


INTRODUCTION
Subluxation remains an enigma in spite of being an emblematic idea within conventional chiropractic. The purpose of this paper is to report and then explain my finding that there is little if any quantitative evidence of what subluxation could be as a clinical entity. I have previously noted that chiropractors seem to fall along a spectrum of accepting subluxation for what they understand it to be, between a majority conventional position in terms of the founding principles and a very small minority position who reject the idea as dogma.1
I do not consider this to be a problem, rather an opportunity to propose a change of inquiry to one of qualitative narration of clinical evidence to better understand subluxation as a perspectival, narrated phenomenon. As such, I will propose that the idea of small spinal dysfunctions in the spine holding an association with health and wellbeing can be adequately shown to be real on the basis of being a perspective-dependent knowledge claim. From this position will come my reconciliation of the clinical acceptance of subluxation by chiropractors and the absence of physical evidence for its existence. It may be trite but it must be said that there is also no evidence that disproves the existence of subluxation.
I shall present this paper in 4 parts:
-
Part One: The report of my systematic review, for which I will keep the ‘methods’ straightforward as such reviews are no longer considered novel in chiropractic and are accepted as a standard practice of inquiry;
-
Part Two: Identification of the resultant conundrum with my proposition of a reason for it. I deliberately use ‘conundrum’ in the sense of the matter having conjectural nature. I show it to be an intricate and difficult (Merriam-Webster), or complex, problem;
-
Part Three: My explanation of the conundrum in terms of a complex problem for the purpose of allowing resolution of its intricacies and difficulties through the application of philosophical principles; and
-
Part Four: The application of the philosophical proposition of Perspectival Truth that should dissolve the troubles of the minority who see subluxation as dogma, by providing the context of subluxation as a perspective-dependent knowledge claim within the framework of chiropractic being a complex problem.
I will commence by identifying the simple problem that led to me conducting the systematic review.
Identifying the Problem
There is a gap in the quantitative knowledge of subluxation. I make this claim on the basis that all contemporary argument in favour of excising subluxation from the profession is based on viewpoints and not scientifically acquired knowledge. The most vocal groups led by Leboeuf-Yde and by Kawchuk, and including Innes, Young, Hartvigsen, and Côté resort to denigration by language, as an example by writing ‘the “traditional” group that subscribes to concepts such as “subluxation” and the spine as the center of good health’ from which they extrapolate the proposition that this ‘is becoming increasingly obvious and problematic.’2
At no stage has any argument against subluxation been advanced with an acceptable basis of scientific observation and evidence. For all intents and purposes the argument against subluxation is opinion, as are the arguments for it. In the absence of evidence these arguments can only be conjectural, hence the intent of this systematic review was to identify evidence of subluxation as reported in the indexed literature. Instead I found none.
PART ONE: SYSTEMATIC REVIEW
I report this systematic review in brief. My method was compliant with the principles of the Cochrane Handbook (Ver 5.1) for Systematic Reviews of Interventions3 and met the Core Standards.4 The purpose was to retrieve and assess the current state of quantitative evidence about subluxation with an expectation to find an association of causation between subluxation and health status. My target population was humans and my strategy was informed by my knowledge of the primary chiropractic literature.
The strongest evidence was set to be findings regarding the null hypothesis subluxation is not associated with health status in humans. It was reasonable to frame this hypothesis given the strategies of Owens et al of 19995 and more recently of Harrison and Oakley6 who advanced 6 subluxation types. The idea being to produce ‘specific quantifiable and testable hypotheses … that can be used to verify or falsify the theories’ [of subluxation].5
In Table 1 I show the 6 subluxation types of Harrison and Oakley6 against the 8 propositions of Owens at al.5 It is obvious the idea of subluxation has been translated into types by believed mechanisms but this does not confer any reality on what is typed and mechanised.7 Also, in 1977 Hildebrandt published ‘radiographic classifications of subluxation’8 which served a purpose at the time to comply with reimbursement requirements; it is a list of descriptions of what was then considered to be radiographic representations of spinal subluxation which are not directly relevant to this report. And in spite of a textbook by Leach9 now in its 4th edition, there seem to be no reports advancing a theory of subluxation let alone evidence for any theory, or aspects of a theory, being tested. It is reasonable to expect at least 1 or 2 or these proposed theories to have been explored; after all, the mechanics of subluxation are eloquently reported by the Harrisons10,11 and it can be said that there is a body of cogent literature that describes the mechanisms of manual correction of subluxation.12,13
In Table 1 the types of subluxation given by Harrison and Oakley, and Owens et al, are mapped against the ‘idea’ they represent. This table seems to cover distinctions and relationships between mechanical and neurological factors thought associated with subluxation in the profession’s historical literature including movement change, muscle change, connective tissue change, and neural change.14 The factor I can’t yet identify as being addressed is vascular change15 which has potential to be a cause and/or an effect beyond its overt presence as oedema, in the supposition that there is indeed any vascular change that is associated with any ‘subluxation’.
