INTRODUCTION
Dizziness is a term used to describe many sensations such as vertigo, syncope, lightheadedness, and disequilibrium. All these terms are symptoms or descriptors and not definite diagnoses. Dizziness is a common complaint seen in clinical practice. In fact, it is the most common complaint that brings people aged 75 and above to see their primary care physician. Overall, dizziness is the 9th most common complaint.1–4 Unfortunately, treatment for dizziness is suboptimal within primary care, with a cohort study finding that almost half the participants had substantial dizziness-related impairment at 10-year follow-up from diagnosis.5 90% of patients with dizziness are given a non-specific diagnosis, leading to unnecessary prescriptions of betahistine and referral to an otolaryngologist.6
Though chiropractic practice has many anecdotal reports of patients having their dizziness improve under care, documented research is lacking. A review of the literature turns up 2 feasibility studies on chiropractic intervention on the outcomes of dizziness and just a few case studies.7–12 The purpose of this retrospective case series is to document the objective improvement in 8 patients with differing forms of dizziness while undergoing chiropractic intervention, including Orthospinology Upper Cervical chiropractic intervention and an individualized vestibular rehabilitation program. Pathophysiology will be examined and the mechanisms of how the interventions created favorable outcomes will be presented.
CASE REPORTS
This retrospective case series was reviewed and approved by the Life University Institutional Review Board as “exempt from full review,” per HHS policy for the protection of human research subjects. Informed consent was explained to each patient verbally and in written form, with their signed forms on file. Each of the 8 cases had chronic dizziness (≥3 months from onset). Cases 1-5 and 8 received their diagnosis from a neurologist, and case 6 from her primary care physician, before being seen at our clinic. Case 7 had been to a number of providers, including a neurologist, ear, nose, and throat (ENT) physician, and primary care physician before starting care at our clinic. He only received a non-specific diagnosis of “vertigo”. His case fits well into the Barany Society’s “Probable Meniere’s” diagnostic criteria; therefore, that is how we have classified him.13 Each filled out a comprehensive dizziness intake form and a Dizziness Handicap Inventory (DHI) prior to their initial examination. The DHI is an objective outcome assessment tool used to measure self-perceived handicap from dizziness.14 Each case completed a follow-up DHI after their initial 30-day trial of treatment. All 8 were physically examined with a bedside exam. This examination included physical vestibular and neurological testing such as eye movements, vestibulo-ocular reflex (VOR), cranial nerves, deep tendon reflexes, tactile sensations, and vital signs. Included in the bedside exam was the Orthospinology upper cervical physical evaluation. This included cervical palpation, supine leg-length inequality testing, standing hip-height discrepancy measurement, and standing posture evaluation to observe for head tilt, head rotation, shoulder-height discrepancy, and shifting of the lower neck on the trunk. Each case was also examined with computerized posturography and video-oculography (VOG) except cases 4 and 7 due to our clinic not having access to this equipment until after these 2 started treatment. All 8 cases had digital radiographs taken of their cervical spine. TABLE 1 summarizes the case examination data.
Cases 1,2,3,5,6, and 8 were given individualized vestibular and neurovisual rehabilitation exercises to practice. Interventional recommendations were based on the physical examination findings. For example, Case 1 had a left esophoria, and the eyes had a rightward slow drift when placed in darkness. Therefore, she was given recommendations to complete leftward horizontal pursuits, left X0 viewing, and rightward-only X1 vestibulo-ocular reflex exercises (VORs). These personalized strategies were used to target the examination finding versus simply giving the patient the standard recommendation of X1 bilateral VORs.
