Introduction
Given that the meaning of subluxation has changed over time and given the semantic form of the word developed relatively recently from Latin, our approach to understanding the term examines the speaker’s meaning1,2 on those many occasions where it has been documented. We must examine these linguistic interpretations as they carry the meanings that comprise the overall idea of subluxation.
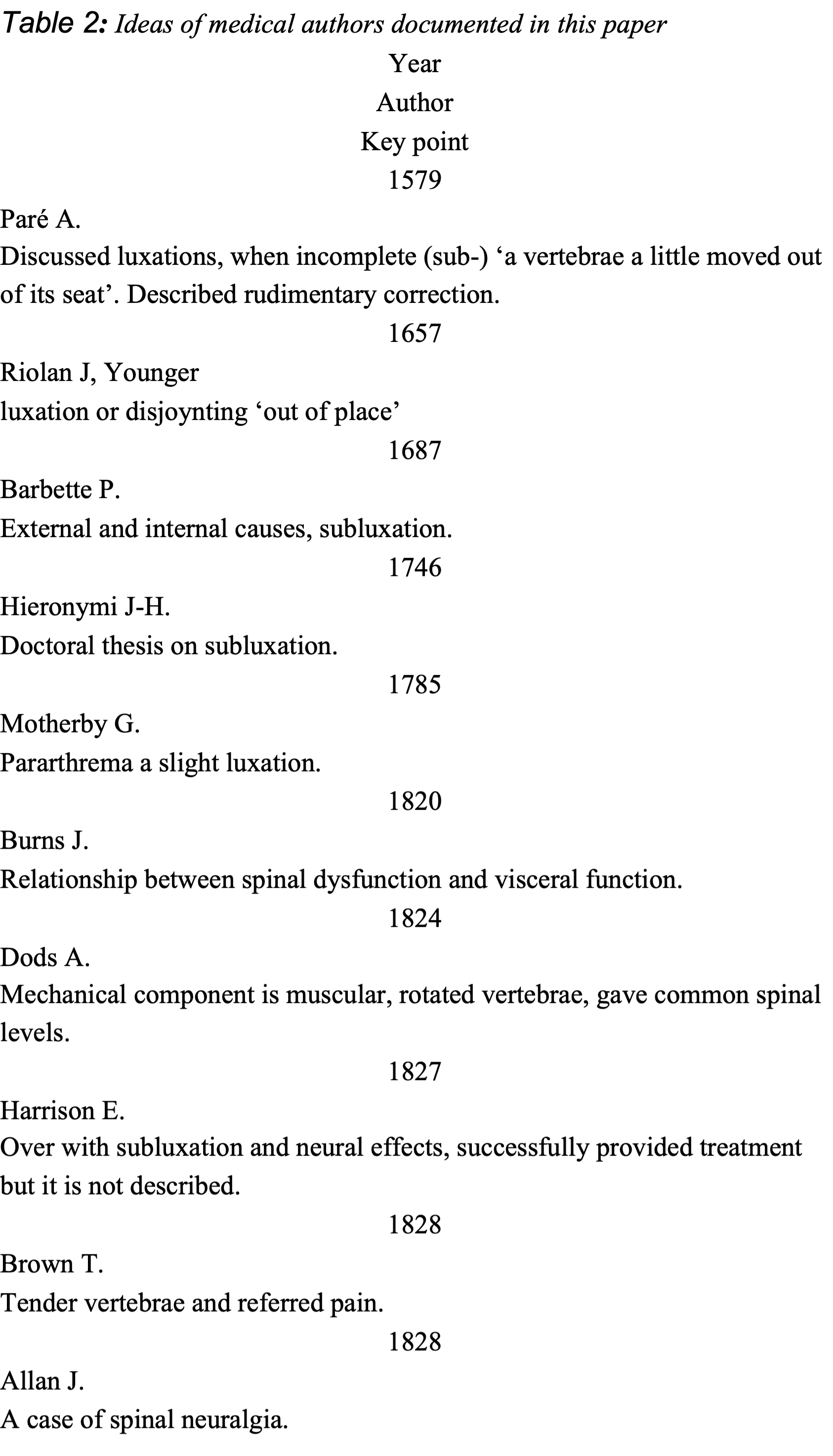
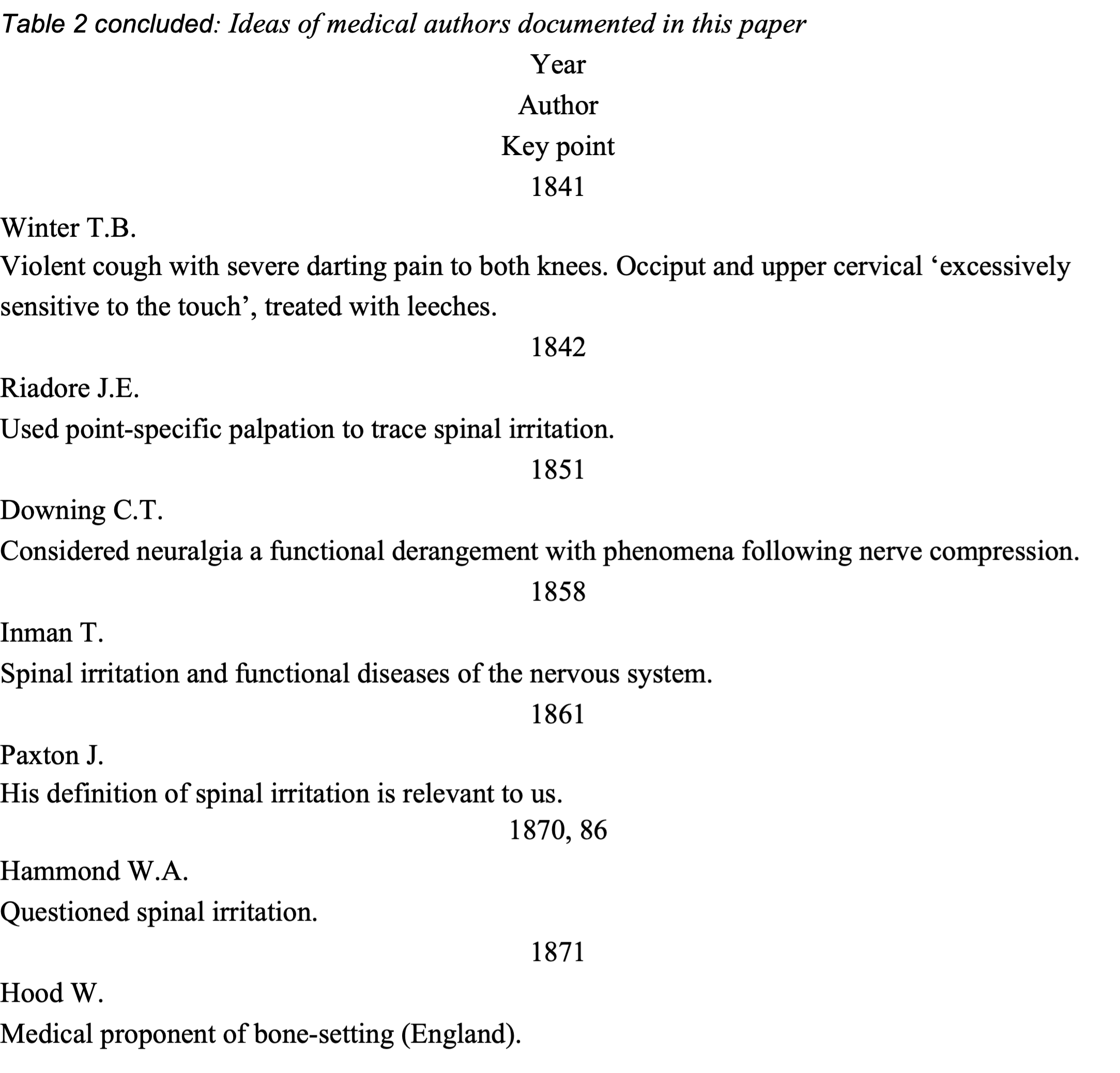
This paper traces various speakers’ meanings as documented in the medical literature to the 20th Century.
DISCUSSION
Origins in Pre-Hieronymi Medical Literature
From 1543
One of us (PE) dated the idea of subluxation to Egyptian medical writings of 1,600BC or so3 while the other (GB) provided a history of subluxation as it evolved from the Greek ‘pararthrema’,4 tracing it from Hippocrates around 500 BC5 through the Nicetas Codex manuscript of the 10th Century.6 We continue the story of subluxation from the year 1543, when Paris physician Jean Tagault wrote the book ‘De Chirurgica Institutione, Libre quinque’ in 1543. It was translated to Italian in 1570.7 The ‘Fifth book’ (libro quinto) opens with a discussion of luxation and its many differences. Subluxation (Subluxatione) is addressed on p. 333 with citation of the Greek pararthrema and is given in mechanical terms:
‘Therefore, luxation, as it is defined by a certain formula, is characteristic of a joint from its native position, or properly said, from its own socket, slid into a strange and un-customary seat, by which its voluntary motion is impeded. Greeks call this exarthrema. Moreover, there are no other differences (as Paul says) beyond that which is taken by the degree, the greater or lesser. For when a joint is fallen from its own seat and has been completely shaken out, by the common vocabulary of genus it is called exarthrema by the Greeks and luxation by the Latins. If the connections move only a little down the side of its concavity we call it subluxation in Latin, and pararthrema in Greek.’
We now report specific texts in ascending chronological sequence.
Paré A. The workes of that famous Chirurgion Ambrose Parey translated out of Latine and compared with the French. Johnson T. London: Cotes and R Young 1634 . Author’s note signed Paris, 8 Feb 1579.
Book 16, starting p 379, is a discussion ‘Of dislocations, or luxations’ with a number of chapters introduction luxations including their prognostics, and treatment. Detail is provided for major joints (knee, jaw, shoulder) and Chapter 12 is ‘Of the luxations of the spine, or backbone’ Paré provides an anatomical description of the spine, referring to the disc as ‘gristle’ with a ‘tough, and (as it were) albuminous humor’ referring to the nucleus. He felt the spine more ‘clearly manifests the industry of Gods great workmanship’ through its arrangement of vertebrae and its inherent stability and mobility. Chapter 13 relates upper cervical dislocation with death. Chapter 14 talks of dislocations of the ‘vertebræ, or rackbones of the neck.’
Paré refers to incomplete luxation, (subluxation) ‘a vertebrae a little moved out of its seat’ and usually with rotation. He felt that such dislocations or strains can be restored in the seated patient with cervical traction and shaking to move every part until the vertebra be restored to its place.