Methods
This systematic review was undertaken in the last quarter of 2018 and the primary results represent the literature at the end of that year. On the basis that this initial search did not return any research-based papers the string was modified and run again at the time of writing this paper, October 2020.
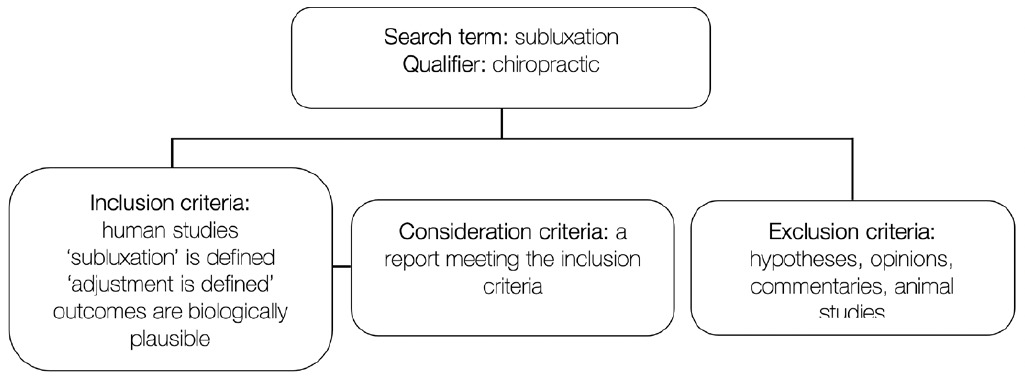
My schemata is given as Figure 1.
My data sources were the primary chiropractic literature as indexed in MEDLINE accessed using PubMed,® and the Index to Chiropractic Literature (ICL), accessed directly.
I categorized my returns by ‘class of subject’ (human accepted, animal rejected) and was to then rank them by evidential strength as a systematic review or meta-analysis, an RCT, literature review, cohort study, case control, case series, case report, opinion, or historical review. The PRISMA Guidelines16,17 were held to be relevant.
My challenge was to determine a consistent understanding of what clinical entity constituted ‘subluxation’. The characteristics I applied are given as Table 2.
Process
The following search string limited returns to the discipline of chiropractic with options for the name of the clinical entity in addition to subluxation: “chiropractic”[MeSH Terms] AND (subluxation[ti] OR (“joint dislocations”[MeSH Terms] OR (“joint”[All Fields] AND “dislocations”[All Fields]) OR “joint dislocations”[All Fields] OR “subluxation”[All Fields]))
The primary data base was Medline in which the complete search string was entered as given above. The secondary data base was ICL where I additionally applied a modified strategy better suited to its advanced screen using the terms ‘subluxation,’ ‘hypothesis,’ ‘results.’ I did not use CINAHL due to it not being Open Access and therefore limiting those able to access its holdings. All readers have open access to MEDLINE through PubMed,® and to ICL directly.
Results
Applying the search-string within ICL on Tuesday 11 December 2018 returned 335 articles. The string was again run in October 2020 and filtered by ‘NOT case report’ returning 65. Limiting the date range to ‘(2010) TO (2020)’ and modifying the string to ‘(chiropractic) AND (subluxation) AND (human research) NOT (case report) NOT (commentary)’ returned 11 papers. Six of these were historical explorations by Senzon which are not relevant to my intent. Including ‘NOT (history)’ returned just 2 papers, each reporting an organization’s research agenda, also of no relevance.
