
Introduction
It has been shown that leg length inequality (LLI) is associated with pelvic misalignment (torsion and tilting) and low back pain.1–3 Interventions aimed at correcting leg length frequently consider these apparent relationships. Clinically, LLI is commonly represented as the difference in height of the femur head levels (FHL) visible on a standing pelvic radiograph, although other methods such as full-length radiographic examination of the lower extremities are the gold standard.4
Within chiropractic, Gonstead proposed a 5:2 ratio between pelvic misalignment and relative FHL on an A-P full-spine radiograph.5 According to this concept, every 5 mm of innominate misalignment, whether from +/-Θx (torsional) or +/-Θy (rotational) changes at the sacroiliac joint, should produce a corresponding 2 mm change in relative FHLs. Forward torsion (+Θx), seen as a shorter innominate length on the A-P film, is expected to create an ipsilateral functional lengthening of the leg, reflected by a higher femur head; the opposite applies to posterior torsion. Similarly, +Θy rotation, identified by lateral offset of the pubic symphysis relative to the S2 tubercle, is theorized to produce an ipsilateral 2 mm lowering of the femur head, with the reverse pattern for -Θy rotation. This proposed proportional relationship between innominate alignment and FHL has traditionally guided heel/shoe-lift recommendations in the Gonstead approach to LLI.
In 2022, a survey of international chiropractic educational institutions reported responses from 29 of 47 programs queried. Gonstead technique was identified as a mandatory entry-to-practice component in 15 of the 29 institutions and as an elective course in an additional four programs, indicating that 65.5% of responding institutions included Gonstead instruction within their curricula.6 In addition, a 2003 review by Cooperstein reported that 58.5% of practicing chiropractors used Gonstead technique methods.7 Continuing education programs focused on Gonstead technique also remain widely presented. These findings indicate that Gonstead technique has been both widely taught and commonly used within the chiropractic profession for decades. Therefore, the present investigation is clinically relevant given the wide-spread influence of the Gonstead technique in the chiropractic profession.
The purpose of this retrospective study was to formally test the Gonstead theory on the relationships of pelvic measurements and observed FHL differences comparatively in pre- and post-treatment radiographs. Comparing measurements from pre- and post-treatment A-P pelvis radiographs under chiropractic care in cases with FHL changes can help clarify relationships among these measurement parameters.
Gonstead reportedly formulated the 5:2 rule using radiographic measurements of images from a skeletal spine/pelvis model, according to personal communication.8 He is said to have created pelvic misalignments on the model, obtained radiographs, and measured both the innominate changes and the corresponding FHL differences. These comparisons between pre- and post-manipulated model images reportedly showed a 2 mm change in relative FHL for every 5 mm of innominate misalignment. Notably, the model apparently did not include lower extremity contact with the ground, unlike human subjects who are radiographed while weightbearing. This absence of weight bearing load in the experimental setup is incongruent with Gonstead’s own Level Foundation Theory,9 which asserts that unleveling of the base of support destabilizes spinal structures above.