With regard to the back, he felt that vertebrae may be dislocated by external or internal causes. External causes led to dislocations which could not be reduced by external force or thrust, and usually were fatal. He spoke of the most severe type being unable to be reduced by anterior forces, and of a posterior type that could be treated by manual means including a forward thrust and pressing to force the vertebra back into its seat. This could represent the antecedent to Palmer’s idea of replacing by hand. Such reductions were then supported by bandaged splints. Palmer’s great advance was the lack of any need for such ‘post-replacement’ adjunctive support.
One would know of a successful restoration by the smoothness of the whole spine. There was no real differentiation between a dislocation and a subluxation in these discussions, the vertebræ were simply considered displaced out of their seats.
Chapter 18 is a ‘more particular inquirie of the dislocation of the vertebræ proceeding from an internal cause’ and is of great interest. This chapter talks of the nervous ligament binding all vertebrae and the meninges, and these may beget a tumour, or become distended and draw a vertebra into luxation. Paré referred to Galen considering a classification secondary to ligamentous looseness yet the vertebra remained in its place. This is more descriptive of subluxation as it is conceived today. He described different types and gives them as curable or not. This extends the Egyptian view that a lesion could respond to care or fail to, and we consider Paré to represent medical thought of the 16th Century and are intrigued to note his continuation of the Egyptian view from 3,000 years earlier.
Riolan J (Younger). The sixth book of the anatomy and pathology. (Encheiridium anatomicum et pathologicum) London: Peter Cole. 1657. Short title: THE FIRST BOOK OF ANATOMY AND PHYSICK, OF John Riolanus. London: Printed by Peter Cole 1657.
Jean Riolan (the Younger,15 February 1577 or 1580 - 19 February 1657) was a French anatomist who was an influential member of the Medical Faculty of Paris. His father, Jean Riolan (the Elder) (1539-1605) was also a noted French anatomist. Riolan was the personal physician to Marie de’ Medici (1553–1642) for all his life and served King Henry IV of France, then Marie’s son, King Louis XIII of France. We consider Riolan the foremost authority of the 17th Century, his book was fully titled as ‘THE SIXTH BOOK OF THE ANATOMY AND PATHOLOGY OF John Riolanus, THE KINGS PROFESSOR OF PHYSICK. (Encheiridium anatomicum et pathologicum. English)’. We quote directly as written:
‘A sure guide, or, The best and nearest way to physick and chyrurgery that is to say, the arts of healing by medicine and manual operation: being an anatomical description of the whol body of man and its parts: with their respective diseases demonstrated from the fabrick and vse of the said parts: in six books … at the end of the six books, are added twenty four tables, cut in brass, containing one hundred eighty four figures, with an explanation of them: which are referred to in above a thousand places in the books for the help of young artists’
‘Luxation, or Disjoynting, is a Disease of the bone in Scituation, when it is removed out of its place.’
‘There is a two fold Luxation, or disjoynting of a bone; the one compleat, when the Head of the bone is slipt out of its socket, and this is called Exarthrema, a being out of Joynt.’
‘The other is Incompleat, and termed Pararthrema, when the bone is in some measure only removed, and lengthened as it were, which is mostly seen in the subluxation of the Thigh. In an Exarthrema, the Leg seems shorter than it was wont to be; in a Pararthrema it seems longer than usual.’
'The Causes of Luxation and Subluxation, that is to say, of perfect, and imperfect disjoynting of any Member, are external, or internal: The External are, a blow, a violent distorsion, or wrenching, a fall, and extension of a Member. The Internal causes are, a thin Humor, which does relax the Ligaments, or a thick Humor which by little and little, fils the Cavity of the Joynt, and at last thrusts out the bone, by reason of an Anchylosis, which is bred.
‘The other is Incompleat, and termed Pararthrema, when the bone is in some measure only removed, and lengthened as it were, which is mostly seen in the subluxation of the Thigh. In an Exarthrema, the Leg seems shorter than it was wont to be; in a Pararthrema it seems longer than usual.’
Also in the 17th Century a London surgeon, Babette, published advances in medical thinking that included discussions on the circulation and the plague. We find it of great interest that he considered that even the unborn could suffer subluxation.
Barbette P. Thesaurus chirurgiae. London: Printed for Henry Rodes 1687. (The chirurgical and anatomical works of Paul Barbette … composed according to the doctrine of the circulation of the blood, and other new inventions of the moderns: together with a treatise of the plague, illustrated with observations).
'BARBETTY’S CHIRURGERY. The First Part. CHAP. V. Of the Nature, Difference, Signs, Causes, Prognosticks, and Cure of Dislocations in general. '… the laxity of the Ligaments, than it becomes longer the part is painful, chiefly upon motion. In a Subluxation, these Accidents are lesser, and seldom all together. Prognosticks. CHAP. V. Of the Nature, Difference, Signs, Causes, Prognosticks, and Cure of Dislocations in general.
'A Dislocation is a forcing of the Bone out of its cavity and natural place into another, hindering voluntary motion.
'The Differences are taken, 1. From the manner; for sometimes the Bone is altogether forced out of its place, and that is properly called Luxation or Dislocation: Sometimes it is got out but a little or half, which is called Sub-laxation, or Elongation. 2. From the Cause; for sometimes it is from an external accident, as by wrestlings, Falls, or Blows, &c. Sometimes from internal Causes, by the afflux of Humors.
'The Causes are of two sorts; 1. External, Such as are Falling, Beating, Running, Wrestling, and vehement extention, as it often happens to Women in Labour, through the unskilfulness of Midwives; yea, by a violent stroke or fall, even the Bones of the Infant in the Womb, may be dislocated. 2. Internal, By the afflux of Humors, which falling into the Joints, relax and resolve the Ligaments, and so causeth the Bones to slip out of their places.
'The Signs, especially in a lean Body, are manifest enough. The Bone causeth in the place to which it is forced, a tumor or rising; and in that whence it is forced, a cavity. If there be a perfect Dislocation, the Member will be drawn up, and shorter (unless the luxation happen by the laxity of the Ligaments, than it becomes longer) the part is painful, chiefly upon motion. In a Subluxation, these Accidents are lesser, and seldom all together.
'Prognosticks. In Children and other tender Bodies, the Bones may be reduced more easily; but are kept in with more difficulty; the contrary happens in strong and full grown persons: The Dislocation of the Head is mortal, that of the Vertebra’s dangerous; and that which is inveterate is hard to be cured. That which proceeds from an inward Cause, is of a slower Cure, and does easily return. Cure. The Bone forced out, must be reduced to its place, either by the Hands, Ligatures, or Instruments; but by which of these three it shall be performed, the Nature of the affected part will declare. ‘Tis certain, that these four Manual Operations (Extention, Setting, Binding and Well-placing) must here be used as well as in Bones nor the Muscles, but to keep their natural figure. Before you proceed to binding up the Member, endeavour to preserve the part from inflammation and flux of Humors, and strengthen it with the following Medicines. Fractures of Bones. Extention must be made so great, that there may be a cavity between the Bone that remains well, and that which hath been forced away, to the end that in the setting, the one may not rub against the other; whence afterwards are wont to rise very grievious, and sometimes incurable Accidents. In the Setting, care must be had not to wrest the …’
Hieronymi
1746
Hieronymi wrote about subluxation and luxation as his thesis for introduction into the medical profession. He was an obscure figure, and little is known about him. Like so many other theses written by new physicians, he relied on earlier works written on luxation and subluxation, Heister, Pare, etc Hieronymus gives a good outline on the signs to recognize subluxation.
Hieronymi JH. De luxationibus et subluxationibus [thesis] Jena University: 1746. Johannes-Henricus Hieronymi (Figure 1).

The thesis was written in Latin, examined most likely by natural speakers of German, and remarked upon in French. Today’s doctoral students have an easier ride. Our observations from our own, paid professional English translation:
'The luxationibus and subluxation (thesis). Jena; 1746 (Luxations and Subluxations) p 01.
‘Magnificent as the rector as the serene prince master Ernest Augustus Now the rest of the leadership of saxoniae Iuliaci cliviae of the mountains angariae er Westphali.’
'President Georg. Erhado Hambergo (PhD Med, anatomy, surgery, botanty, physics), ‘Summer is license for a medical office to obtain the rights and privileges of doctoralia on 21 Dec 1746’.
'(attributed to) his excellence, Monsignor Baron Jen Clamor August de Busch, private counselor of the chamber of his majesty, and his minister with the imperial court, lord of Walbeck (Funded by King Louis VX of France)
‘Examined by four examiners and a chair person. Johannes-Henricus Hieronymi (awarded) Most Learned Medical doctor by John Henry Jerome, President Jena University’ (p 36).
Our key take-away regarding the constituents of subluxation is: ‘mechanical “altered movement”’, ‘neural “Mild pain than dislocation.”’ Note: It seems that Hieronymi means that milder pain is not a clear piece of evidence in diagnosis if the other points have not been observed), ‘Other “Altered gait.”’
Hieronymi wrote
'Subluxation is recognized:
1) from diminished or difficult movement, or otherwise destroyed movement.
2) from the slight change in placement and form [of the joints]
3) from occasionally increased length [of the joints]
4) from, for the most part, milder pain than in the case of dislocation, which nevertheless is not very clear evidence, if you have not taken out the following [evidence]. Therefore they ought to be considered.
5) a vexed gait of motion, and
6) by the nature of the joint. For instance, less force is more likely to produce a partial dislocation than a dislocation, and the jointed structures of the bones of the elbow are arranged so with the shoulder as with the wrist, and moreover the bones of the wrist and metacarpus, the knee, the bones of the tarsus and metatarsus—these are disposed towards partial dislocations more than true dislocations on account of their wide surfaces, or in reality more flat, and on account of having many tough ligaments.
‘That is to say, the bones, whose surfaces are broad and less circular, indeed easily yield to the first inflammation, but are not able to be moved to a large space, unless the inflammation would become too large and rend the ligaments, because the adjoining bones, which at the same time ought to be moved, they weaken the inflammation little by yielding, indeed those adjoining bones increase their resistance. (Inaugural Medical-Chiropractic Dissertation On Dislocations & Partial Dislocations by Hieronymus (section 15, pages 12-13))’.
Post-Hieronymi
1746 - 1890
Motherby G. A new medical dictionary 2e. London: Printed for J Johnson St Paul’s Churchyard and J Robinson Paternoster-Row, jun and J Murray Fleet Street. 1785
Motherby confirms Bovine’s work of identifying the Greek ‘pararthrema’ from the Latin ‘subluxatio’: ‘PARARTHREMA. A slight luxation. A tumor from protrusion, as an hernia.’; SUBLUXATIO. Subluxation. It is where the head of a bone is not quite out of its socket, but rolls upon the brim.’ Here Motherby is recognising and classifying pararthrema as a slight luxation and then subluxation, as:
‘subluxatio as movement change within the joint (rolls upon the brim) beyond being in its normal place.’