A further look within ICL with the modified string ‘((chiropractic) AND (subluxation)) AND (human)’ returned 173 articles, including dross by Ernst and Homola. I determined that this filter was unhelpful.
Applying the base search-string within MEDLINE on Tuesday 11 December 2018 returned 101 papers. A repeat search using the same string on 17 September 2019 returned an additional 5 papers which did not change my results. Data harvesting returned a further 95 papers of variable strength and relevance from low to none.
About 105 found papers were accepted as directly relevant and the harvested papers were dismissed. An important finding is that the found papers included case reports notably by Alcantara18–21 who writes in a structured manner inclusive of the information that allows interpretation and application by others, the measure of replicable clinical reports.
The remaining non-case report papers were classified as surveys, literature reviews, commentaries, letters, and other. There were ‘guidelines assessments’22,23 which are not primary reports. One cohort study investigated ‘spinal manipulation’ for a ‘manipulable lesion’,24 whatever that may be, and a prize winning cohort study25 of crepitation associated with generic spinal manipulation failed to describe the target of the manipulation. Whilst these may be of use within the field of manual medicine they did not address the manual correction of subluxed vertebrae which characterizes conventional chiropractic.
No reports of primary inquiry identifying quantitative attributes of subluxation in humans were found. There are many case reports reporting subluxation identification and correction in humans.
Comment on systematic review
The results from this review do not show support for subluxation being an entity with quantifiable dimensions. This takes nothing away from the work of Harrison and Oakley in particular, nor from the tenets of other well-documented techniques like Gonstead Methods26 and Activator Methods.27 Rather, it provides a stronger reason for seeking evidence about the ‘thing’ they address in a thoughtful, reasoned, evidence-based manner. As with Massimi and her example of quarks,28 to which I shall return, we have a phenomenon that we can’t observe but for which there are several clinical approaches to identify, codify and correct.
PART TWO: THE CONUNDRUM
We know that agreement is found among most (70-90%) practitioners29 that subluxation is important in conventional chiropractic.30 The term sits within the published curriculum of all but 2 US course catalogues.31 Elsewhere32 I have reported that a regulatory body, the General Chiropractic Council (GCC) of the UK issued an evidence-free edict that there was no evidence for subluxation and their opinion-based corollary that it only held interest as an historical concept. Without any critical thought, about a dozen chiropractic colleges33 echoed that uninformed opinion and presumably no longer teach subluxation as a clinical concept.
Keating critically examined a ‘subluxation hypothesis’34 which drew comment.35–37 He also provided a commentary on the scientific basis for the chiropractic subluxation.38 Others have questioned whether the subluxation is real7 which also drew critical comment.39 None of these works venture beyond opinion and in the absence of supportive evidence are based in fantasy. They cannot be accepted as perspectival truths which must have a relationship to an experienced reality.
Evidence-based Ideas
Haavik and her team publish evidence-based ideas of the neurological outcomes of spinal manipulation in the absence of a known subluxation, which I interpret as reporting the effects of a physical action (manipulation) about the spine.40–42 The work of Hotta and Watanabe43–45 similarly elucidates mechanisms at the leading edge of neuroscience that strengthen arguments of biological plausibility but are not evidence of subluxation per se.
It remains open as to whether the effects reported from the labs of teams Haavik and Hotta are generic or specific to the correction of subluxed vertebrae. I am yet to see evidence of what it is they address in a clinical sense, but accept their collective belief that the target, should it exist, could be called a subluxation. But how do we know that any such target could also not be called a subluxation?
Holt, a member of Haavik’s research group, found46 ‘definite agreement on the motion segment that had the most subluxation findings’ yet his report fails to be convincing that the ‘thing’ on which agreement was reached by experienced chiropractors was anything more than something about which the clinicians agreed whether or not they called it subluxation. In other words there is evidence of what it was that generated agreed clinical findings and we can only presume it is appropriate to name it ‘subluxation.’
This subtle understanding shows Holt’s quantitative report is his opinion from his perspective and hence a Perspectival Truth, and is not to be taken as quantitative evidence of subluxation, nor as opinion. It actually demonstrates the difference between a perspectival truth and an opinion, the former is informed by observed evidence.
