
Introduction
An important differentiation between scoliosis and pseudo-scoliosis was made in a 2006 publication by Harrison et al.1 It was previously determined that a lateral translated thoracic posture displayed a vertebral coupling pattern of a lower lumbar lateral flexion towards the thoracic shift and an upper lumbar/lower thoracic spine lateral flexion away from the shift back towards the vertical, essentially creating an S-shape.2 In the 2005 study,1 purposeful thoracic lateral translation movements were made by 15 volunteers and showed that with >50mm of translation, a 14-19° lumbar (L1-L5) or thoraco-lumbar (T12-L5) Cobb angle was created.
The key characteristic that differentiates true scoliosis and pseudo-scoliosis is that in lateral translation of the thorax over the pelvis (which creates the characteristic S-shaped spinal coupling pattern) involves no rotation of the involved vertebrae; therefore, the spinous processes remain centered.1 Alternatively, true scoliosis has definitive vertebral body rotation as seen with the spinous processes off center. This is a critically important differentiation clinically, as scoliosis is difficult to treat (reduce) while lateral thoracic translation postures are relatively straightforward to treat.3
The first reporting of the clinical treatment on reducing a lateral thoracic translation posture was the non-randomized controlled trial in 2005.3 Sixty-three chronic low back patients experienced an average 8mm reduction in lateral thoracic translation after 36 treatments over 11.5 weeks. There was also a 2.2-point reduction in pain rating. A comparison group of 23 volunteers not receiving treatment had no radiographic changes in posture and no change in pain rating after 37 weeks.3
Since the publication of this first trial,3 there have been case studies documenting the reduction of this posture (e.g. Henshaw et al.4). The approach that CBP technique applies to reduce lateral translation postures is 1-sided or ‘mirror image’ thoracic exercises, mirror image spinal adjusting, and mirror image traction,3,5–7 directed toward restoring verticality to the spine and posture.
This review characterizes the evidence of Chiropractic BioPhysics® (CBP®) technique methods5–7 in the reduction of lateral thoracic (pseudo-scoliosis) translation postures and its effect on pain, disability and quality of life.
Methods
A review of the CBP NonProfit citation listings8 was performed for clinical papers reporting on the reduction of lateral thoracic translation postures via CBP technique methods.5–7 Any clinical study type was included (trial, case report/series). A search on both Pubmed and the Index to Chiropractic Literature (ICL) was also performed using the keywords lateral thoracic/thorax translation or pseudo-scoliosis, and this was done to verify if any papers were missing from the CBP NonProfit website listing and/or if any papers were published since its last update (every fall). References were screened from any located articles. Searches were performed in dedicated chiropractic journals and conference proceedings. Experts were also contacted to further locate studies (i.e. authors of located cases).
CBP case reports were searched for this postural distortion and its correction even if not explicitly mentioned in the title of the manuscript. Cases were excluded if the treatment involved patients with scoliosis or if the treatment for the reduction of a lateral thoracic posture was treated exclusively by the prescription of a heel lift (i.e. Fortner et al.9).