Motherby’s introduction recognises the input, including some levels of sophistications, from Arabian thought, contributing to the ‘Materia Medica’ of Hippocrates, noting others such as Galen, Aretaeus and Trallian. He notes that about the middle of the 15th Century medical ‘learning began to diffuse itself throughout Europe’ with Hippocrates and Celsus again being ‘received’. He noted the ‘Hippocratical methods of concluding from observations founded on experience, was again restored.’ This point helps understand the reports of association between clinical findings and specific spinal levels that emerged in the 19th Century.
Dods A. Pathological observations on the rotated or contorted spine, commonly called lateral curvature. London: Printed for T. Cadell, in the Strand, and W Blackwood, Edinburgh: 1824.
The mechanical constituent is given as muscular secondary to postural; specific cause was rotated vertebrae, most commonly upper Lx, Dx 5, 6, Cx 4, 5. Dods argued the contorted spine was ‘an affection totally independent of any disease or diseased action, either in the vertebræ themselves, or in their connecting ligaments or cartilages’ … being ‘produced by peculiar affections of the muscles of the back’ exerting a rotary effect on the spine (p. 30). In contrast to Harrison’s view that spinal contortion was not a muscular disease Dod argued to the contrary. Harrison, whom we next examine, ascribed all spinal complaints to ‘one common cause … the connecting ligaments of the vertebræ’ (p. 59).
Dods wrote:
‘I have recourse to friction, manipulation, position and exercise’ (209) describing manipulation as being ‘long used in the surgical art, for the replacement of displaced bones; and for this purpose I use it in the contorted spine.’ The intent was to use friction to relax the muscles allowing ‘the vertebræ will rise of their own accord, from their new, and resume their former, or natural situations’ (p 212).
He wrote of the ‘endeavour to return the displaced vertebræ to their natural situations,’ noting unilateral muscle contraction rotated the vertebra. This was to be corrected by rotatory motion as gentle applied force, contrary to that caused by their muscles.
We consider Dods’ work to be an informed discussion on gross distortions mainly as lateral curvature (scoliosis) in contradistinction to the rotated or contorted spine. He argued that scrofula was over emphasised as a cause (referring to Potts - 1779): Potts’ logic was curved spine = hump back = kyphosis. He felt that postural exertions were a significant cause and that causative vertebrae were very painful to touch (palpation). Treatments were all mechanical in nature; boards, collars, chairs, drilling as in soldiers.
Dods makes the interesting point that to date the proposals for treatment represented the individual writer’s views, as eminence-based medicine (Part II, p. 164). The polar views were a structural disease of the vertebræ (after Potts) and muscular contraction (Dods) with Harrison being an outlier considering ligaments. Dods argued for cumulative effect of vertebrae upon vertebrae and inferred the muscular contraction was caused by ‘mal-position’ but does not state ‘of a vertebra’.
Harrison E. Pathological and Practical Observations on Spinal Diseases. London: printed for Thomas and George Underwood. 1827.
Spinal dysfunction, later called subluxation, with an altered state of nervous tissue, was known to British surgeon Harrison. The significance of Harrison’s work is that from about 1820 he argued a role of spinal dysfunction in the health and well-being of the individual, through spinal dysfunctions affecting visceral function.8 He provided generous descriptions of the clinical effects of such changes. He described the cause as changes to the anatomical relationships of the nerves and their filaments exiting the spine:
‘We cease to be surprised that luxations of the vertebræ should produce such an endless train and succession of perplexing symptoms’ (p. 50). The ‘obvious cure is to restore the displaced bones to their natural situations.’
In the 1820s Harrison recorded what could be considered the first case report of manually correcting subluxation. He treated a man who had fallen from a horse and lay motionless. Harrison wrote:
‘I visualise that he had a subluxation … I believe that the vertebrae was displaced compressing the cord and phrenic nerve’.
Harrison treated the neck and the man recovered and rode off.9 ‘Harrison described the contact areas on the vertebra for adjustment, was the first to complain about repetitive strain injury while treating the patient, designed a hand held instrument to assist the thrust, formed a theory of “chronic” subluxation, used vertebral “prominence” and position as a diagnostic sign, discarded exercise as a form of treatment for subluxation and used the word “manipulation” to describe his treatment. Upon the occasional death of his clients, he confirmed the vertebral organ neuropathology by autopsy’.9
Harrison related spinal changes with health changes mediate by altered organ function (p. 25). He saw the spine as influential on the ‘complicated functions of the thoracic, abdominal, and pelvic viscera’ (p. 32)/ He was not, as suggested, entirely reliant upon ligamentous involvement, saying ‘I think we are still bound to pay some regard to the ligaments’ (p. 37) in the context of explaining Mr Pott’s view, however he did hold the position that affections such as those studied by Potts generally begin in the ligaments and pass to the bone and cartilage. He was presenting a counterpoint to Mr Potts’ claim that affections always began in the bone. He countered Mr Dods by name and denied his suggestions he ascribed all ailments to ligaments (p. 89).
He wrote ‘8 years since …’ meaning he first spoke of these matters in 1820 (preface xiii) and commented on the experienced practitioner’s view that ‘luxations of the dorsal and lumbar vertebræ are impossible under any circumstance’ (p. 7). Agreed vertebral dislocations seldom appear in those parts, ‘I am unacquainted with any case of luxation in the dorsal vertebræ … incomplete luxations’ on visual examination of the spinous processes, ‘this subluxation’ … ‘scarcely a complaint can arise in which they do not participate’, adding ‘in recent cases these subluxations are easily replaced’ (p. 12). Muscle ‘attached to the articulating fibrous structure and not to the vertebræ it encloses’ describing the musculotendinous junction with the capsules about the SMU and gave Ricketts as the cause of lateral curvature and caries of the anterior curvatures.
Harrison described luxations as of a significance affecting blood flow giving turgidity, bowls are obstinately constipated and haemorrhoids often prevail to a great degree: ‘A dislodgement of other abdominal viscera disturbs their respective functions, and lays the foundation of bad health’. We consider this relates to the status of health we today consider as well-being.
He presented a collection of cases ‘because of the occurrence of vertebral luxations, independently of external violence, appears to be commonly denied.’ Nine cases are presented in detail, with plates.
Harrison gave a thorough anatomical description of the spine, including the thoracic concavity on the left for right-handed persons, and on the right for left-handed persons, and described centres of movement between vertebra and how changes in these were the true source of spinal deformities. Elongation of the ligaments and displacement or luxation of the vertebræ is most common:
‘If one of the articulating bones be either wholly separated, or only partially removed from the other, the disorder is called a dislocation, luxation, or disjunction. “luxo” loosen or disunite. Displacement is also frequently used to mark the lower grades of dislocation, but very improperly, since we employ it to denote the changes in soft parts, as well as the joints.’ …. ‘… it is really of no importance whether it be said that the vertebræ are luxated or displaced’ (p. 133).
All he contended was that the articular ligaments elongated before the vertebræ change their position. Harrison proposed two stages of luxation:
‘one of the bones wholly removed - complete, perfect, entire. In the second the bones still remain more or less in contact with each others. The latter example is denominated an imperfect dislocation, a subluxation, or partial disjunction’ and cited Hippocrates ‘articulations which slip, and are disjointed, do not always fall out entirely, nor are they invariably luxated in the same manner.’
Harrison felt small luxations are more easily re-instated, but was not clear if Hippocrates was discussing spinal joints, as he continues to discuss the hip, thigh and arm, joints of the feet
Brown T. On Irritation of the Spinal Nerves. Glasgow Med J 1828 May;12:131-60. First read January, to the Medical Society of London in January 1823 (from Teale). Cited by Allan, 1828.
Brown gives a detailed description of referred pain from a ‘tender part of the spine’. He describes a ‘young lady with pain in her left side, and numbness and pain of the left arm and leg, distinctly connected with tenderness situated about the lower of the dorsal vertebrae.’ He also identified a ‘similar state of the 2d or 3d cervical vertebrae, which occasioned pain in the left side of the neck. commencing between the angle of the jaw and the mastoid process.’ The patient declined blistering and on surgical incision about the spine instead, experienced ‘great irritation.’
In discussion he noted mid lumbar vertebrae associated with severe abdominal pain and proceeded to present a case from 1821. Another lost her voice in association with tenderness of cervical vertebrae. He presented other cases and a discussion on what we now understand as vertebrogenic pain, pain referred from dysfunctional vertebrae. This is one of the earlier discussions on pain referral from the spine. He proposed mechanisms which, while crude with respect to Palmer’s painless approach, were advanced for his time.
Brown is considered by Hammond of New York as the first to use the term ‘spinal irritation.’ We note that the first to use the term spinal irritation was not Brown. The Scottish physician John Burns M.D. wrote of it in the fifth edition of his work, ‘The Principles of Midwifery’, published in 1820, which includes a chapter on Cerebral and Spinal Irritation:
Burns, J. The Principles of Midwifery. Fifth edition. London. 1820:667-89.
From the above we consider that the relationship between spinal dysfunction and visceral function emerged in Britain during the 1820s.
Allan J. Case of spinal Neuralgia. Glasgow Med J. 1828 September:406-9.
Informed by Brown’s paper on ‘Irritation of the Spinal Nerves’ Allan presents a case of a young adult female presenting with pain under the left breast sometimes extending down to her ilium and up towards her left shoulder, described as a type of burning. On examination Mr Allan found three or four very tender ‘middle dorsal vertebrae’ which resolved her pain following the application of leeches to that area. The longer term (7y) pain history included an acute onset when kneeling, in her left knee, thigh and loins, accompanied by limping. She reported menstrual irregularity. A selection of other tinctural treatments about the spine resolved the matter. Allan’s critical reflection on the case considered the neuralgic symptoms overpowered underlying a bowel complaint accompanied by worms. In terms we consider clumsy today he proposed that the spinal irritation gated the visceral pain.
Teale TP. A treatise on neuralgic diseases . dependent upon irritation of the spinal marrow and ganglia of the sympathetic nerve. London: Gunnel and Shearman, printed for S Highley 174 Fleet Street. 1829.
Teale advanced the understanding of a differential in expressed pathology from the known and accepted gross phenomena to ‘slighter forms of the disease’ and referred pain with reflex loops. He took the accepted knowledge of disorders of the nervous system and brain to be one form of clinical presentation, and disorders of the sympathetic system of nerves and its ganglia to be another, less obvious, other. He acknowledged this would be difficult to establish by experiment and relied on analogies. He took the position that ‘many nervous affections of the viscera ought not to be considered as diseases of the viscera themselves, but as symptomatic of disease in those particular ganglia whence their nerves are derived.’