Statement of Conundrum
In the absence of quantitative evidence for subluxation, how do chiropractors practice? On the assumption that a therapeutic intervention must have a target and a purpose, what is the target and what is the purpose? Is this a simple problem that is easy to resolve, or is it a complex problem that commands our attention?
PART THREE: SUBLUXATION WITHIN A COMPLEX PROBLEM
My consideration of the conundrum in terms of a complex problem is for the purpose of allowing a resolution of it through the application of philosophical principles; chief among these being Perspectival Truth, a way for a person to observe something and believe it is real, as demonstrated by Holt with what he documented as evidence, but not by Leboeuf-Yde et al who offer no evidence only opinion at times wrapped in parable (Unhappy Families).2
The inference of accepting subluxation as a perspectival truth flows from the idea that the world’s 105,000 chiropractors may well exhibit 105,000 perspective-dependent knowledge claims which in turn would represent chaos. That argument proposes there should be a definition of subluxation. The weakness in this argument is the demonstrated lack of uniformity among the definitions which do exist in the profession. For the sake of my counter-argument I will propose there are 105,000, give or take, definitions of subluxation and in making this claim also note this has neither retarded the growth of the profession nor the satisfaction gained by patients.
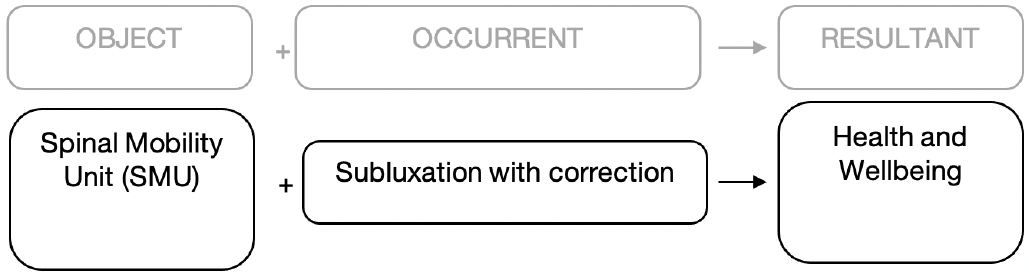
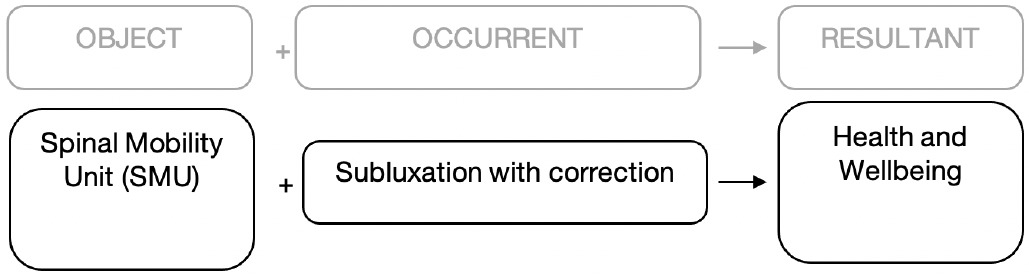
However my analysis of chiropractic as a complex problem will allow an operational definition of subluxation to emerge that endows my reasoning with historical integrity.47 To begin my analysis I will construct a framework to allow observation, description, and meaning. To create that framework I propose ‘chiropractic’, in the sense of a clinical discipline, represents a complex problem that may be represented as shown in Figure 2.