The Upper Cervical chiropractic analysis that was applied to each case was the Orthospinology Procedure. Upper Cervical is a subspecialty of chiropractic. It is based on the idea that improper structural alignment of the craniocervical junction (CCJ) leads to neurological disruption and that the precise re-alignment, or correction, reduces the misalignment, thus improving neurological function. The CCJ comprises the occiput, atlas, and axis, with their respective joints including the occipitoatlantal and atlantoaxial joints. We further examine this intervention in the discussion section of this article. The use of canalith repositioning maneuvers (CRM) was applied to cases 1,2,5,6, and 8 for reasons other than benign paroxysmal positional vertigo (BPPV) treatment. The purpose for this is also explained in the discussion section. Minor musculoskeletal soreness was reported after two cases received Orthospinology Upper Cervical chiropractic intervention resolving within 24 hours; however, no serious adverse events were rep
DISCUSSION
We will examine the 2 major topics of this case series and then summarize the treatment and outcomes in this section. The two topics to be discussed are 1) Craniocervical junction structural alignment and its relevance to dizziness, and 2) Performing canalith repositioning maneuvers for reasons other than BPPV intervention.
1.) Craniocervical Junction Structural Alignment and its Relevance to Dizziness
The craniocervical junction is a unique and sensitive region of the body. Both the structures and functions of the CCJ are particular to itself. For example, the occiput, atlas (C1), and axis (C2) comprise the hard tissue. The atlas and axis are uniquely shaped relative to all other spinal vertebrae. The occipitoatlantal joint connects the occiput to the atlas. It is responsible for 300 of total cervical flexion and extension.15 The atlantoaxial joint connects the atlas to the axis and is responsible for 500 of total cervical rotation.16 The considerable amount of mobility of these joints is at the cost of stability.17 The numerous amounts of soft tissue within the CCJ and its relevance to function are plentiful. It includes the occipital triangle of muscles: rectus capitus posterior minor, rectus capitus posterior major, obliquus capitus superior, and obliquus capitus inferior. The vertebral artery makes 4 900 turns within the CCJ and only 20% of cervical rotation and extension is enough to limit blood flow by constricting the lumen.16,18–20 It can also serve as a choke point for craniospinal hydrodynamics such as cerebral spinal fluid.21 The dentate ligaments provide a soft tissue attachment between the atlas and pia mater.22 The neurological significance of the region is plentiful. The suboccipital triangle contains over half of the mechanoreceptors in the entire cervical spine, and the rectus capitis posterior minor has a direct attachment to the dura mater.23,24
The symptoms of dizziness arising from a problem with the cervical spine is not a new concept and is also not without controversy. In fact, the first modern-era publication of “cervical vertigo” dates from 1945 in French Literature.25 In 2022, the Barany Society released a position paper stating that at this time they cannot make recommendations for or against the treatment or diagnosis of cervical dizziness due to a large lack of research.26 Saying this, we present 3 hypotheses that provide the greatest level of current evidence as to how structural malpositioning of the CCJ can lead to symptoms of dizziness. We will also discuss the structural realignment of the CCJ using an established Upper Cervical chiropractic technique and how this method could relieve these symptoms. We will use the 8 case examples in this paper to guide the discussion and bridge the gap between academia and clinical practice.
1.1.) Mechanoreceptive Dysafferentation
Of the 3 theories presented, mechanoreceptive dysafferentation holds the greatest level of evidence and is the most widely accepted theory. In the Barany Society’s position paper on cervical dizziness, they refer to this pathophysiology as The Somatosensory Input Hypothesis.26 The nervous system is composed of 3 functional categories: motor, sensory, and integration. The sensory portion contains peripheral sensors, proprioceptors. These receptors are found within tissues all throughout the body, relaying tactile sensations and position sense to the neuroaxis.