Teale acknowledged Brown (1828) and John Darwall whose contribution ‘Some forms of cerebral and spinal irritation’ in the Midland Medical Reporter and in the book ‘Plain Instruction for the Management of Infants’. He also acknowledged as important in the development of his thinking RP Player who, in a letter to the editor (Quarterly Journal of Science vol 12 p. 248) dated 10 December 1821 wrote:
‘I take the liberty to submit to your notice a pathological fact, which has not, to the best of my knowledge, been generally remarked, and attention to which, as far as my own experience goes, promises some diminution of those difficulties with which the healing art has to contend. Most medical practitioners who have attended to the subject of spinal disease, must have observed that its symptoms frequently resemble various and dissimilar maladies, and that commonly the function of every organ is impaired whose nerves originate near the seat of the disorder. The occurrence of pain in distant parts forcibly attracted my attention, and induced frequent examination of the spinal column; and after some years’ attention, I considered myself enabled to state, that in a great number of diseases, mort(a)l symptoms may be discovered about the origins of the nerves which proceed to the affected parts, or of those spinal branches which unite with them; and that if the spine be examined, more or less pain will commonly be felt by the patient on the application of pressure about or between those vertebr(a)e from which such nerves emerge.’
A distinction between cause and effect was not possible at that time:
‘This spinal affection may, perhaps, be considered as the consequence of diseases, but of its existence at their commencement any one may satisfy himself; and this circumstance, combined with the success which has attended the employment of topical applications to the tender parts about the vertebrae, appears to indicate that the cause may exist there. Prejudice sometimes operates against the idea of connexions so remote; but in many instances patients are surprised at the discovery of tenderness in a part, of whose implication in disease they had not the least suspicion.’
Teale’s treatment was traditional and not in the manner of manipulation or bone-setting as reported by his contemporary Harrison. He diagnosed a vertebral level on the basis of point tenderness to palpation and associated with it clinical symptoms for example, C3 and C4 and vertigo (Part 24). He did not report a manual thrust as an intervention, however such was reported by Harrison.
Teale went a step further and associated what later commentators10(p59) considered ‘Type O’; or ‘organic’ conditions with the spine, in Teale’s case diabetes. He gave the lower thoracic ganglia as implicated (Part 40). He also related tender cervical vertebrae with some affects of the heart, writing:
‘This state of the heart, I have already remarked, depends generally, if not always, on a morbid state of the cervical ganglia of the sympathetic.’ He gave a case (XI) of a female who ‘has been five months affected with palpitations and pain in the region of the heart. The palpitations occur in violent paroxysms several times during the day; at night they are less violent, but are frequently troublesome. The pain is referred to the immediate seat of the heart, and occasionally spreads over the lungs. There is often an oppressive tightness across the upper part of the sternum; and also pain darting down the arms and over the scalp. In other respects she enjoys good health.’ He associated this with ‘great tenderness in the five upper cervical vertebrae’ and treated the area, with leeches, to some effect and then with oral saline solution and turpentine liniment to achieve resolution.’
Also, a range of stomach disorders were associated with spinal nerves and the splanchnic nerves from the thoracic region: ‘… to be connected with tenderness on pressing some of the middle or lower dorsal vertebrae; and on removing the tenderness in the spine and neighbouring parts by proper remedies, the stomach affection and attendant symptoms have been almost immediately relieved’ (Part 48).
In his discussion on angina pectoris he states ‘I am fully convinced that it is to the nervous system we must look for the seat of this disease’. Teale advanced the understanding of a differential in expressed pathology from the known and accepted gross phenomena to ‘slighter forms of the disease’ and referred pain with reflex loops. He took the accepted knowledge of disorders of the nervous system and brain to be one form of clinical presentation, and disorders of the sympathetic system of nerves and its ganglia to be another, less obvious, other.
He acknowledged this would be difficult to establish by experiment and, as we have noted, relied on analogies. He took the position that ‘many nervous affections of the viscera ought not to be considered as diseases of the viscera themselves, but as symptomatic of disease in those particular ganglia whence their nerves are derived.’ Teale’s conclusion (Part 120) is a discussion on somato-viscero-somatic reflexes:
‘Whci … hese diseases have proved unusually obstinate, or the treatment has entirely failed, 1 have generally ftoid that they hare’ been complicated with others. Th bones osr intervertebral cartilages are ilk some instances affected, and the nervous structures are thereby disposed to repeated relapse. The h…f may be the soat of incipient organic changes, which seems to keep up irritation in the nervous masses from which its nerves are derived ; or the stomach may have under-gone some alteration of structure, which, by its continued irritation, may keep up a disordered state of the ganglia, and thereby produce obstinate neuralgic symptoms’ (sic as published).
In many respects Teale may be seen as laying the foundation for Palmer’s claims about the relationship between spinal dysfunction and health disorders (colloquially collectively called disease or literally dis-ease or altered wellbeing). Palmer’s great contribution was the adjustment of these spinal dysfunctions by hand. During the active phase of Palmer developing his ideas about ‘subluxed vertebrae’ or these came to be called first by a graduate of his, Smith, subluxation.
Beale LJ. A Treatise on Deformities; exhibiting a view of the nature and treatment of the principal distortions and contractions of the limbs, joints, and spine. London: John Wilson 16 Princes St Soho. 1830.
Subluxation is NOT mentioned, perhaps representing an inflexion point in the history of the idea of subluxation. Beale considered categories of gross distortions as lateral deviations and described these is the gross manner, and spoke to disease processes of the vertebrae themselves, and also of the disc, and smaller dysfunctions, ‘partial luxations (subluxations) of the cervical and lumbar, if not dorsal vertebræ’ identified by palpation of tenderness (p. 201).
Our findings are that the deviations of 1 or 2 vertebræ were given to suggest partial luxation and that altered intervertebral spaces were noted as of clinical importance. Beale reported that spinal issues arose in children and were not observed until they started to walk. He does not state what these are however these descriptions would hold meaning to today’s chiropractor as subluxation due to the deviations of the spinous processes. He reported a child of about 5y with prominent 3rd and 4th dorsal but otherwise in good health. Beale associated pain and difficulty with rotation when cervical vertebrae were involved (today this is termed ‘decreased ROM’) associated with depressed breathing.
Beale associated spinal levels with organic dysfunction as signs. He gave a rudimentary well-being paradigm involving food and good environment with gross machine-based treatments, and some local irritation to the skin such as moxa.
Wark D. Cases of Spinal Irritation. Glasgow Med J. 1831:132-8.
This is one of the earlier papers we can identify in which ‘spinal irritation’ is addressed. It sits after Harrison’s work which reported subluxation, and follows works that introduced the concept of spinal neuralgia. Wark considered that if patients were properly examined there would be many more cases reported of spinal irritation.
His cases are reported with granular clinical detail however his therapies, while appropriate for the times, can only be considered as crude.
Turnbull RJ. A case of spinal irritation. Boston Medical and Surgical Journal 1833;711:341-44.
Turnbull makes reference to Teale (London, 1829) thus demonstrating the transmission of the ‘idea’ to North America. He commences his case report by stating ‘we know of no other medical fact, of recent observation, which has illustrated the nature of so many diseases. and those too of an anomalous and obscure character, as the above condition of the spinal cord’ referring to spinal irritation. The patient was a 19 yo female with dysmenorrhoea and menorrhagia plus neck and shoulder pain, with a hacking dry cough. The usual materia medica gave not the slightest relief. His clinical thinking went to spinal irritation and on palpation he found pain from C2 to C6, about T4/T5, and T12/L1. The case is replete with descriptions of his local interventions and the patient’s response and can be summarised as resolving. The intervention that seemed effective was counter-irritation at the named spinal levels. He noted that care has to be taken to not create too great an inflammation about the spinal site as that would be counter-productive by irritating adjacent areas.
Turnbull concluded this case with an informed discussion on the neurology and its mechanisms to allow the presenting complaints and recommended that in similar cases the patient should be examined with regard to their spine. This is a clear statement associating specific health disorders with small spinal dysfunctions, amendable to intervention, regardless of its crudity, to specific spinal levels known to have neurological relevance.
It is interesting to note the reference to Teale (London, 1829). In a subsequent issue unattributed references were made to a writer in the ‘Edinburgh Medical Journal’, the ‘London Medical Gazette’, and the ‘Dublin Journal of Medical and Chemical Science’. The Boston Medical Journal published authors from a wide geographic distribution. Turnbull wrote from Charleston CS, another from Ohio, and from Aberdeen. It must be remembered that at this time public buildings were erected in Boston with funds from the illegal opium trade in China.12 Could it be that the idea of subluxation was disrupted by the 19th Century opium wars?
Barrows HA. Case of spinal irritation. Boston Medical and Surgical Journal. 1834;8:70-1
Barrows reported a case of a 46 yo male labourer ‘naturally hardy and of good constitution, free from hereditary taint’ and a 5-year history of morbid symptoms of the chest, with pain in the side, disturbed rest, and general debility. A comprehensive physical examination is reported and his previous physician had abandoned. On spinal palpation T6 and T7 were ‘found exquisitely tender.’ Cupping, scarification and vesication (blistering) were applied about the spine and the convalescence was steady and uniform. No medications were used internally ‘save a slightly tonic preparation’ with reliance on the ‘“backbone” treatment’.
Nichols A. On irritation of the nerves. Read before the Massachusetts Medical society 1836:May 25.
Nichols’ presentation can be taken as descriptive of the medical thought in North Eastern America in the mid-19th Century. McDowall13 has identified how these thoughts could have impacted the young Palmer. The nervous system was understood as divided into sensory and the ‘ganglionic nerves of life.’
Nichols consolidated thinking about health by noting the value of 'exercise and the ‘sanatory power … light … the direct rays of the sun.’ He stated ‘a spare or vegetable diet increases the power of the intellect and the activity of the sentient and motor filaments.’ He acknowledged the role of the ‘ganglionic nerves to effect the contractile coats of the arteries, capillaries, veins, &c.’, important for their function. He categorised diseases into four: ‘neuralgic, affecting principally the nerves of sensation; spasmodic, affecting principally the nerves of motion; inflammatory, febrile and organic, affecting primarily the ganglionic nerves; and mental, affecting the moral and intellectual portions of the nervous system.’
Nichols used palpation about the spine to identify ‘tenderness at the origin, in the spinal chord, of the nerves which endow with sensation the parts involved in the disease’ (p. 373) and was able to reproduce the ‘paroxysm … in greater or lesser degree’ … by pressure on that area of the spine.
