
Introduction
Chiropractic is one of the most used alternative health care systems for a variety of childhood conditions in the United States.1,2 A systematic review from 2019 by Prevost et al described 4 medium/high quality studies of the clinical effectiveness of chiropractic treatment of otitis media. While the children had primarily favorable results and no serious adverse effects, the studies were small and the level of evidence low and was therefore inconclusive.3 Case reports have been published regarding management of otitis media by chiropractors, demonstrating resolution of conductive hearing loss,4,5 but high quality evidence is lacking for conclusive recommendations.3,6,7
Hearing loss may be conductive, sensorineural, or mixed.8,9 Conductive hearing loss can result from a variety of anatomical and physiological interferences, both acquired and congenital, although the major cause in children is otitis media with effusion.8 Studies report a 15% prevalence of hearing loss in school-age children, attributed to approximately 90% conductive etiologies; this approaches 26% in lower-middle income countries.9 Otitis media is a prevalent condition in the pediatric population. By the age of 3, 50-85% of children will have been diagnosed with otitis media with effusion.10 Although patients typically exhibit ear pain and fever, complications such as hearing loss can occur. If left untreated permanent hearing loss may be the result.
Allopathic management ranges from watchful waiting, medication (otitis media), or surgical interventions.9 Complementary/integrative medicine (e.g., echinacea, xylitol, probiotics, homeopathic treatments, chiropractic, etc.) have been used in conjunction with conventional therapy and during watchful waiting periods. Again, supportive evidence is lacking.6,7
Our paper discusses the resolution of hearing loss following chiropractic manual therapy in a pediatric patient, adding to the literature supprting low-risk alternative treatments.
CASE REPORT
The patient was a 4-year-old-male with an unremarkable history, void of symptomatic ear infections or medications. He received routine wellness examinations but no recommended vaccinations. He was born vaginally at home without complications or interventions. He was breastfed until he self-weaned at about 3 years old. He was never given formula and was introduced to solid foods around 6 months of age. His diet involved all the major food groups, including foods containing dairy, gluten, and eggs.
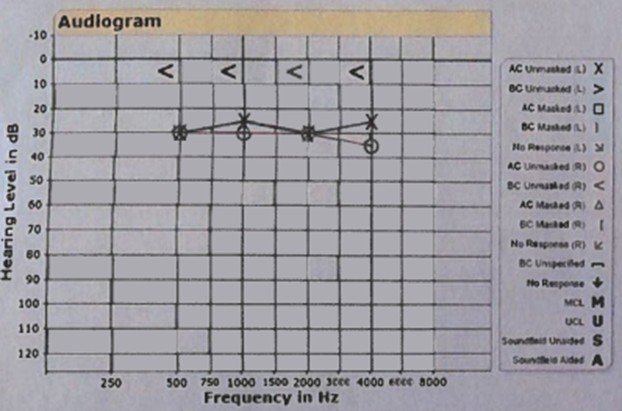
HIs parents became concerned when he was not responding to them when asked to do something or when his name was called. Following this observation, he was taken to his primary care provider for an evaluation. The primary care provider performed an exam on the patient and confirmed the parent’s suspicion of hearing loss and found fluid bilaterally in the ears. The child was referred for an audiogram to determine the extent of the hearing loss. To differentiate between attention/selection/hearing loss, he underwent an audiogram and was diagnosed with 25% conductive hearing loss bilaterally. Hearing loss is diagnosed when the Y-axis levels are above 20 db.11 As shown in the audiogram in Figure 1, all the levels for this patient were above 20 dB for both ears. Mild hearing loss is diagnosed between 20-40 dB and the patient’s numbers fall within this range. An internal ear examination on the same day revealed fluid in both ears. The primary care physician recommended using medication to help with the fluid and the hearing loss. The patient’s guardian declined this treatment at the time to pursue chiropractic care.
.jpeg)
Clinical Findings
An internal examination of the ears revealed non-purulent fluid behind both tympanic membranes. No absolute or relative contraindications to chiropractic treatment were found during physical examination. The patient had hypertonic musculature in the suboccipitals and cervical paraspinals and decreased occipital glide on the right and left lateral bend and right rotation of C1. All other physical, neurologic, and orthopedic exams were negative. The patient was able to perform all tasks (relative to age appropriateness) asked of him without difficulty.