Mechanoreceptors are a group of proprioceptors that sense static and dynamic position sense of joints, tendons, and muscles. Mechanoreceptors are responsible for sensing body position relative to gravity. The muscle spindle mechanoreceptor provides the most clinical relevance here. Muscle spindles are in abundance within the suboccipital muscles. The central structure of the muscle spindle is composed of noncontractile intrafusal sensory fibers. These fibers are split into nuclear bag and nuclear chain fibers. The nuclear bag fibers contain large amounts of nuclei that exist in the central portion of the receptor. The nuclear chain fibers contain nuclei aligned in a chain all throughout the receptor. The annulospiral (primary afferent) and flower spray (secondary endings) are 2 sensory nerve endings found within the receptor area of the muscle spindle. These nerve endings respond to change in length to the receptor through both a static and dynamic response. Slow stretching of the receptor portion of the muscle spindle activates the static response. The number of impulses generated from the annulospiral and flower spray endings increase proportionally to the amount of stretch. The dynamic response activates when there is a sudden increase in the spindle receptor length. Stretching the nuclear bag structure activates the primary endings, resulting in a very powerful response relative to the static response. The tone of the extrafusal muscle is affected by the afferent input into the neuroaxis from these receptors due to changes in muscle length. The primary afferents synapse with the dorsal nucleus of the spinal cord and alpha motor neurons.
Gamma efferent fibers change the length of the extrafusal muscle fibers in response.23,24,27 The muscle spindle plays an important role in regulating movement and posture. They also have a responsibility to monitor and regulate joint position through the mechanism explained previously. A positional change of only 0.40in the upper cervical spine is sufficient to cause an increase in afferent discharge in articular mechanoreceptors.28 Normally, the afferents from other vestibular sensory anatomy such as the otolith organs and the semicircular canals would coincide with the afferents from the cervical proprioceptors.
However, a malpositioned craniocervical junction could cause improper cervical proprioceptive afferents to be generated and not match up with the other sensory anatomy. As stated earlier, the CCJ is a very mobile joint complex. Higher mobility is always at the cost of stability. If the complex were to become misaligned due to injury, it would cause an imbalance in intrafusal muscle receptor stretch. The imbalance would inappropriately lead to increased static afferents from the annulospiral and flower spray endings. The increased afferents when the head is at static neutral would not match the afferents generated by the semicircular canals and otolith organs, thus leading to a sensory mismatch, and resulting in sensations of dizziness. As observed in this case series, every patient presented with a structural malposition of their craniocervical junction of more than 0.40.