He reported that localized irritation in the spine was associated with a ‘very large proportion of chronic complaints, organic and functional, - complaints, which differ essentially from each other in their symptoms, progress and termination, have causes many eminent physicians among us to be rather skeptical in regard to the modern doctrine on this subject.’ That doctrine is taken as spinal irritation, today’s subluxation.
He extensively explored the doctrine of spinal irritation and clearly noted ‘the doctrine is not that the spinal chord is compressed, but that the portion which is diseased, conveys to the nerves preceding from it, its own sensitivities’ (p. 376). He made the point that the covering of the vertebræ being supplied with nerves there from, the shortest conductors of impressions to their centers, by their own condition, indicate that of their origin. This can be taken as an early attempt to describe what we now understand as the innervation about the spinal motion unit, the disc and the ligaments, and the facet joints, and a role for the recurrent meningeal nerve (p. 366).
Nichols went on to associate constitutional diseases with spinal irritation, an early claim of a relationship between small spinal dysfunction and well-being (p. 377). He also described spinal reflex loops, known today as somato-visceral and viscero-somatic, relating neuralgia of the face with, for example, ‘acrid matter in the intestines or elsewhere.’
Of relevance to Palmer’s claims of disease being caused by spinal dysfunction, Nichols stated:
‘… I might go over the whole catalogue of diseases, and show that the irritability of some portion of the nervous system increased or diminished, is, if not the whole, an element of each, - an element of sufficient importance to require attention in the treatment of every case which occurs in the practice of physic’ (p. 386, 7).
Not only does this claim by Nichols closely resemble Palmer’s claim of some 60 years later, it also speaks of Palmer’s ‘too much or too little.’ Nichols’ main treatment approach was to create local irritation at the spinal level on the theory ‘the same stimulant, suddenly and largely applied, exhausts the irritability which, by a slow and sparing application, increases it’ (p. 374). His main approach to treatment was to remove, if possible, the original irritating cause (p.387) He frequently did this by applying counter-irritation, often as moxibustion (cupping).
Serny JB. Spinal curvature: its consequences and its cure: illustrated by the history of thirty-three cases successfully treated. London: self published. 1840.
John Serny was an associate and follower of Edward Harrison. Serny gives the case of Miss Boddam, 15 yo, who caught cold and then had a stiff neck, looking awkward with it. He states one of her ‘teachers of the school said to her “my dear, I will make you well very soon;” and, at the same time, twisted her neck forcibly, which caused her to faint, and hemiplegia of the right side, and paraplegia also, immediately followed.’ This may be the first recorded case of an adverse event associated with neck manipulation. On there being no resolution, the girl’s parents placed her under the care of Harrison and Serny where examination revealed ‘a large swelling about the atlas, and the dentata also, and a small lateral curvature of the spine, below the right shoulder blade.’ The girl was treated twice a week ‘every time making the semblance of the reduction of subluxation of the atlas, by gentle extension only’ (p. 38). On the encouragement of Harrison Serny eventually delivered ‘the real attempt’ after a month, ‘I made a strong extension of the neck, with a semi-rotation, and fully succeeded, not without great attendant anxiety, as Miss B. remained for some time in a state of insensibility.’ Miss B. improved and three days later had ‘fully recovered the use of all her limbs, and felt quite well.’
Serny also gives a case of a 24-yo-male with outward curvature attended with affection of the heart and of the sight ‘cured by Dr Harrison’ (pp. 54-5). Subluxations were found at three cervical and the five upper dorsal vertebræ; ‘all of which are tender, stand irregularly, and at unequal distances from each other.’ Harrison’s intervention is not described but it is noted that ‘The eight vertebræ … have been, for some time, restored to their natural situations’ and ‘The palpitations have entirely left him’ along with other reported health improvements including restoration of the eyesight.
A section (from p. 72) of Serny’s textbook makes general observations regarding spinal curvature, postural distortions, and describes subluxations in the extremity joints, with illustration plates of this and other reported patients. His 30th case describes multiple subluxations causing paraplegia. He reports Harrison as reckoning that the cause of the paraplegia was in the back, suggesting that in future ‘the medical practitioner will … neglect his duty, unless he examines into the condition of the backbone’ (p. 83).
Serny acknowledges Harrison as his teacher and reports perhaps the first adequate observations of subluxation and their correction with health affections and their resultant improvement. Serny earlier published on local inflammation and diseases of the eye14 at which time he gave his position as an oculist.
Winter TB. Case of spasmodic cough from spinal irritation. connected with deranged secretion. Provincial Medical and Surgical J. 1841;May:164-5
Winter presents the case of a 10-yr-old male ‘of strumous’ (goitrous) ‘build and highly excitable temperament’ with a very violent cough and severe darting pain in both knees continuing for 6 days from which the knee pain worsened and both arms showed spasmodic motion, especially the right. Fever was not present to any degree and the boy was able to sleep and breath easily. Blistering and leeching the throat provided no relief and as the condition became more constitutional, irritation of the brain and spinal cord was suspected.
On palpation the occiput and upper cervical vertebræ were ‘excessively sensitive to the touch.’ Six leeches were applied directly to this spinal level and with the taking of a ‘powder of calomel, rhubarb, and James’s Powder’15,16 gave fast relief. Leeching was again applied to the still tender upper cervical vertebræ. The symptoms varied and both the neck and the sacrum were cupped and an enema applied and eventually things settled. Winter’s conclusion was that ‘irritation at the origin of the nerves that supply the muscles of the throat, the effects of that irritation being manifested only at their sentient extremities’ (knees) and a purging of the bowel implicated the liver.
An interpretation of this case is that in addition to an underlying systemic disorder perhaps associated with the goiter, upper cervical subluxation produced coughing and perhaps constipation, the knee pain. In lieu of adjustment local irritation about the upper cervical complex was created by leeching and other matters settled with the turpentine enema and assorted powders.
Riadore JE. A treatise on irritation of spinal nerves as the source of nervousness, indigestion, functional and organical derangements of the principal organs of the body. London: J Churchill Princes Street Soho. 1842.
John Evans Riadore was a friend of John Serny, and was a follower of Edward Harrison’s method of spinal treatment. Along with others Riadore considered the neural involvement complex and including ‘the great sympathetic, and par vagum.’ (vagus nerve). He provides a generous discussion of subluxation:
‘In recent cases of spinal curvature, this subluxated form is decidedly most commonly met with in practice; its magnitude, of course, will depend upon the number of vertebræ subluxated … when one vertebra forms a slight exception in the regularity of the spinal line, either by height or distance from its fellows, a serious train of nervous symptoms may supervene that are not particularly distinguishable from those arising from other causes …’ (p. 87).
Riadore was informed by Harrison, Brown, Bell, Hall, Carpenter, Granger and others writing in the field of clinical neurology and physical medicine. His Chapter VIII explored nervous affections and the involvement of cranial and spinal ganglia, local neuralgiæ and functional diseases of a viscus to its nerve supply, including the splanchnic system. He gave a cause as ‘spinal irritation’, not specifically subluxation, however significantly he spoke to the concept of too much or too little with reference to neural flow, a concept developed in detail by Palmer and re-iterated by Homewood.17
Riadore wrote:
‘… it seriously behooves us to make ourselves acquainted with the characteristic symptoms of excessive presence of nervous energy, in contradistinction of inflammatory action, and its natural tendency, under certain circumstances, to continue a nervous affection, or to terminate in inflammatory action, and consequent varied changes of organic structure.’ He continued ‘To distinguish the symptomatic signs of insufficient supply of nervous energy to some organs …’, which became essential principles of chiropractic.
He used point-specific palpation to determine and trace spinal irritation, an idea later developed and refined by Palmer as nerve tracing. The fact that this clinical approach was well know within medicine3–6 tells us that Palmer was abreast with contemporary approaches and that there was substance behind his idea of nerve tracing. Riadore used this approach to make correct diagnosis of ‘various affections, such as organic, functional, inflammatory, rheumatism, &c., …’.
Whilst understanding and describing small dysfunctions in the spine as subluxation, he did not connect this with a topic he explored in detail, spinal irritation. He showed visceral dysfunction relating to over- or under- nerve supply and relied on medical interventions such as tinctures. He was able to describe displaced vertebrae and identify them also by percussion and palpation, but did not propose a mechanical resolution, in spite of Harrison having so reported.
Riadore reports 1 particular case that some 40 medical ‘men’ were unable to determine a cause and which was ultimately referred to and treated by Harrison. The report reads today of a post-trauma cervical subluxation over several segments, and Harrison’s intervention from 15 November 1831 included cervical traction with the intent ‘to replace all the vertebrae’ which apparently succeeded and by the end of the month ‘her symptoms were resolving’. Continued treatments about the spine resulted in excellent health by 12 February 1832. It seems a persistent subluxation was present as it took until the end of July before examination by a number of practitioners declared her spinal column to be excellent.
The vogue was surgical intervention and the preference for this led to overlooking the possibility of manual ‘setting the bones,’ a traditional approach seemingly employed by those seen as less educated, such as Harrison, by the medical elite of London.
The idea of clinical presentations related to spinal irritation was also reported at this time (1842) in the United States, with two such case histories being documented in the ‘Am J Med Sci (1842;IV:176).’ One was a ‘short convulsive nervous cough’ identified by heavy digital percussion of the ‘middle dorsal’ vertebrae, the other ‘violent fits of hiccups’ related by percussion to T4 to lower. Both cases were attributed to the London Medical Gazette, 4 February 1842.
Riadore notes (p. 79): ‘the spinal column became occasionally incurvated in consequence of incomplete or sub-luxation of the vertebrae’. Palmer can only be considered as being well informed with medical terminology when he spoke of subluxed vertebrae and ‘sub-luxations’.
Author GB reviewed Riadore and his main concern was that he was considered more influential by some than he felt deserved, and concluded ‘Riadore wrote an interesting book on spinal irritation, but this was not considered as an important work …’. GB considers Riadore not to be influential in the early developing years of either osteopathy or chiropractic. His main point being that Riadore learned spinal manipulation from Harrison and Serny. Serny acknowledged Harrison as his teacher in his work on Spinal Curvature (1840).
Morris BR. Observations on spinal irritation. BMJ. 1843;Sep 9:497-90.
The mechanical constituent is given as: ‘all cases have tenderness on pressure over the vertebræ’. Neural constituent is differentiated between organic pain and reflex pain and suggested both sites needed to be considered in treatment.
Morris stated it was ‘scarcely possible accurately to define irritation, it so closely approximates, and so often runs into inflammation’ (opening par p. 487). He continued by showing ‘different morbid actions produced according as different parts of the spinal cord are in a state of irritation.’