Applying the findings from that model experiment to real patients is questionable. Such a development should also be viewed in context: the experiment reportedly took place over 60 years ago. The model became the basis for recommending heel lifts when certain radiographic findings were present, such as a lumbar curve with its convexity or body rotation on the side of the short leg. Lifts were generally not used when the LLI measured 6 mm or less and were considered more strongly when a patient was unable to stabilize with care alone.5
LLI is common in the general population and has been linked with spinal and lower-extremity conditions, including scoliosis, lower back pain, and degenerative joint disease.10 A recent systematic review reported that full-length standing radiographs remain the most valid and reliable method (global reference standard) for determining anatomical LLI when compared to clinical assessments such as block testing or palpation.4 LLI under 10 mm are common and usually asymptomatic, with the body often compensating through natural lower-extremity adaptations.11 Because palpation or block-based assessment methods alone may lack precision, radiographic evaluation is particularly useful when clinical findings are equivocal or when small asymmetries might have clinical significance.4
Evidence to guide decisions about when to treat LLI is lacking. Apparently, there are no studies that have compared the natural course of LLI with treatment or evaluated how different treatment approaches compare with one another.10
Knutson et. al.12 found a 90% prevalence of anatomical LLI in a collection of 573 subjects, including groups of patients from several studies with low back pain, runners, random subjects, and volunteers, with a mean value of 5.2 mm, using data on LLI obtained from what they termed accurate and reliable x-ray methods, which were reportedly preferred over non-radiographic clinical methods due to the reliability of radiography in comparison. Knutson et. al. also discussed a study of imposed LLI via applications of foot lifts showing a linear relationship in pelvic torsion as the leg was lengthened from 1/4" to 7/8". They cite references that report other effects of LLI and pelvic torsion, such as lumbosacral facet joint angle asymmetry, scoliosis, and vertebral body shape distortions.
Cummings et. al.13 showed that imposed leg length differences produce pelvic torsion, with anterior rotation (+Θx) of the innominate on the short-leg side and posterior rotation (-Θx) on the long-leg side. This supports the concept that anatomic LLI induces sagittal plane innominate rotations as a primary compensatory mechanism. This pattern is consistent with Gonstead’s observations of +Θx/AS innominate misalignment, in effect lengthening the ipsilateral leg, in compensation for an imposed shorter leg and +Θx/PI innominate misalignment compensation for an imposed longer leg.
The best clinical, non-imaging-based measurement method for LLI is likely the standing block method.4,12,14 The standing block method captures both the anatomical and functional aspects of LLI, has high inter-examiner reliability and correlates well with radiography for LLI greater than 5-6 mm. The block test plus one confirmatory AP pelvic film is also a recommendable approach in clinical settings.4
Considerations with LLI Measurement Methods
Small leg -ength differences on standing pelvic X-rays (around 5 mm or less) may not be true bone-length differences. Studies show that simply tilting the pelvis or changing hip position can create a few millimeters of apparent leg-length inequality on an X-ray even when the legs are the same length.15 Reviews and clinical studies state that functional factors such as soft-tissue imbalance, hip contractures, spinal curves, and postural compensation can contribute to apparent leg-length asymmetry, even in the absence of true anatomical differences.9,16,17 Therefore, when the femur head height is unequal up to 5 mm, it may often be a functional or postural effect, not an actual difference in bone length.
Without a standing spine/pelvis radiograph, contraindications to heel/shoe-lift use such as a contralateral convexity of a lumbar curvature or lumbar vertebral body rotation opposite the lower femur head, or a spine that is already well-balanced may go unnoticed. Several scoliosis and LLI studies emphasize that these biomechanical patterns are best evaluated on standing radiographs, and that applying a lift in the wrong biomechanical context can potentially worsen a curve rather than improve alignment.18–21 However, other published literature bases lift prescription primarily on clinical LLI assessment and symptoms, without requiring a standing spinal radiograph, and still reports clinical improvement.22,23
Overall, some evidence suggests that detailed radiographic evaluation is more critical in some cases, whereas general LLI management sometimes proceeds effectively without standing spinal imaging. Those non-radiographic clinical methods may be useful for screening but have been shown to have error rates of about 5 to 8 mm of leg length inequality when compared to pelvis radiographic measurements.24,25
The direction of pelvic torsion may vary depending on whether the LLI is of anatomical or functional origin.26 But common pelvic landmark tests, such as PSIS level checks, can be unreliable and some pelvis alignment changes may not be accurately measured without imaging.27 Radiographs, in contrast, are frequently used as the reference method for measuring pelvic tilt and rotation and are used in comparison to surface-based evaluations.28,29 Surface based assessments, however, are reasonably reliable for clinical assessments in certain situations.28 There are various methods available to measure LLI, the reliability and accuracy of some of which have been previously investigated.30
Radiographic measurements of LLI were shown to be reliable as early as Friberg’s work in 1980.31 Plaugher found the Gonstead pelvic measurements used in this study to be both reliable and stable over time.32,33
Gonstead proposed that sacro-iliac joint (SIJ) injury and other biomechanical changes could create secondary pelvic torsion-misalignment, which would alter the femur head heights seen on standing radiographs.34 His 5:2 rule was intended to help clinicians tell whether they were looking at true anatomic LLI or functional LLI from biomechanical changes. He used misalignment listings such as PI (posterior-inferior), AS (anterior-superior), EX (external), and IN (internal). The listings were descriptive of the relative position of the innominate bone to the sacrum when it is misaligned, with the alteration in alignment occurring within the SIJ.34
Comparative FHL may not be the same as the LLI, which is important to differentiate.35 FHL is measured by comparing the height of the femur heads and is the result of the bilateral lower extremity lengths, as well as pelvis and lower spine biomechanical effects on femur head balance. LLI is solely the anatomical inequality of lengths of the lower extremities.