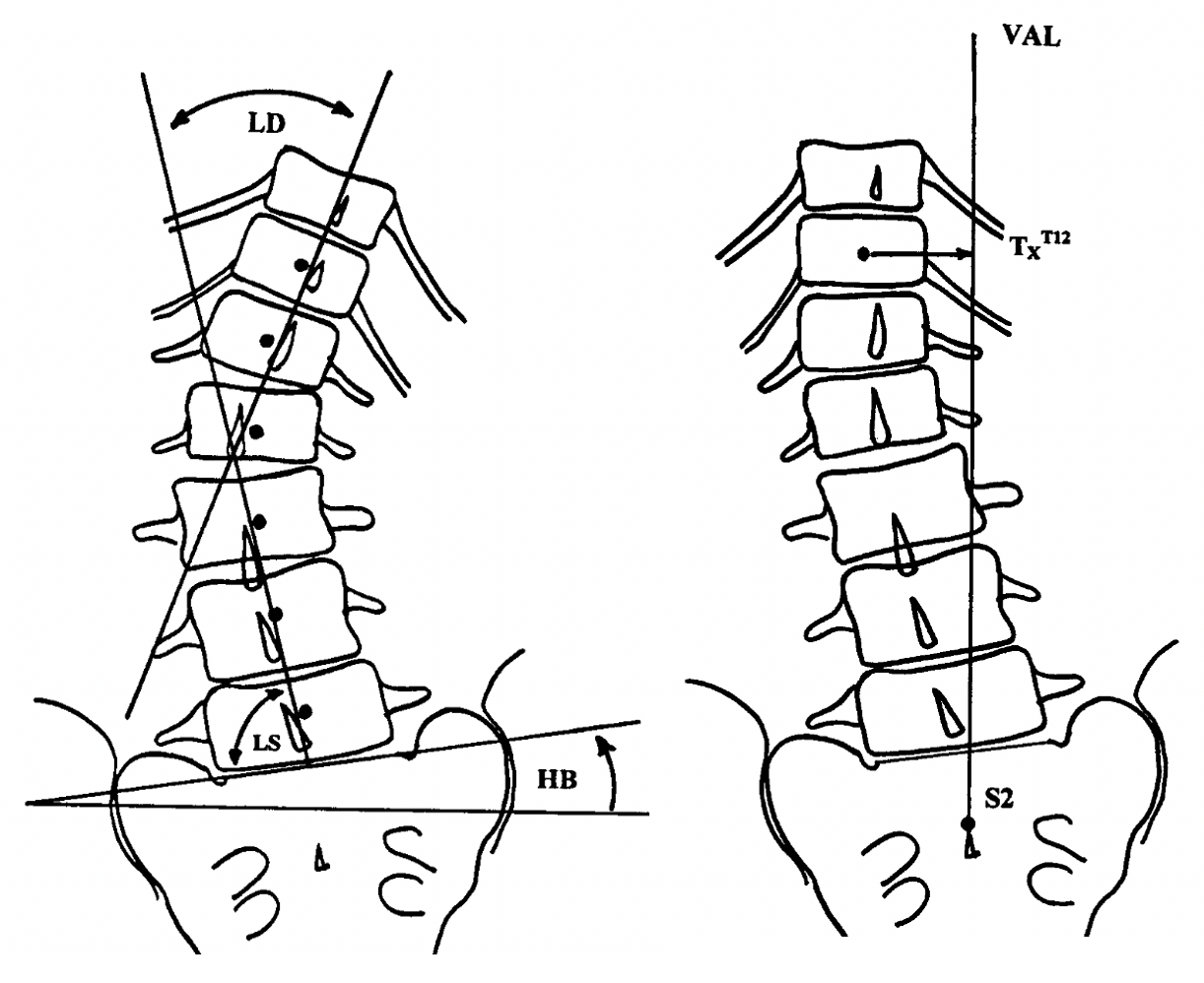
Information extracted from any located studies included the age and sex of patient, chief complaint, number of treatments, time duration of treatment, treatment specifics including traction set-up, traction duration, exercise protocol, adjusting protocol, as well as pre- and post-treatment magnitude of coronal offset (TxT) and corresponding lumbodorsal (LD) and lumbosacral (LS) angles (Figure 1).

Results
Our search of the CBP NonProfit site located one non-randomized controlled trial3 and 6 case reports described in 5 manuscripts4,10–13 (Table 1). Searches in Pubmed revealed 4 hits and ICL 16 hits that either did not meet the inclusion criteria or were already located from the CBP NonProfit website. No other cases were located by searching journals, references or contacting case report authors.

As mentioned, the clinical trial reported an 8mm reduction in lateral thoracic translation posture after an average of 36 treatments over 11.5 weeks in 63 chronic low back pain patients.3 There was a 2.2-point drop in pain rating (3/10 to 0.8/10) during the treatment while there was no change in spinal position or pain rating reported in 23 untreated control group volunteers with chronic low back pain.3
The 6 located cases (Table 1) showed an average lateral thoracic translation reduction of 23mm after 33 treatments over 3.7 months.4,10–13 The corresponding reduction in LD and LS angles were 4.8° and 10.4°, respectively. The average age was 52 and the average reduction of pain was 3.8 points on a 10-point rating scale (5.4/10 to 1.6/10).