Diagnosis and Management
The patient was diagnosed with cervical subluxation associated with cervicalgia and hypertonicity of the cervical paraspinal musculature. Informed consent included the options to pursue other approaches, including watchful waiting (as otitis media with effusion has been shown to spontaneously resolve)9 or the medical intervention that was previously offered to them. The parents chose chiropractic treatment for 1 month to gauge improvement with their son’s hearing loss, and would pursue further medical intervention if no changewe initially set a treatment plan of 3 chiropractic visits a week for 2 weeks. After 2 weeks of care, fluid was still noted in both ears and no improvement in symptomatology was noted so the decision was made to extend the care plan to 3 weeks.
Therapeutic Intervention
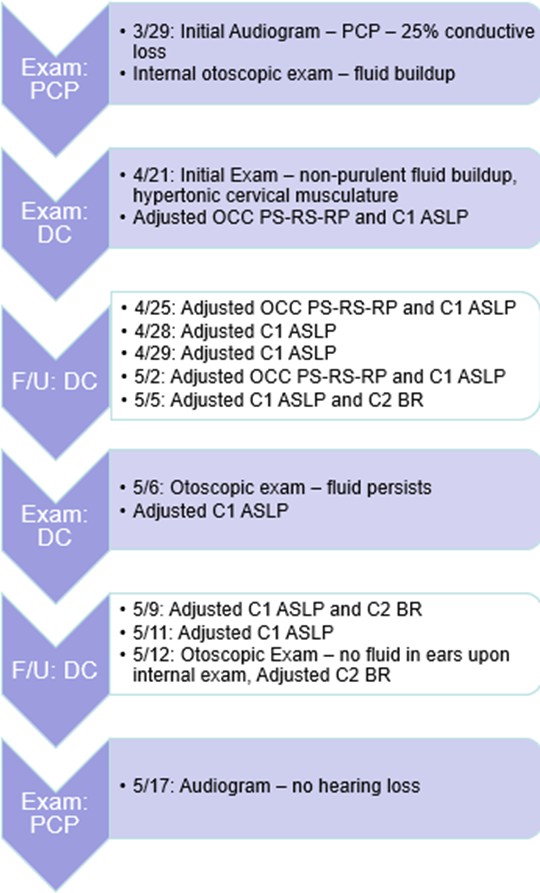
Given the patient’s age and size, the Activator instrument was used to deliver specific low force adjustments to the upper cervical spine. In total 10 adjustments were performed in 3 weeks. Figure 2 details the frequency of adjustments and the specific segments that were adjusted at each visit.

Follow-Up
The patient had a follow-up visit with his primary care physician after the 3 weeks of treatment and the physician noted that no fluid was present in the ears. The patient was sent for another audiogram at a separate location. Figure 3 shows frequencies detected below the 20 dB level. The parents were encouraged to continue chiropractic care as prevention. The patient’s guardians chose to continue chiropractic care on a PRN basis.

Discussion
Hearing loss in children can manifest from a variety of origins, including wax or foreign objects in the ear, syndromes, and pathologies, and most commonly otitis media.10 Otitis media with hearing loss, particularly chronic otitis media with effusion, can have a detrimental impact on a patient’s quality of life, especially when affecting young children. Early diagnosis and management are essential in preventing long-term complications associated with hearing loss.8 An internal ear examination and an audiogram to confirm hearing loss are needed for definitive diagnosis.9 Our patient was in the mild hearing loss range for both ears when the initial audiogram was performed. The second audiogram indicated improvement. Medication and surgical procedures are often recommended as treatment for hearing loss due to otitis media.10 With the rise of antibiotic resistant bacteria, interest in alternative treatment options should be considered.12 A possible mechanism of improvement is relaxation of noted muscle spasm in the cervical region following chiropractic manipulation. The muscle spasms may have been mechanically disporting the eustachian tube, lymphatic drainage, and/or disrupting nerves or blood vessels to the inner ear causing improper drainage.
Strengths of this case study include the availability of objective hearing loss testing, the timing of the resolution, and patient/parent satisfaction. Limitations of this study must acknowledge that conductive hearing loss may resolve with natural progression,13 although there was a lack of improvement prior to the onset of chiropractic treatment.
Conclusion
This case report detailed chiropractic spinal manipulations with a pediatric patient suffering from conductive hearing loss possibly due to otitis media with effusion. The outcome of this case was full resolution of hearing loss in 3 weeks of care with 10 chiropractic adjustments. Patients (or patients’ guardians) and providers may consider chiropractic manual therapy for hearing loss caused by otitis media in the pediatric population as a conservative non-invasive treatment.. Further study is warranted to assess the mechanism and efficacy of chiropractic manual therapy for this condition.