An A-P full spine radiograph is used in the practice of chiropractic when multiple regions of the spine need to be viewed, in medical practice for spinal assessment of scoliosis and to measure outcomes for surgical procedures for the spine. The A-P full spine film is not the gold standard for LLI assessment. The femur head level radiograph is less prone to image distortion than the A-P full spine view,36 whereas full length, bilateral lower extremity radiography provides a more direct leg length measurement.37 LLI is often assessed as a part of scoliosis38 and is usually visible on A-P full spine scoliosis radiographs. Dependable measurements from the A-P full spine radiograph would enhance the practical application of corrective lifts for chiropractors when full spine radiographs are indicated.
The image and measurement of FHL on A-P full spine radiographs to determine indications for leg-length management may be affected by distortions in pelvic or other skeletal alignment factors due to the angle of projection,39 especially in comparison to a direct view of the femur heads with more specific, femur head level radiographs. The measured difference in FHL on A-P full spine radiograph may be due to image distortion from positioning the patient with the pelvis rotated or translated to one side.40 It is also possible that a femur head view radiograph may not always represent the actual anatomical difference in leg length, since it is possible that functional disturbances in pelvis alignment or lower limb dysfunction may be a confounding variable in measurement of LLI.41,42
The Gonstead theory of pelvic misalignment and functional LLI also suggests that rotation (IN or EX pelvis listings) may cause functional LLI. But there is essentially no published research showing an association of +/-Θy rotation misalignment of the innominate bones with LLI. There is reportedly about 1.5 degrees of axial rotation (around the y axis) at the SIJ.43 Furthermore, there is no logical reason for rotation around the Y axis of the innominate bones to cause LLI. Whereas pelvic height asymmetry or obliquity from pelvis torsion as described by the AS/PI misalignment in the Gonstead methodology, which could include a difference in hemipelvis or acetabular height, is plausibly related to functional LLI.
The causes of FHL imbalances exhibited on radiographs are not fully understood. There are functional adaptations to LLI that cause pelvic torsion and FHL imbalances and there are anatomical variations in leg length that include relative bone length inequalities, degenerative changes in the lower extremity joints, functional and anatomical conditions resulting in relative asymmetries of the feet and other possible causes. This study sought to investigate a small portion of those phenomena.
Sacro-Iliac Joints
A widely cited review reported that most in vivo studies describe normal SIJ motions as ranging from less than 1° to approximately 4° of torsional movement, with substantial variability attributable to individual SIJ anatomy.44 Some studies have reported torsional values as high as 6° or even 9° (likely outliers).44 Translational motion at the SIJ has been reported to range from approximately 2 to 5 mm, with observed motion dependent on factors such as sex, subject positioning, and the method used to induce movement.44 In contrast, during typical daily activities such as walking, SIJ motion is generally minimal, often measuring less than 1 mm.45
Ranges of SIJ motion can increase with injury but are still relatively small. There is little evidence of in vivo measurements of such effects. In a foundational study cited over 200 times in the literature using cadavers, they showed up to 4 to 5 times the normal movement after destabilizing the ligaments (still only a few degrees increase),46 but these types of studies do not likely resemble the effects of in-vivo injuries.