1.2.) Spinal Cord Tension
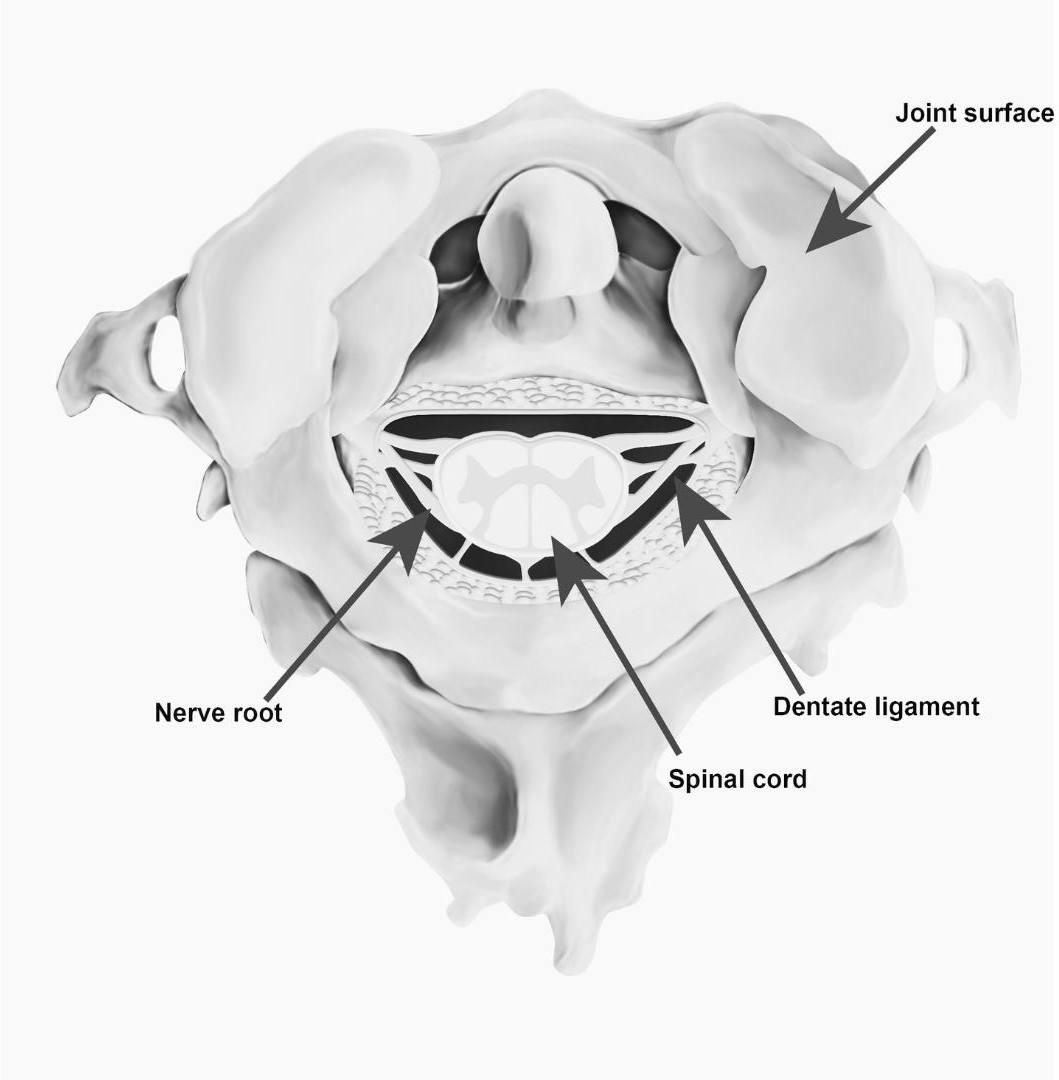
The spinal cord is directly attached to the foramen magnum, the second and third cervical vertebrae, the posterior longitudinal ligament, rectus capitus posterior minor, and through dural attachment to the periosteum of the atlas.29 There are 21 pairs of lateral connective tissue bands midway between the ventral and dorsal attachments of the nerve roots. These tissue bands are called the dentate ligaments (Fig. 1). Their medial connection is the pia mater of the spinal cord and lateral border is the dura mater. The more cephalad pairs are stronger and project more horizontally relative to their caudal counterparts. The dentate ligaments anchor the spinal cord onto the circumference of the foramen magnum to prevent the brainstem from being pulled through during cervical flexion.30 Grostic22 proposed 2 mechanisms how a misaligned CCJ can lead to neurological insult. The first is direct mechanical irritation of the nerves of the spinal cord. The second is venous congestion by vascular compression.

The dorsal spinocerebellar tract (DSCT) ascends on the lateral portion of the spinal cord. The DSCT relays proprioceptive afferents from the periphery to the ipsilateral cerebellum. Due to the DSCT’s anatomical location, it is the most vulnerable to mechanical irritation from inappropriate tension applied by the dentate ligaments. The small veins of the upper cervical spinal cord are scarce compared to other regions of the spine. Mechanical obstruction of these veins can cause stasis of blood and local ischemia. These veins move blood at a very low pressure which predisposes them to easy occlusion by compressive forces.22,30 Gillilan31 stated that the dentate ligaments may be a means of transmitting mechanical stress to the cord and resulting in small vein occlusion. Local ischemia by means of venous compression and direct mechanical tension on the DSCT are two theories as to how a CCJ misalignment may affect the normal proprioceptive afferents through the dentate ligaments causing spinal cord tension.
As stated above, the DSCT carries proprioceptive afferents from the periphery to the cerebellum for higher-order processing. The cerebellum corrects posture based on the information it receives from the DSCT. If the information is faulty due to the mechanism(s)
explained above, postural abnormalities may result. In our case series, every case had significant postural abnormalities.