The reduction of lateral thoracic postures successfully relieved symptoms in patients with degenerative disc disease,10 Parkinson’s,11 low back pain,4 urinary incontinence,12 and pain associated with post-surgical laminectomy.13 Several cases also reported on improvements beyond pain relief including functional measures (e.g. range of motion), disability (e.g. Oswestry disability index), and quality of life (e.g. SF-36). There were no adverse events reported in any of the located studies.
Discussion
This review has summarized the details from one non-randomized controlled trial and 6 case reports documenting the reduction of lateral thoracic translation postures in the treatment of low back spinal disorders.
The single located clinical trial showed an average reduction of 8mm over 36 treatments3 while the case reports demonstrated an average 23mm reduction after 33 treatments.4,10–13 It is not surprising that the amount of correction shown in the individual cases averaged more than the trial as it is likely that a greater reduction in spine deformity would motivate a clinician to publish a positive clinical outcome (i.e. selection bias). However, since there is limited evidence in the manual therapies,14 lower forms of evidence are acceptable toward informing clinical practice.15,16
Although there was a limited number of total case reports and only 1 trial, the data clearly shows that CBP methods can be used to reduce lateral translations of the thoracic cage. Also, from the data one can estimate a 0.22mm-0.7mm reduction per treatment. Therefore, a patient with a 10mm, 20mm or 30mm lateral thoracic translation posture would require 14-45, 29-91 or 43-136 treatments, respectively. Although there are wide ranges in treatment estimates, these represent the evidence-based practice estimates that currently exists. Further research into the CBP treatment of this postural subluxation will help refine treatment extrapolations.
As mentioned, we did not include any reports on reducing lateral thoracic translation postures by use of a heel lift exclusively or with the treatment of patients having scoliosis. Indeed, there are other causes for the torso to be offset from the midline and these can only be comprehensively assessed by radiography.17 For this reason, we recommend the routine radiographic screening for those presenting with low back complaints as the diagnosis of a lateral translation posture, as differentiated from a true scoliosis or leg length inequality, is clinically important as it dictates a unique potential corrective treatment approach; that is, CBP methods.
Since the treatment approaches to low back disorders have questionable efficacy,18 CBP methods offer a unique and spine-specific, radiographically-guided regimen that has an evolving evidence base, including for the treatment of lumbar and thoracolumbar pseudo-scoliosis. This review adds to other recent reviews characterizing the scientific evidence in the clinical application of CBP methods to increase cervical lordosis, increase lumbar lordosis, reduce thoracic hyperkyphosis, and reduce lateral head translation postures.19–22
Since there is a lack of scientific evidence in chiropractic for many commonly practiced procedures, case reports become an important source for guiding information on clinical practice.15,16 Further, as discussed by the late David Russell, there is also a lack of clinical reports that document direct indicators of pre- and post-vertebral subluxation outcomes23; however, CBP methods including those procedures used to reduce lateral thoracic translation postures help satisfy this clinical evidence gap.
It is also important to mention that although there are contrasting views within the chiropractic profession regarding X-ray use,24–33 this review adds to the accumulating evidence that CBP structural rehabilitation methods leads to reduced spinal misalignment, a type of subluxation.34 In fact, small groups of individuals do argue that there is no support for routine X-rays in diagnosing or aiding treatment choice24,26,28,32; however, this is in opposition to evidence presented here and elsewhere, including many clinical trials supporting CBP methods.19–22,25,27,29–31,33
There are some limitations to this review. First, there was a limited number of cases, and only 1 clinical trial. This is important as individual cases do not have control groups for comparison; however, there was a trial that did have a comparison group showing structural improvements coinciding with pain reduction. Second, there are limitations to the long-term knowledge of structural correction stability as only two cases included long-term follow-up, though both these cases reported the patient had remained well at a 9-month13 and a 1.75-year follow-up.11 Third, the generalizability of the data is limited to mostly mid-aged persons as the trial was composed of 34 males and 29 females with an average age of 38 (± 18.4 years),3 thus representing a wide range of adult ages of both sexes, however no children or adolescents were included in any report. Fourth, further research should help elucidate more precise treatment extrapolations.
CONCLUSION
There is limited but evolving clinical evidence showing that specific CBP protocols can reduce lateral thoracic translation postures. More research is needed to verify this data and to assess the long-term stability and its application to children and adolescents.