The examples given were ‘pains in the scalp, shoulders, arms, cramps in these regions, difficulty in deglutination, nervous cough, disordered digestion, hiccough, dyspnoea’ associated with the cervical spine; ‘nervous pains in the integuments of the thorax, and perhaps abdomen, more particularly the submammary and sternal pain’ when the dorsal portion is engaged, along with ‘disordered digestion, lassitude and inaptitude for business, &c.’, and regions of the loins, genitals and lower limbs affected with irritation in the lumbar spine. He acknowledged sciatica was associated with sacral irritation. The symptoms were described as ‘only occasionally present, but in severe cases some of them are never absent.’
Morris stated little was known with any certainty regarding the origin of spinal irritation, considering ‘it could originate in local causes affecting the spinal cord, not subsiding but keeping up the irritation once established - or whether it is induced in the nervous centre by disease of a distant organ, either functional or organic, by a reflex action, as is supposed by my old teacher Dr Graves.’ Morris held the opinion it could be either and that both the organ and the spine required treatment. He held ‘it often happens that disease is established in the spinal cord by reflex action, that the distant organ may become healthy, and yet the irritation still remain in nervous system.’
The vagueness of many diseases could be associated with specific pain in the spine and both were worsened by palpation of the spinal region: ‘I believe that in cases of spinal irritation we shall find tenderness on pressure over the vertebræ, in that part of the spine where the disease exists, always present - an invariable symptom’ (p. 488).
Morris went on to describe abdominal pain associated with the mid-dorsal spine, nervous cough with both cervical and dorsal spines, and referred to Dr Ducros of Marseilles who give nine cases of asthma relieved by applying ammonia over the cervical vertebræ about the origin of the pharyngeal plexus, ascribing the clinical benefit to the principle of counter-irritation. A range of other cases from different practitioners was given and discussed.
On interest is his view that ‘some cases of spinal irritation will occasionally yield without local treatment’, saying these were mostly reflex irritations from an organ. His conclusion was ‘that much could be done by directing some of our treatment to the spine, even when the irritation does not exist idiopathically.’ He considered it a mistake to treat ‘either or’ and that better results were achieved by considering the complete clinical picture of organ and spine.
The treatise by Morris may be taken as a definitive position in 1843. He was physician to the York Dispensary, presented this paper to the Yorkshire branch of the Provincial Medical and Surgical Association at their annual meeting in York on 29 June 1843, and published in the British Medical Journal shortly thereafter. His position seems authoritative.
Downing CT. Neuralgia: Its various forms, pathology, and treatment. (Jacksonian Prize Essay, The Royal College of Surgeons for 1850). London: John Churchill. 1851. See Table 1.
Speaking to neuralgia Downing stated ‘the subject is rather of a speculative nature, involving the most secret workings of vis nervosa, and not capable of demonstration by either the scalpel or microscope of the pathologist.’ This is equally applicable to the clinical phenomenon of spinal irritation which was at best at this time was a diagnostic label applied to a narrative phenomenon existing largely by its description supported by rationalisation of few seemingly unconnected clinical symptoms. Downing said it this way: ‘all is thus left to observation and hypothesis.’
He considered the essential nature of neuralgia as being ‘A functional derangement - preternatural irritability of the nerve, leading to spasm of its fibres - The vis nervosa a motive force … Phenomena following compression of a nerve …’ (p. X) ideas echoed by Palmer. He identified cervico-occipital neuralgia as pains in the neck involving the posterior cervical plexus, and the sub-occipital and great occipital nerve. Perhaps his most notable observation is that it is difficult to clinically determine the source of nerve irritation, speaking to the idea of reflex loops between a disease in one part and pain or spasm in another.
These writings are around the time of those by Brown-Séquard and set the tone of discussion, leading to Gillies’ 1895 work on counter-irritation,18,19 around cause and effect within the nervous system. This became a core idea in Palmer’s assertions of relationships between disease and neural function where nerve energy could be too much or too little.
Paxton J. On spinal irritation. Glasgow Med J. 1861:283-7.
Paxton read his paper before the Glasgow Medical-Chirurgical Society in 1861 and gave several cases he classified as ‘spinal irritation’, remaking that ‘the disease is of considerable importance’ presenting as ’ most puzzling and apparently anomalous cases’.
His definition is relevant to us: ‘Pain is some part of the spinal column, generally accompanied by neuralgic or hysterical affections, unattended by fever or by other indications of inflammation, injury, or structural change of the vertebral column of its contents’. In this regard he seems to be pointing more towards fibromyalgia (see Weissman20) than subluxation.
Transition of the Idea to Chiropractic
We have established a strong presence in the medical literature for the idea of subluxation, expressed in terms of neurological change associated with functional derangement. We have seen how specific vertebrae could be identified by point tenderness with distal effects, and that Riadore (1842)21 considered the condition to be ‘spinal irritation’ due to subluxation. Given that Riadore learned under Harrison we can appreciate that these ideas had some currency in medicine of that time and that the idea of subluxation had cross the Atlantic to be a consideration in medicine as it developed in North-Eastern America. In 1835 Montrose Pallen22 wrote his thesis on ‘Spinal Irritation’. (Figure 2) His opening lines asserted:
‘Perhaps there is no department of medicine, in which to little has been done, and in which so much can be affected, as in the class of diseases which have been called nervous. All that we have been able to learn from former nosologists, is that they are dependent on some derangement of the nervous functions, and that their cure requires the administration of cordials, tonics, antispasmodics, “et umna id genus.”’
.png)
Pallen continued with reference to trigeminal neuralgia (Tic Douloureux) and the facial nerve and then spoke to the role of the ‘spinal axis’ and breast and intercostal pains. He noted that the examination of the spinal column revealed ‘generally much tenderness’ and situated spinal irritation in the ganglia and branches of the sympathetic nerves. The issue was, he stated, the ‘depravation of the organs deriving their nerves from this source.’ His discussion then explained what we known as the viscero-somatic reflex, and referred pain distribution, noting the specificity of viscera. We find his perspective to be almost predictive of the path Palmer was to take 60 years later, where Pallen described the symptoms of spinal irritation presenting as hysteria to be ‘phenomena which are dependent more or less directly, on nervous influence … reflect on other organs …’, even noting ‘obstinate constipation ~ the lumbar vertebrae were found tender.’
Correct the Cause
Of interest to us is that following a series of case reports in the genre of his times, Pallen concluded that 'remedies must be addressed to the primary source of irritation, sublata causâ (free the cause) … and that ‘… we should not overlook it because it clashes with our preconceived pathological opinions.’ So close to the thinking of Palmer yet so far in practical reality as he was unable to shift his thinking beyond medical orthodoxy of intervention that created a counter-irritation. The gift of Palmer was his pain-free correction of the cause, where such cause was subluxed vertebrae.
The Move Against ‘Spinal Irritation’
Our inquiry at this point examines the latter half of the 19th Century to determine how the medical idea followed one direction, creating a vacuum for Palmer’s ideas in 1895. During this last half of the 19th Century we see the ideas we have presented in this paper fade from the belief system of English medicine. We say ‘English’ medicine to recognize that London ascended over Paris and fostered the medical profession in the new colonies of North America and Australia. We accept ‘London medicine’ of the 19th Century to be ‘mainstream medical thinking’ in the context of Palmer’s developments.
It must be understood that nosology was in a primitive state of development in the 1850s. Robb-Smith’s paper of July 1969,23 a century after the debate, reports health discussions amongst leading members of the Royal College of Physicians London as they prepared the first listing of diseases and their diagnostic criteria. Eventually they produced a book of 360 pages distributed to general practitioners in May 1869. By 1896 the work was in its third edition.11 The effect of a reference-text was to standardize terms, however it took time to be adopted and applied. By its 7th edition in 1948 there was also the first edition of an ‘International Statistical Classification of Diseases, Injuries, and Causes of Death’,24 moving medical thought to a common nosology.
Prior to the initial publication of the Nomenclature of Disease (1869) and just a few years after Morris and his treatise on spinal irritation (above, 1843), Inman debunked the idea of spinal irritation as misunderstanding the reactions of muscle strain including about their tendinous insertions. The work is drawn from 2 essays, the first addressing ‘Muscular Affections’ (November 1856) and the second ‘Nature of Spinal Irritation’ (August 1857):
Inman T. ThePhenomena of Spinal Irritation and Other Functional Diseases of the Nervous System, Explained, and a Rational Plan of Treatment Deduced. London: John Churchill New Burlington Street. 1858.
Inman T. The Phenomena of Spinal Irritation and Other Functional Diseases of the Nervous System, Explained, and a Rational Plan of Treatment Deduced [Review]. Br Foreign Med Chir Rev 1858 Apr; 21(42):326-31.
In overview Inman states ‘at one period it was supposed that tenderness of any portion of the spinal column indicated incipient disease in the bones, in the cord, or its membranes;’ remarking that thirty years ago (the 1820s and 30s) such complaints were common. He suggested the emergence of a distinction between organic and functional diseases was a positive step towards understanding such clinical presentations, but lamented the emergence of the new theory of ‘spinal irritation.’ He considered hysteria as ‘the Medical Refuge for the Destitute’ and that ‘spinal tenderness’ was ‘nothing more than one of the forms assumed by that Proteus’ (p. ix).
His second part, from p. 99, discusses ‘spinal disorders’, ‘spinal irritation’, and ‘functional diseases of the spine’. He cites from Teale, and specifically writes on ‘what spinal tenderness is not’, saying ‘spinal tenderness has been, and still is considered the chief and characteristic symptom of functional disease of the spine.’ He provides a clinical diagnostic approach to rule out inflammation of the vertebrae themselves, along with congestion or other affection of the spinal cord. He achieves this by localising the tenderness to the spinous process of the vertebrae, with other logic based on the structural form of the spine. He rules out caries and conjoint inflammation of the canal and its contents. He notes the tenderness is superficial and not accompanied by redness, heat or swelling and the paradox that ‘we may have spinal tenderness without any marks of irritation, and symptoms of spinal irritation without spinal tenderness’.
His key point is the claim that ‘spinal tenderness itself is nothing more than the result of over-exertion of those very muscles, whose aches and pains we have already described in their more moveable insertions’ (p. 113). With regard to tenderness in the lumbar vertebrae he stated it related to the muscular exertion undertaken in a range of activities such as gardening and dancing. He stated:
‘We believe that the vast majority of the symptoms considered the result of spinal irritation arise from over-exertion of one or more portions of the muscular system in debilitated subjects’ (p. 123). He enunciated a law ‘The greater the debility of a patient, the greater is the irritability of his nervous and muscular systems’ (p. 144).
We next come to a paper read by the author, Hammond, before the New York County Medical Society on 17 January 1870. Hammond amassed expertise in the subject matter and in 1886 published a textbook ‘Spinal Irritation (posterior spinal anæmia)’.