1.3.) Craniospinal Hydrodynamic Dysfunction
The brain requires an uninterrupted inflow of arteriole blood, outflow of venous blood, and movement of cerebrospinal fluid for proper nerve function. An obstruction of arteriole blood flow can cause ischemia and result in death. A smaller restriction, whether functional or obstructive, can result in hypoperfusion of nerve tissue leading to decreased nerve function. In fact, Flammer32 discusses decreased optic nerve function as a result of non-obstructive, functional hypoperfusion of the optic nerve. The CCJ can act as a chokepoint for craniospinal hydrodynamics.
As stated earlier, the vertebral artery makes 4 900 turns within the CCJ. 16mm below the vertebrobasilar junction, the posterior inferior cerebellar artery (PICA) branches from the vertebral artery.33 The PICA supplies blood to the vestibular nuclei. As discussed previously, 20% of cervical rotation and extension is enough to restrict the lumen of the vertebral artery and result in decreased flow. Since the vertebral artery passes through the transverse foramen of the atlas vertebra, it is logical that improper transverse alignment of the atlas relative to the occiput and axis will predispose the artery to compression at less than 20% of cervical rotation and extension. This improper alignment could result in repeated moments of hypoperfusion from normal daily activities such as driving, personal hygiene, and even head position while sleeping. Of the 8 cases in our series, every case had a certain degree of misalignment of the atlas vertebra in the transverse plane. The misalignment ranged from 0.520 to as much as 3.810.
1.4.) Orthospinology Upper Cervical Chiropractic Intervention
Since its inception in 1895, the foundational invention in the chiropractic profession is high-velocity low amplitude spinal manipulation. Manipulation takes the joint into its paraphysiological space to apply and increase the motion of the restriction. The earliest reference to spinal manipulation was in 400 BCE.34 In 1931, BJ Palmer introduced a new spinal intervention concept, different from manipulation, called the Hole-In-One (HIO) technique. The idea was that the atlas vertebra could misalign relative to the occiput and axis and that a vectored, low-force, adjustment could restore the alignment. The patient’s head remained neutral and supported during the intervention; thus, the joint will never enter the paraphysiological space, meaning the intervention was not technically spinal manipulation.35 This new intervention was called Upper Cervical.
Later, John Grostic expanded on this area of study and practice, creating the Grostic Technique. Grostic was most concerned about inter-practitioner reliability of the HIO technique, so in 1938, he and colleagues formed the Palmer Standardized Chiropractors Council to provide a means to help standardize the methods at the time. Grostic began to x-ray the CCJ before and after applying a vectored force to it. This allowed him to research the structural realignment outcomes using different force vectors and patient head placement on the table. He also developed positioning equipment to be used during the x-ray examinations to eliminate patient placement errors that could result in false alignment measurements. The headpiece that he developed was designed to provide full support to the mastoid process, while he used his pisiform to administer the vectored force to the transverse process of the atlas to reduce the misalignment. In 1977, the Society of Chiropractic Orthospinology was formed as an advancement of the Grostic Technique. The largest contribution was by Dr. Cecil Laney with the development of a solenoid-driven instrument to apply the vectored force to the CCJ rather than using the chiropractor’s pisiform.35 Fig. 2 shows an example of an Orthospinology correction being administered with a solenoid-driving handheld instrument.