METHODS
Hypotheses
Null Hypothesis: The linear relationship between innominate bone asymmetry and femoral head height difference conforms to the Gonstead 5:2 rule; specifically, the true regression slope between the two variables equals 0.4.
Alternative Hypothesis: The linear relationship between innominate bone asymmetry and femoral head height difference does not conform to the Gonstead 5:2 rule; specifically, the true regression slope differs from 0.4.
Study Design
Retrospective Study: This study is a retrospective review of radiographs obtained during the routine course of care for adult patients treated in the practice of a chiropractor certified as a Diplomate in the Gonstead Technique by the Gonstead Clinical Studies Society.
Beginning at a predetermined date and reviewing patient files in reverse chronological order, we identified consecutive patients who had undergone initial full-spine radiographs followed by a subsequent set of full spine radiographs after receiving chiropractic care, and who met all inclusion criteria. The chiropractor serving as custodian of the records started with the most recently acquired radiograph and, using the clinical records, identified the corresponding prior radiograph date retroactively.
This investigation involved a review of existing medical records only. Radiographic measurements and other relevant patient data were extracted from previously acquired records. No control group was included, as the retrospective study design focused on comparing pre- and post-treatment radiographic measurements within the same patients.
Subjects
Inclusion criteria: Patients were included if they were 21 years of age or older, had diagnostic-quality AP and lateral full spine radiographs, and had undergone a subsequent set of full spine radiographs following a course of Gonstead chiropractic care. In addition, we systematically excluded cases in which the radiographic measurements demonstrated less than a 2 mm difference in FHL between the initial and follow-up examinations. This criterion was selected to increase confidence that observed differences were not attributable to measurement error, as described by Plaugher and Hendricks.32 Their findings also indicated that using a single examiner substantially reduced examiner variability compared with the variability observed between two examiners performing the same Gonstead pelvic measurements. Accordingly, they recommended that future research of this method employ a single examiner to enhance measurement reliability as we did in this study.
Exclusion criteria: Patients were excluded if they were younger than 21 years of age, lacked clinical records meeting the inclusion criteria described above, or had hip, knee, spinal, pelvic, or lower-extremity prostheses, or heel/shoe lifts. Patients were also excluded if they had surgical implants, such as pins, screws, rods, or similar devices, within the spine, pelvis, or lower extremities.
Number of subjects in the study: We collected data on 29 subjects that met the above criteria.
Institutional Review Board
We received Institutional Review Board approval from Life Chiropractic College West - Project: PN 2012-018.
Data Extraction
Data extracted from the radiographs included the measurements of the length and width of the ilium bones, relative alignment of the pubic symphysis to the S2 tubercle on the y-axis, relative heights of the femur heads in relation to ground level, the amount of time between radiographic data sets, the patient’s gender and age, and the number of chiropractic visits between the data sets. The use of orthotics or heel lifts, pregnancy, surgery, a history of significant trauma or illness pre-treatment and/or between data sets or other events that may affect pelvic mechanics or limb length, was also recorded.
An associate chiropractor at the facility where the radiographs were obtained performed all radiographic measurements and had been formally trained in the measurement procedures. These methods have been previously evaluated for reliability and stability as reported in prior studies.32,33
X-ray Equipment Alignment and Positioning Protocol
Pelvic and leg length measurements obtained from radiographic examinations require careful attention to patient positioning and proper alignment of the X-ray equipment. It is not the purpose of this paper to provide a detailed discussion of equipment alignment or patient positioning protocol; a comprehensive description of the Gonstead procedure for full spine radiographic examinations is available elsewhere.47
Key aspects of X-ray equipment alignment include ensuring that (a) the central ray is perpendicular to the grid cabinet or bucky, and (b) the grid cabinet is level. However, because the same X-ray equipment was used for both the pre- and post-treatment radiographic examinations in this study, any imbalance in magnification is mathematically unlikely to be significant enough to affect the results.