The shape of my complex system given as Figure 2 follows Snowden and Boone’s48 ‘Leader’s Framework for decision Making’ to operationalize the problem at levels appropriate to the characteristics of a clinical discipline. I give these characteristics as:
-
Large elements, being both overt (object as in the site of the lesion; occurrent as in the therapeutic act to address the lesion; resultant as in the clinical outcome) overlaid by multiple covert potentials expressed as patient individuality;
-
Nonlinear clinical interactions where minor changes can produce disproportionately major consequences. For an example, an unskilled occurrent may harm or cause death, a major consequence;
-
A dynamic system in which the whole is greater than the sum of its parts where solutions can’t be imposed; rather they must arise from the circumstances. This is typical of systems within living entities;
-
The history of the system where the past is integrated with the present, the elements evolve with one another and with the environment; and evolution is irreversible. These are characteristics of clinical presentations;
-
Contradiction where even though a complex system may, in retrospect, appear to be ordered and predictable, hindsight does not lead to foresight because the external conditions and systems constantly change. My interpretation of this is that while a consilience drawn from similar case reports may suggest a certain intervention, it offers no assurance that any specific intervention is the best in any specific clinical presentation of a case about the same as that from which consilience is drawn. This principle also applies to the supposed evidence of RCTs where a specific act needs to be drawn from a group response with no assurance of replication, which shatters the notion of ‘evidence-based’ chiropractic; and
-
Constraint in which the agents and the system constrain one another, especially over time. This means that we cannot forecast or predict what will happen. This is typical of clinical uncertainty.
By applying these characteristics to chiropractic we can represent chiropractic as a complex problem (Figure Three).
Resolution of the Complex Problem
I propose that this complex problem suits the application of Boolean Classes to test my observation that 105,000 chiropractors each do something to their patients in such a manner that most patients pay from their own pocket and return for continuing care. I will state the classic Null Hypothesis thus:
H0: There is no association among small spinal dysfunctions called subluxations by chiropractors with management by chiropractic methods and changes in health status.
In Boolean terms referencing the complex problem, I express it as:
IF [Location S] AND ([Idea A)] AND [Idea B] AND [Idea C] THEN H1
Where
‘S’ is a location within the spine described as the articulation complex between two contiguous vertebrae or analogous structures (object, spinal mobility unit);
‘A’ is the idea that small biomechanical dysfunctions may occur within the articulations of the spine when vertebrae sublux, creating a subluxation. ‘A’ has an historical lineage dating from 1600 BC;
‘B’ is the idea that ‘A’ may be identified and corrected, commonly by what is called the chiropractic adjustment. ‘B’ emerged in medicine in the early part of the 19th Century and in the latter part was finessed to a health discipline by DD Palmer where the dysfunction came to be termed subluxation and its management was correction of those subluxed vertebrae by manual methods, called an adjustment; and
‘C’ is the idea that when ‘A’ and ‘B’ happen at or in ‘S’ then a quantifiable change in health is associated (Wellbeing). ‘C’, as an outcome in the form of a change in health, emerged in early medical thought as a means to measure the effectiveness of intervention and became strongly associated with the correction of subluxation when chiropractic emerged in 1895. From about 1920 the outcome of mental health became included in chiropractic, and from Engel’s arguments in 1977, medicine in general49,50 shifted from a biomedical perspective of disease to a biopsychosocial perspective on health, as has chiropractic.
Hypothesis testing is not common in qualitative methods51 but can occur.52,53 In quantitative methods the hypothesis examines large data, the general, to make claims for the specific. In qualitative methods this is reversed, where the hypothesis makes a claim from the specific. The claim in my case would be about reported association.
Summation of the Complex Problem
I summarise chiropractic in Figure Four:

My argument is that the Object is quite well known, in other words it is fully evidence-based. It is the anatomical site in the spine where small dysfunctions are known to occur. No rational person could lay claim that such small dysfunctions do not occur, they are documented from the earliest medical writings and need little in the way of information to show they exist which we would believe to be evidence. Chiropractors typically use palpation of these to identify subtle changes in intersegmental movement and then associate these findings with other signs and symptoms.
Similarly the Resultant of Health and Wellbeing is well established in the literature and there are multiple tools of measurement and contexts within which the measured outcomes may be placed, for example within Waddell’s Biopsychosocial model.54 It is reasonable to state that Health and Wellbeing are states of existence that can be measured and are thus evidence-based.