The Orthospinology technique detects a misalignment of the CCJ through physical and structural evaluation. If the doctor suspects that the patient may have a CCJ misalignment through the case history, they will begin with the physical evaluation. The physical evaluation consists of postural evaluation and palpation of the suboccipital muscles. The postural checks include measuring for leg-length inequality (LLI) while the patient is supine, measuring iliac crest heights relative to one another while the patient is standing, and observing the patient while he or she is standing for any head tilting, rotation, and shoulder height. All the posture checks have been clinically observed to reduce after administering the corrective force into the CCJ.36 In 1988, Dr. John F. Grostic’s son, John D. Grostic, researched the dentate ligament cord-distortion hypothesis to explain why this improvement was observed. He concluded that a misaligned CCJ can cause mechanical tension on the spinocerebellar nerve tract, resulting in postural distortions.21 Static palpation of the suboccipital muscles allows the doctor to assess for taught and tender fibers. Myofascitis can occur when joint mobility is restricted. Abnormal sensory input from the dysfunctional joint can result in reflexively activated trigger points.37 Taught and tender suboccipital muscles tend to relax immediately following the Orthospinology corrective force. Each of our cases had significant postural distortions and tender suboccipital musculature.
Once the doctor determines that the patient is showing physical signs of a CCJ misalignment, they will obtain radiographic imaging of the region. The first view obtained is the lateral cervical, which allows the doctor to view the CCJ in the sagittal plane. The sagittal angle of the atlas bone provides the x-ray tube set up for the following view. Next, the doctor takes a nasium view, which shows the CCJ in the coronal plane. Third, a vertex view is obtained to view the CCJ in the transverse plane. The doctor then measures the lateral tilting of the atlas bone relative to the center of the skull and the center of the C7 vertebrae, the rotation of the C2 vertebra, and the condylar and axial curvature measurement. Finally, the doctor measures the rotation of the atlas vertebra relative to the center of the skull on the vertex view. The measurements are calculated and provide a 3-dimensional correction factor to use as a vectored- force to reduce the misalignment of the CCJ. After the force is given, the doctor rechecks the initial postural and palpation findings for improvement. If not improved, the doctor may administer another corrective force. If improved, repeated nasium and vertex views will be obtained and re-measured to check for structural improvement.38
2) Performing Canalith Repositioning Maneuvers for Reasons Other Than BPPV Intervention
Benign Paroxysmal Positional Vertigo (BPPV) is one of the most common causes of vertigo, resulting in up to 2.5 million clinic visits in the United States per year.39 BPPV occurs when otoconia dislodge from the utricle macular bed and fall into a semicircular vestibular canal. The otoconia add mass to the endolymph, resulting in increased afferents when that canal is brought through its anatomical plane relative to gravity. A canalith repositioning maneuver (CRM), such as the Epley maneuver for posterior canalolithiasis, is exceptionally effective at resolving the associated vertigo.40
During the CRM for canalolithiasis, the patient’s head is moved through the affected canal’s anatomical plane while pausing every 900 to allow the otoconia to collect. The procedure ends when the head reaches the position where the otoconia moves out of the canal and into the vestibule.
The idea of using a CRM procedure for reasons other than BPPV intervention is not new. Neurologic Clinical Specialists (NCS) of the physical therapy profession and Diplomates of the American Chiropractic Neurology Board (DACNB) of the chiropractic profession have been using these procedures in non-BPPV cases with anecdotal reports.41 There are 2 mechanisms as to how a CRM procedure can aid in the recovery of dizziness and function in non-BPPV dizziness. The first is habituation, and the second is canal stimulation.
Habituation is the diminishing of a physical response through the use of repeated exposure to the antagonizing stimulus. Habituation has always been a key component of a comprehensive vestibular rehabilitation plan. Most recently, habituation was tested and found to be effective, using virtual reality gaming.42 The participants were “placed” in a visually stimulating racing environment through the game headset. Of our case series, there were multiple patients that experienced positional dizziness, but did not have accompanied nystagmus to indicate BPPV. We chose to bring those patients through the CRM procedure that’s onset caused the dizziness. For example, if lying on their left side caused them dizziness, we chose to bring them through a left Epley maneuver or left BBQ roll. An example of this is case 1. Case 1 had left-sided Meniere’s disease. Her history revealed dizziness sensations exacerbating with
left-sided vestibular stimulation and her physical examination confirmed this. We chose to perform CRM procedures of the left horizontal canal and left posterior canal for habituation. She reported less dizziness each session that we performed these maneuvers on her, and she showed objective improvement overall with her condition as viewed in the summary.