Hammond WA. Spinal Irritation. New York: A. Appleton and Company 1870. Also published J Psychological Medicine 1870 (no volume, issue or pages given).
Hammond WA. Spinal Irritation (Posterior spinal anaemia). Copyrighted and published by George S. Davis, Detroit Michigan, 1886.
The history of his work is given as addressing the question of whether spinal irritation existed:
‘It has been question by several distinguished authors whether such an affection as spinal irritation really exists as a distinct disease.’ Referring to Inman he wrote he ‘… considers the pain produced by pressure over the spinous processes of the vertebræ as existing in the muscular attachments, and as indicative of what he calls myalgia.’ Hammond suggests it '… would be easy to ‘bring forward other authorities who have expressed similar views …’ and proceeded to give his own opinion. It was ‘there is a well-defined disease of the spinal cord, which if designated by its pathology, may properly be called spinal irritation.’
Hammond’s authority is found in him being ‘Professor of Diseases of the Mind and Nervous System and of Clinical Medicine in the Bellevue Hospital Medical College, and Physician-in-Chief to the New York State Hospital for Diseases of the Nervous System, ETC.’ He agreed with the directory’s symptomatology of spinal irritation as ‘its symptoms frequently resemble various and dissimilar maladies, and that commonly the function of every organ is impaired whose nerves originate near the seat of the disorder.’ He gave as a distinct feature that which we today consider referred pain, as ‘pain in distant parts’ and related these to the nerves arising from the spine and innervating those parts.
Hammond identified Dr C Brown of Glasgow (1820) ‘who, in a very excellent paper, gives a picture of the disorder which cannot fail to be recognized as truthful and exact by those who have witnessed several cases of the affection.’ He named Brown as being the first to use the term ‘spinal irritation’ (p. 5). Our interpretation of this finding is that Brown’s ‘spinal irritation’ was contemporaneously synonymous with Harrison’s ‘subluxation’.
Hammond continued to explain that when examining the spine in patients with affected parts then more or less ‘pain will be commonly felt by the patient on the application of pressure about or between those vertebræ from which such nerves emerge.’ This is a clear statement of relationship between pain in distant parts of the body, and distinct, identifiable levels of the spine. He refers to Dr Darwell of Birmingham who ‘described several features of the affection with accuracy, such as those simulating cardiac and gastric diseases,’ a clear statement of a link between spinal dysfunction and visceral disorders. (‘On some forms of cerebral and spinal irritation’, Midland Medical Reporter, May 1829).
On his retirement from Surgeon-General of the US Army, he published his second book (1886), firmly establishing tenderness over 1 or more vertebrae as pathognomonic of spinal irritation. He formed the view that ‘the essential condition of spinal irritation is anaemia of the cord.’ (1886 p. 43).
The Bonesetters
Bonesetters formed a concurrent stream of thought and practice which lent some methods to medicine, but not legitimacy. In England, medical doctor Wharton Hood published a series of four articles in The Lancet of 1871 (March and April), and his book later that same year (July). His articles related how his father came to attend a Mr Hutton, described as ‘the famous bone-setter’ and on refusal of Hood Senior to accept payment, invited him to observe his work as a bone-setter on his recovery. Hood Senior was unable to accept due to work pressure and his son Wharton took his stead. The articles described Hutton’s practice and then Hood’s application of his learning.
Hood W. On the so-called “Bone-setting”, its nature and results. Parts 1-4. The Lancet 1871: pp. 304-10, 336-8,372-4; 441-3.
Hood WP. On bone-setting (so called) and its relation to the treatment of joints crippled by injury, rheumatism, inflammations, &c. London: MacMillan and Co. 1871.
In our view Hood is a transition point between bone-setting and medicine. His articles are interpreted in conjunction with his textbook where subluxation is given as ‘some disturbance of the proper relations of a bone, without absolute displacement’. He does not specifically discuss ‘subluxation’ with reference to the spine, but does give detailed descriptions on how to ‘manipulate’ to correct the problem.
In essence Hood’s intervention specified a fast thrust, and he described hand and patient positions to achieve this. For low thoracic and lumbar segments the patient would be standing, fully flexed, and the holds taken as the patient is rapidly extended up and backwards. For the cervical spine the hold was under the chin in a seated patient. The treatment is not clearly described but infers a combination of traction and thrust. Upper thoracics were treated in a manner that would be familiar to many today, with the patient seated using the practitioner’s knee as a fulcrum.
Hood does not seem to have made a connection given between spinal dysfunction and bodily dysfunction such as diseases but he is particular in discussing the use of pain and tenderness as indicators, and using differential diagnostic approaches (‘scientific examination’) to rule-out ‘disease of the nervous centres, or of caries, abscess, or other destructive change in the vertebral column.’
Jewell JS. Spinal Irritation. The Journal of Nervous and Mental Disease. 1881 pp 760-72.
Jewell wrote this paper with the stated intent to ‘to give the results of a rather prolonged experience with and study of this disorder.’ The strength of his argument is the ruling out of diseases to leave only a spinal lesion that could be safely treated by a range of therapies.
These included the use of opium, and of electricity, two methods that again point to the merit of Palmer’s strong stance of ‘without drugs or surgery.’
A more recent (2008) paper20 outside the scope of our paper, deserves to be mentioned at this point as it links ‘Spinal Irritation’ with ‘Fibromyalgia.’ To us, this seems a logical destination which separates ‘spinal irritation’ as ‘fibromyalgia’, from ‘subluxation’.
Ross J. On the segmental distribution of sensory disorders. Brain. 1888 January;104:333-61.
The relevance of this paper lies in it being a ‘sate-of-the-art’ description of neuroanatomical knowledge at the beginning of Palmer’s decade of active development (the 1890s). The work is factual and there is no speculation regarding the idea of ‘spinal irritation’, however ‘nerve irritation’ is discussed in three places:
‘this pain did not extend up the occiput, it was situated in the surface area supplied by the posterior branches of the fourth and fifth cervical nerves, and it is the lateral and anterior branches of these same nerves which supply the skin over the outer part of the clavicles and shoulders, and consequently both pains are likely to have been caused by irritation of the phrenic nerve … the action of the heart becomes tumultuous and irregular … the abdominal aorta is seen and felt to pulsate strongly . The bowels also rumble a good deal, and he seems to find some relief in belching, and still greater when wind passes per anum; these last symptoms being probably due to associated irritation of the pneumogastric nerves’ (p. 355);
‘We thus see that the region of the spinal cord which gives origin to the brachial plexus gives origin also to the greater part of the fibres which eventually find their way to the heart. Wherever, then, the original commotion may have taken place in an attack of angina pectoris, whether in the cardiac ganglia of the sympathetic, or in the spinal cord, and whether the commotion be due to some peripheral irritation from disease of the heart’s substance, or be a spontaneous outburst on the part of the nerve cells implicated, it is evident that it is only when the commotion has begun in the cord, or has passed up to the grey matter of the spinal cord from the sympathetic …’ (p. 356); and
‘the patient complains of a pain shooting across the spine and shoulder-blades on a level with the third or fourth dorsal vertebra. There is no reason to believe that the posterior branches of the third or fourth dorsal nerves are subjected to direct pressure or irritation, and therefore the pain must be an associated one, caused by irritation of the sympathetic roots of these nerves, which are known to supply splanchnic fibres to the large blood-vessels. Anginal attacks, and, indeed, all diseases attended by great anæmia of the brain, are accompanied by a feeling of weight and oppression of the top of the head, but of the causation of this pain I cannot give a satisfactory account’ (p. 358).
The Arrival of Chiropractic
The paper by Ross (above) can be accepted as closing the medical discussion on spinal irritation and in its place firmly establishing the concept of nerve irritation, one that was central to Palmer’s working hypotheses.
We can not over-emphasise the importance of Palmer’s ‘without drugs, without surgery’ mantra as the prevailing treatment of that time carried the intent to produce pain as a counterirritation to the clinical presentation, whatever it was called, and believed to stem from the spine as evidenced by tenderness over vertebrae. Gillies produced these 2 definitive works on the matter:
Gillies H. The theory and practice of counter-irritation. London: Macmillan 1895.
Gillies H. The theory and practice of counter-irritation [Review]. American J Medical Science 1896-04: 453-4.
Gillies provides a comprehensive review of the 19th Century literature on spinal irritation. It is a British publication and its review in America soon after its publication demonstrates how rapidly medical knowledge crossed the Atlantic. Gillies does not address spinal irritation in any meaningful sense but does make reference to Brown-Séquard’s 1858 presentation on spinal reflexes to the Royal College of Surgeons (p. 37) Gillies draws from Brown-Séquard’s work the principle:
‘when we wish to produce a modification in the conditions of any organ, we must apply the means of irritation that we prefer to the parts of the skin or mucous membrane which have the most evident nervous relation to it.’
He recognized segmental relationships of the ‘cerebro-spinal axis’. He cites Sturge of 1883 who concluded ‘the sensory centres for the skin over any particular organ or part are associated more or less closely with those controlling the sensory functions of the subjacent organ or part …’ if we wish, for example, to act on the kidney, the skin of the abdomen in its upper part is the best for the application of any kind of irritation.’ Gillies wrote:
‘That the principle of nervous reflex action is a factor in the mechanism of irritation is almost certain, but that it is the principal factor has not yet been proved’ (pp. 38,9).
He cited the 1877 report of Ross regarding ‘a close connection between internal organs and definite areas of skin surface through the rami communicantes - the sensory sympathetic fibres to such organs coming off from the same part of the spinal cord as the somatic nerves to such areas of skin.’
The value of this work is that it demonstrates emerging knowledge and application of neurological processes associated with health and well-being, and presents the best argument in favour of counter-irritation. Gillies states:
‘that by Counter-Irritation we seek to establish an increased action in in one tissue or organ for the purpose of diminishing an increased action which is taking place in another tissue or organ, the performance of whose functions is of great importance to the organism.’
It must be remembered that the application of counter-irritation could not be considered a painless procedure, indeed it is stated ‘An irritation is always more or less an injury’ (p.119). Gillies presents a detailed description of the process of creating irritation, starting with cautery:
‘the most violent, and it is believed, in certain cases the most effective of all counter-irritants remedies’ which included about the vertebræ, was performed with ‘a piece of red-hot iron’ (p. 194).
A milder form of heat had passed out of style, this may have been the 1827 description of ‘firing’:
… applying of a metallic instrument, heated to a temperature of 212 degrees by immersing the head of it in boiling water for five minutes … covering the part with a piece of silk moistened in warm water …’ then applying gently for three or four seconds.’
It is interesting that Gillies readily acknowledged the importance of the patient’s mind in the healing process (p. 57), stating:
‘the physician who does not recognise this, or knowingly disregards it, is placed at great disadvantage.’