The matter of Quality of Life was known to Palmer. Senzon observes ‘In his 1889 anti-vaccination tract republished in 1894 … He ended the article with a few common sense approaches to “natural health producing and disease repelling agents.” This is a rudimentary description of the body’s own innate healing mechanisms. D.D. also named some of the things people can do such as cleanliness, pure air and water, plain wholesome food, abstinence from intoxicants, outdoor “open air” exercise, and city-wide hygiene’.55
This brings us to the Occurrent which I give as a subluxation with its correction, as the essential part of the Explanandum to justify the Explanans. The purpose of this paper is to show that the use of the philosophical tool of Perspectival Truth fully satisfies the need for a sense of order in the knowledge claims of chiropractors in that they are accepted as perspective-dependent.
PART FOUR: ACCEPTING PERSPECTIVAL TRUTH
I propose a shift from viewing subluxation as a ‘thing’ that can not be quantified, to a phenomenon understood by informed clinical narration and observable clinical evidence. The philosophical principle for this approach is given by Massimi28 in her discussions on observing unobservable phenomena; specifically in her argument ‘quarks’ and for us in ours, ‘subluxation’.
In other words, I will show that we can come to know subluxation from the clinical stories we create about the clinical phenomena we observe, particularly the cascade of outcomes from perceived correction. I propose that an effective way to show this is by narration from clinicians and perspectival truths from clinicians and patients, a proposition which if valid will place case reports as the highest level of evidence for chiropractors. My bias must be declared and it is my position as a scientist and writer to accept the primacy of case reports in forming the evidence base of chiropractic as a clinical discipline.
Perspectival Truth
I hold the view that there is a perspectival truth56 in the idea of subluxation as it is relevant to chiropractors. The phrase ‘perspectival truth’ means the observer brings their own perspective to the observed. This is the nature of patient-centered clinical practice in general and of chiropractic in particular. The perspectival truth will differ among observers; however, as Holt et al demonstrated46 there is good clinical agreement among clinicians with identifying the phenomena thought to indicate spinal subluxation.
My perspectival truth about subluxation is that its identification, correction, and the clinician’s intent all change according to the clinician’s perspective at the point in time of a doctor-patient interaction. In this respect the conditions of a Complex Problem are met, specifically that the Occurrent is dynamic. I reject the idea that subluxation must be an unchanging thing represented by disembodied data.
I hold that the idea of subluxation is universal, is time-honored, and has substantive cross-cultural representation. The idea has been held in Egyptian medical writings from at least 1,600BC.57 Bovine58 has shown how the meaning of that idea came to take the semantic form of ‘pararthrema’ in Greek and of ‘subluxatio’ in Latin. We know the meaning of the word ‘subluxation’ in medicine of the early 19th Century59,60 and we know Palmer was not obsessed with that word, in fact he first termed the lesions he addressed as ‘luxations’61 with an emphasis on chiropractic being ‘… the science of … how to adjust displaced vertebrae …’.62
Today the idea is truly global given that the WFC documents chiropractic practice in over 93 countries.63 Only the naive would dare suggest that English is the global language of chiropractic; we know it is taught in Japanese,64 Spanish,65 and French,66,67 among others.
The Chinese Perspective
In contrast to the McGregor-Puhl argument68 that subluxation is representative of unorthodox chiropractic practice, the idea of subluxation and its association with wellbeing as being iconic of chiropractic has strong meaning in Traditional Chinese Medicine (TCM). The idea is expressed in the clinical approaches of both Traditional Chinese Spinal Manipulative Therapy (TCSMT)69 and Traditional Chinese Orthopedic Medicine (TCOM).70
Lamenting that the clinical art of TCSMT is not as widely recognised as that of chiropractic, Wang69 observed ‘Although chiropractic’s “subluxation” and TCSMT’s “Jin Chu Cao and Gu Cuo Feng” theory have not been widely recognized, comparatively TCSMT has a mature theoretical system and satisfactory clinical effectiveness’. They suggest that meaning is found in ‘TCSMT’s basic … clinical application,’ a proposition I agree is applicable to chiropractic.
Yuan et al70 are aligned, stating ‘“Gu Cuo Feng and Jin Chu Cao” is the key pathogenesis for spinal degenerative disease, such as cervical spondylosis, but there is also … controversy for the concept of “Go Cuo Feng and Jin Chu Cao”.’ He shows how the concept of ‘Cu Cuo Feng and Jin Chu Cao’ starts with structural abnormality and dysfunction and builds with clinical symptoms, conventional physical signs … special physical signs (mainly by palpation) and imaging measurement to indicate systemic disorders.