Canal stimulation is another key component of a quality vestibular rehabilitation plan. The foundational exercises of a vestibular rehabilitation plan are the vestibulo-ocular reflex (VOR) exercises.43 Though the purpose of the VOR exercise is for gaze stabilization, the first part of the reflex is canal stimulation to drive the afferents. Bringing the patient through a canal’s entire anatomical plane will stimulate the entire afferent potential of that canal.44 We chose to bring patients who had canal hypofunction through the respective CRM procedure to input and drive afferents. For example, case 5 showed reduced right posterior canal and right horizontal canal function during the physical examination. We chose to input and drive afferents to those canals using right-sided Epley maneuvers and right horizontal canal BBQ rolls.
3) Summary of Treatment and Outcomes
A review of the study data indicates that 4 cases had probable or definite Meniere’s Disease, 1 with post-concussion syndrome, 1 with generalized anxiety disorder, 1 with chronic vestibular neuritis, and 1 with vestibular decompensation. All 8 cases had CCJ misalignments and received Orthospinology chiropractic intervention to improve alignment. Cases 1,2,5,6 and 8 had CRM procedures performed. All cases but 4 and 7 were given personalized vestibular rehabilitation exercises such as VORs. All cases were re-examined at 30 days and found to have subjective and objective improvement with their DHI scores decreasing significantly. Direct statistical analysis of the DHI score changes was used to find the end values by subtracting the post-treatment value from the pre-treatment value and dividing the difference by the pre-treatment value. (TABLE 2)
Since each case received Orthospinology chiropractic intervention, with some also receiving a mix of CRM procedures and vestibular rehabilitation exercises, it is difficult to say how much each intervention individually helped each case. However, cases 4 and 7 only received Orthospinology intervention and their DHI improvement was noteworthy.
An interesting finding published by Rochester found that patients treated with Orthospinology had better neck pain disability outcomes if their initial structural correction was greater than 30%.45 Each case that received an intraprocedural x-ray in our study had objective improvement with their CCJ alignment after the initial Orthospinology intervention as visualized on the x-ray. (TABLE 3) We did not take an intraprocedural x-ray on case 3. Case 7 had an intraprocedural x-ray taken roughly 12 months after the initial Orthospinology intervention so the post findings for this case should be interpreted with caution. Though our study only includes 8 patients, these findings stimulate the question of the CCJ’s alignment with its relation to the symptom of dizziness.
Our final discussion point is cervical dizziness. Cervical dizziness has yet to be an established diagnosis or criteria. Since there were vestibular hypofunction findings and higher-level diagnoses in all 8 of our cases, they would not fit the currently proposed criteria for cervical dizziness.28 Saying this, intervention to their cervical spine still achieved favorable outcomes. This finding leads us to the question of causative versus contributory. It is unlikely that any of these 8 cases’ cervical lesions were the complete cause of their dizziness, which disputes a causative relationship. However, it is relevant and logical to assume that the cervical lesion (CCJ misalignment) observed in each case had some degree of contribution toward their presenting dysfunction and symptoms.
CONCLUSION
A 30-day trial of Orthospinology Upper Cervical chiropractic intervention and a personalized vestibular rehabilitation program was safe and beneficial at reducing self-perceived dizziness handicap in the short term for these 8 cases. This study adds fuel to the cervical dizziness debate, bringing attention to the question of contributory versus causative. Future studies should isolate Orthospinology Upper Cervical chiropractic intervention as the only intervention applied to patients with dizziness to test for higher level efficacy. Future studies comparing CRM procedures to other forms of habituation and canal stimulation for non-BPPV vestibular hypofunction may be beneficial.
ACKNOWLEDGEMENTS
The author would like to thank Dr. Christie Kwon for being the IRB faculty sponsor of this project.