An understanding of these views is essential to understanding Palmer’s closely-following arguments in relation to the role of the nervous system in what he first called ‘dis-ease’, and his premise that the correction of subluxed vertebrae removed the cause.
It could be said that this is the same concept of counter-irritation which is stated to affect the cause through neural mechanisms. This is summarised in Gillies’ view that:
‘… the irritation of the cutaneous nerves will modify in a simple reflex way through the centres in the brain and cord, the circulation and nutrition generally of the parts beneath; the impression which passes along, in being immediately reflected along the vascular or trophic nerves.’
With today’s knowledge such mechanisms could have been as simple as the pain-gate mechanism and reflex neural actions. Gillies referenced Davidson of Liverpool ‘that disease can be modified by influences acting through the nervous system, is quite consistent with our knowledge of the dependence of the health processes of circulation and nutrition on the nerves. As to the therapeutic evidence of the value of counter-irritation the evidence is as strong as it can be’ (p. 64) concluding ‘where blisters do any good it is because of their genuine inflammatory action’ (p. 65).
Conclusion
We have presented this combined report of our individual searches exploring a history of the idea of subluxation. In particular our findings show that the idea of small spinal dysfunctions, amendable to intervention, emerged in Western medical writings from the 14th Century and by the 19th Century and Harrison they were termed subluxation. Quite a number of medical practitioners explored the idea and by the 1850s had introduced the term ‘spinal irritation’. We acknowledge the much earlier appearances of the idea in Egyptian and Greek medical writings.
The authors and their works which we have considered are gathered chronologically in Table 2.
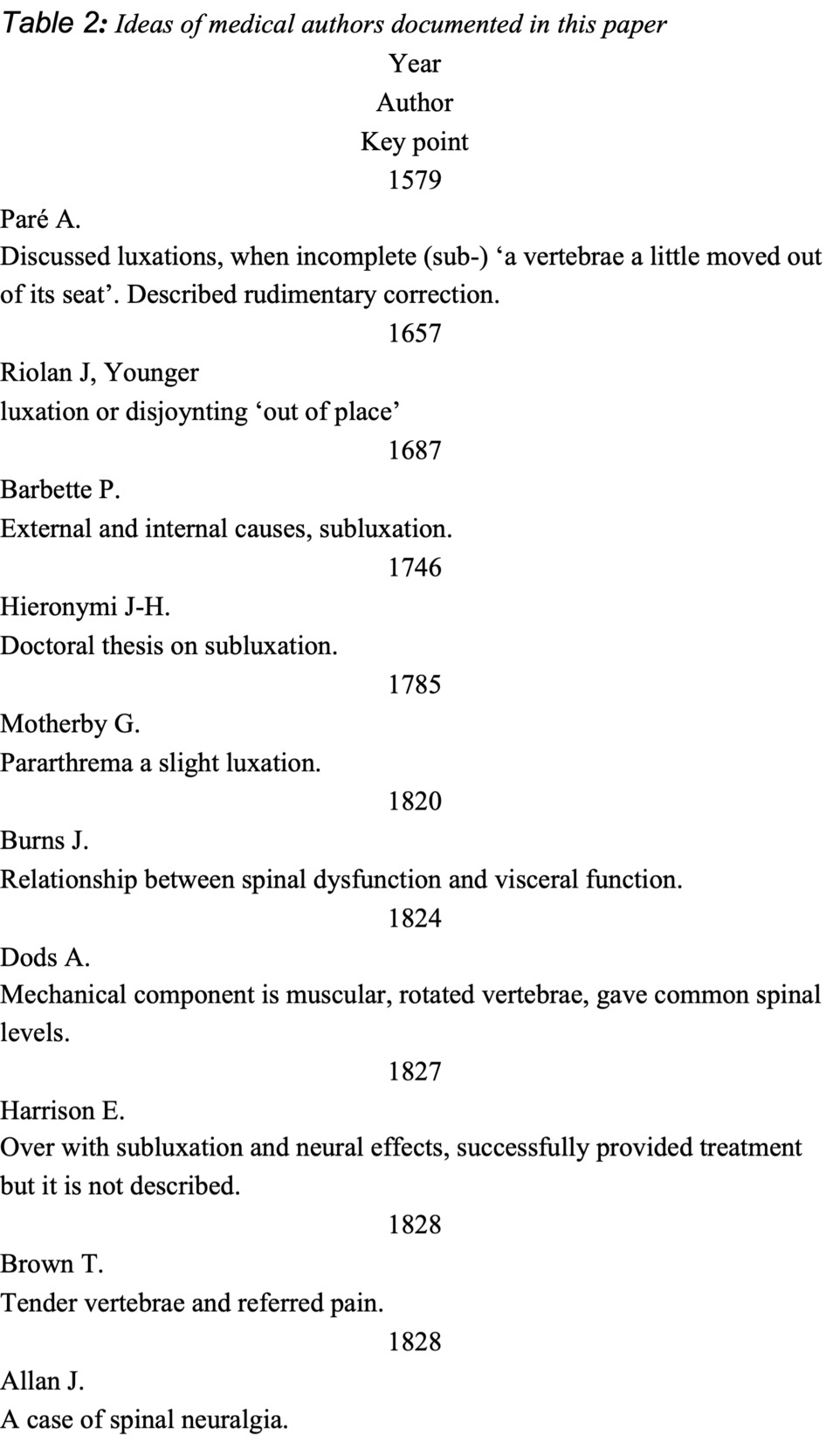
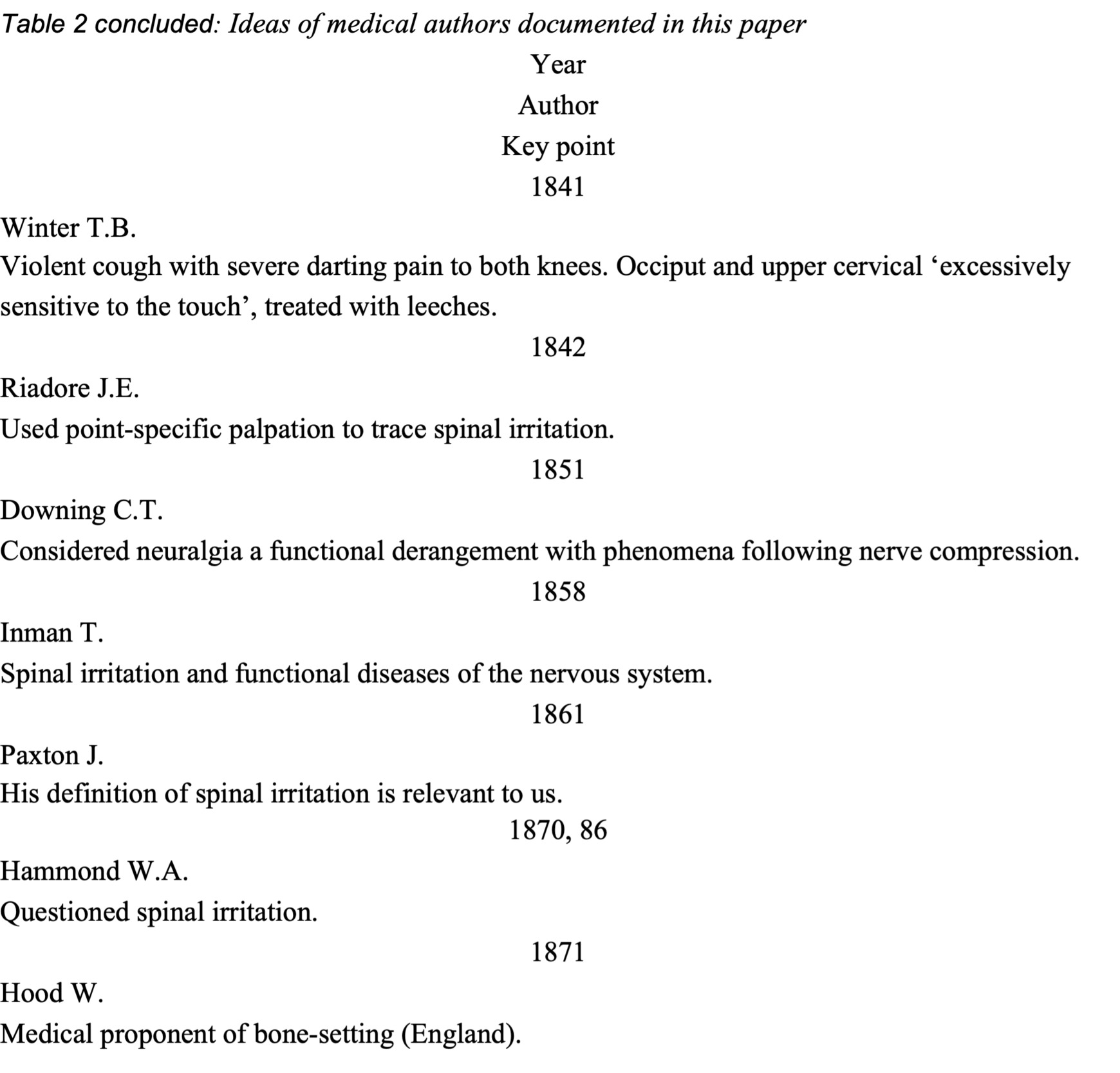
The emergence of nosology placed emphasis on clarifying the medical lexicon and by the time of Palmer the term ‘spinal irritation’ was out of favour however the clinical conditions persisted, so much so that we have Gillies’ detailed discussion of methods to create pain about the spine as a counter-irritation. Palmer’s pain-free method also proved to be remarkably effective according to the many reports he published.25
Oakley Smith, a 1900 graduate of Palmer’s, used the term ‘sub-luxation’ in an advertisement 4 February 190226 and shortly after DD himself used that form of the term, the term ‘sub-luxation’, in a letter to B. Palmer26(p103) Eventually the term lost the hyphen, to become ‘subluxation’, with the meaning of DD Palmer being to describe a subluxed vertebra in relation to its fellow. The idea of subluxation as a small spinal dysfunctions amendable to intervention has become emblematic of chiropractic, and the journey of the term throughout the profession’s history is another matter and one we feel worthy of thoughtful investigation.
We conclude with the observation of Palmer, speaking of himself:
‘D. D. Palmer said, in print and person … it was he who first described how and why luxations were the cause of disease. He has created a science of vertebral adjustment. True, there were others, perhaps thousands, who had replaced joints of the backbone, but none had knowingly used the spinous and transverse processes as handles.’27
We understand him to be reinstating the role of small spinal dysfunctions, amendable to intervention that he considered to be subluxed vertebrae, a role abrogated within mainstream medicine.
Authors’ Note
We reproduce the spelling and sentence structure as found in the documents examined.