As with Haavik, Yuan is reporting associations between spinal manipulation and ‘brain functional activity’71 and between spinal lesions and vertigo,72 as examples. Overall, I hold similar views that chiropractic has a ‘mature theoretical system’ and that its ‘clinical effectiveness’ has much greater strength than ‘satisfactory’.73–75
Animal Models
There are dated reports of bench science with animals such as ‘Cleveland’s Rabbits’ (early 1950’s)76; however, I consider these not to have relevance as they created a mechanical lesion thought to be representative of subluxation. My intent is to seek evidence of subluxation in humans in the clinical context; I am not interested in mechanically-induced lesions in animals or humans.
However these studies contribute to proof-of-concept where the concept is that light pressures on a nerve fiber affect neural transmission. I consider this concept to be established, primarily through the works of Suh77,78 and Sato.79 The significance of Suh’s findings were noted in 1979 by the New Zealand Royal Commission.80
The fact that the matter of subluxation in animals remains current81 and that case reports show animals responding to chiropractic care82 eliminates any argument that the outcomes of chiropractic care are in any way reports of placebo effects.
Finding the Narrative
The evidence supports the idea of subluxation within chiropractic and it may be that its meaning could be derived from case reports using narrative methods.29 Case reports describe ‘real world problems’83 in chiropractic as well as other disciplines. There is ample evidence to review; on 12 April 2021 the search string ‘(subluxation) AND (case report) OR (study) or (series) AND (YEAR)’ returned from ICL 235 articles published in the year 2019 and 226 published in 2020. These are appropriate numbers for qualitative thematic analysis.
THE WEAKNESS OF THIS PAPER
My internal weakness lies in the proposition that 105,000 perspectival truths of chiropractic as 105,000 definitions or understandings, with each being variable depending on the patient, would represent a state of chaos.
My counterargument is 2-fold:
-
That chaos already exists as a survey of definitions held by associations will attest. This is sufficiently self-evident as to not require more detailed analysis but 2 examples will make the point;
1.1 The definition held by the WFC states chiropractic is ‘A health profession concerned with the diagnosis, treatment and prevention of mechanical disorders of the musculoskeletal system, and the effects of these disorders on the function of the nervous system and general health. There is an emphasis on manual treatments including spinal adjustment and other joint and soft-tissue manipulation’84 with no mention of subluxation; and
1.2 The definition of the International Chiropractors Association holds the position that ‘The science of chiropractic deals with the relationship between the articulations of the skeleton and the nervous system and the role of this relationship in the restoration and maintenance of health and concluded with the concept of subluxation is essential to chiropractic, just like oral health is essential to dentistry.’85
The result is the presence of many groups, spread globally, where those groups each gather around one particular interpretation of a definition. This seems to not affect public acceptance nor legal status; and
-
That an operational definition for chiropractic educators can be drawn from the basic ‘5 elements’ model which seems to largely be the case at the moment with the exception of a very few colleges that reject the model.33
My Position
It seems reasonable to propose that a Perspectival Truth about subluxation can be considered as being that meaning which a trained chiropractor gives to a standardized set of clinical findings. In many respects this would seem true to the intent of evidence-based medicine when clinical findings are interpreted in light of the doctor’s experience, the patient’s preferences, and best available evidence.
CONCLUSION
I find little evidence that subluxation is a quantifiable entity and rather, that it exists as an idea that small dysfunctions in the spine relating to health and well-being are identifiable and correctable.
Notwithstanding the reported vagueness1,86 about subluxation, it is ‘an important practice consideration for about 70% of chiropractors’ allowing ‘patient care with a musculoskeletal spine focus’ to be ‘dominant in clinical practice.’12,87
It seems easy to appreciate that there are many interpretations, even misunderstandings as to what the term means yet harder to understand why the word is seen by some as divisive2 let alone indiscriminately excluded from the learning experience of some the profession’s next generation.33
I find that the position of an elite minority88–91 traducing the profession by assigning the derogatory term ‘dogma’ to the idea of subluxation is no longer credible and I invite argument to the contrary.