016, albeit in a greatly diminished capacity. The energy and commitment of the 2,005 chiropractors who completed the original baseline survey and the 1,680 chiropractors who joined the network provided a solid platform for the development of substantial chiropractic research initiatives and extensive chiropractic research capacity building across Australia and beyond. The ACORN-PBRN generated at least 25 peer-reviewed manuscripts and many more scientific conference presentations which covered a broad range of topics that served to describe many characteristics of the profession and people who consult chiropractors in Australia.15,36–38,41,60–73 Rejuvenated funding of a similar PBRN would facilitate further development of future initiatives. These could include the creation of a ‘collegial’ community of researchers that transcends institutions and practice paradigms. Such a community could provide an inclusive and unifying platform to facilitate exploration of innovative and creative features toward the aspiration of production of high-quality evidence within the chiropractic space.
A comprehensive research register, or repository would serve to facilitate connections between individual researchers potentially decreasing duplication and unproductive competition. Existing resources provide models that may be useful such as The PEDro Partnership (The Physiotherapy Evidence Database),74 Manual Alternative and Natural Therapy Index System (MANTIS),58 Chiro.org - Chiropractic Resource Organization75 and the Chiropractic Educators Research Forum (CERF).76 As the bodies representing chiropractors in Australasia, the leadership of the ACA, CA, and New Zealand Chiropractors’ Association (NZCA) are well placed to collaborate on these initiatives within WFC at modest cost.
Summary of Insights and Recommendations
-
Further research in the form of deeper engagement with each stakeholder group possibly using qualitative methods such as focus groups is needed to delve more deeply into the issues identified in this project.
-
There are few recognized chiropractic organizations that fund research in Australia, and cooperation and consensus between these organizations regarding research strategy is lacking.
-
Communication and cooperation between funding organizations should be encouraged and facilitated to promote and enable meaningful research that can be easily translated to inform clinical practice.
-
The overlap in research priorities encountered within the chiropractic profession, considering all stakeholders, should be identified and ear-marked for implementation within the context of the primary care setting of the chiropractic profession.
-
Those academics who are keen to been engaged with research, and the programs within which they are embedded, could be encouraged to re-distribute their time and activities to include research activity where there is a proportionate relationship between time and (research) activity/output. This is a workforce planning and workload allocation issue.
-
Engagement and capacity building is possible for the large pool of practitioners who have indicated an interest in research to engage in ‘research as a hobby’. Participation could improve overall capacity and open pathways other than clinical practice for the ‘clinician researcher’.
-
Convene a recurring Australian (or Australian-Aotearoan (NZ)-SE Asian-Oceania) research agenda conference to include all stakeholders such as regulators, educational institutions, accreditors, professional organizations, practitioners, research funders, chiropractic students, consumers, insurers, third-party payers, health system administrators, and possibly government and health departments. In the emerging era of health service task substitution, chiropractic research could facilitate the expansion of chiropractic service delivery in the primary care sector.
-
Fund the continuation or future iteration of the ACORN-PBRN in future phases of development to allow maturation of the resource.
-
Construct an international chiropractic focused research database register and repository under the auspices of the World Federation of Chiropractic (WFC) within an existing institution of higher learning.
-
Accreditors could facilitate reporting of research output by requiring regular reporting to a central database by institutions as a condition of accreditation.
Limitations
This is the first study to examine research priorities from the perspectives of Australian chiropractic academics, researchers, and practitioners, and we have acknowledged the limitations in the series of papers arising from the project, especially in relation to the qualitative data.
The survey, while informed by other studies and although pilot-tested by people who were not part of the dataset or research team, was not a validated instrument. Practitioner input was limited to members of the Australian Chiropractic Research Network (ACORN) thus practitioner participants may have different perspectives and research interests to non-respondents and to the wider profession. The ACORN database of practitioners was aging and had not been updated due to the expiry of funding by the ACA in 2016. The findings are also limited due to non-response bias from part-time and casual academics. Since the response rates are not representative, we cannot generalize how valid the collected data are to the wider profession.77
There are a number of other limitations [described detail in previous papers36–38] particularly in the richness of qualitative data that were collected using open-ended survey questions rather than other qualitative methods such as in-depth interviews or focus groups. These methods were beyond the scope of this unfunded study. We have presented transparency of the design, sampling, data collection and analysis of individual components across the series of papers15,36–38 in the hope of stimulating discussion and constructive considered debate around the recommendations we offer.
Conclusion
Our study used a mixed-methods research approach and identified agreement and differences in the priorities and perspectives toward research among Australian chiropractors that precipitated multiple recommendations to address research gaps. The principal recommendations are 1) the development of a comprehensive chiropractic-relevant Australian research agenda and 2) an international chiropractic research register database. Such initiatives should incorporate input and reflect the needs and concerns of a wide range of key stakeholders including (but not limited to) regulators, educational institutions, accreditors, professional organizations, chiropractic students, practitioners, and research funders. Ideally also included would be external stakeholders such as consumers, insurers, third-party payers, health system administrators, and possibly government and health departments. Resources like these may help improve the quality and utility of evidence available to Australian chiropractors and thus translate into benefits for people who attend chiropractors.
Funding Statement
The Australian Chiropractors Association (ACA) formerly known as the Chiropractors’ Association of Australia (CAA) initially funded the ACORN project between 2013-2016. However, the funding source of the ACORN project had no influence on any aspect of the study. No funds were received specifically to conduct this study. The research reported in this study is the sole responsibility of the authors and reflects the independent ideas of the authors alone.
Patient consent
Not required.
Ethics approval
The study was approved by the Human Research Ethics Committee of the University of South Australia (UniSA Ethics Protocol #0000035553).