Radiographic Analysis
Relative FHLs represent the measured LLI. Differences in the apparent length of the left versus right innominate bones indicate relative pelvic alignment and may reflect unequal tilting resulting from differing degrees of +/-Θx torsion on one side compared with the other. Such asymmetrical Θx innominate torsion can cause the femur head heights to appear different on the radiograph, thereby producing a measurable LLI. Gonstead theorized that such x-axis rotation, as well as y-axis pelvis rotation, could both create LLI.5
The degree of deviation between the center of the pubic symphysis, which represents the anterior pelvic center, and the center of the S2 spinous process, which represents the posterior pelvic center, is measured to assess any y-axis rotational displacement. The relationships between the magnitude of LLI and the degree of pubic symphysis-to-S2 deviation, the magnitude of LLI and the relative ilium length measurements, and whether these relationships demonstrate predictable ratios, are the primary focus of this study. An example of the measurements on the radiograph is shown in Figure 1.

Figure 1. AI generated depiction of an A-P radiographic view of the lumbo-pelvic region, showing the Gonstead technique measurements: alignment of the innominates by relative lengths of each (A); leg length inequality by relative femur head heights (B); pelvic rotation as measured by relative positions of the S2 tubercle to the pubic symphysis on the y-axis (C).
Collecting the Data
1. The investigating chiropractor reviewed every patient listed in the clinic’s X-ray logbook and then retrospectively searched each patient’s record in chronological order.
2. The investigator would then determine whether the radiographs she initially found were from a follow-up X-ray examination, meaning that set of radiographs were the patient’s second series in the office.
3. If the above inclusion criteria were met, the investigator retrieved the radiographs from the initial and follow-up examinations from their records.
4. The investigator would erase any previous markings and measurements that may have existed on the radiographs. She would then reassess the radiographs with the indicated measurements for leg length inequality by comparing femur head heights bilaterally on these standing full-spine radiographs.
5. If the radiographs of that subject showed a minimum of 2 mm or more measured difference in leg length and the radiographic image included the full pelvis on the film and the subject was at least 21 years old, then those radiographic records were considered for inclusion in this study.
6. The investigator would then record the date of the radiograph, and the age and gender of the subject.
7. The case number was then assigned to the Data Extraction Form in place of the subject’s real name, and that number was also kept on a master list of real names that were not shared with anyone outside of the treatment facility.
8. The investigator would then perform all the markings and measurements on the A-P film that was required for the Data Extraction Form. The Gonstead Spinograph Parallel radiographic measurement tool was used for all marking procedures and measurements. Good inter and intra-examiner reliability, and stability over time, of these pelvis and leg-length inequality measurements using this marking/measurement tool and these Gonstead measurement procedures were previously established by Plaugher, et al.32,33
9. She then transferred the radiographic measurements onto the Data Extraction Form.
10. She then checked the subject’s records to determine if orthotics and/or a foot lift was applied for that subject and, if so, recorded that information on Data Extraction Form.
11. The investigator would then count how many chiropractic adjustment visits the subject received at that clinic between the initial and follow-up x-ray examinations and record that information onto the Data Extraction Form.
12. The Data Extraction Forms were then scanned and sent by email to the Principle Investigator. Real names of subjects were not included in these shared Data Extraction Forms, and case numbers were substituted for real names of subjects. All cases were saved with the master list of real subjects’ names and stored in the clinical facility where the treatment was rendered.
Preparing the Data for Analysis
The primary variables in data calculations were the change in combined right-side innominate alignment and the change in right femoral head height. The net change of the innominate misalignment (PI, AS, EX, IN) measured on the pre- versus post- treatment radiographs was figured in relation to the right innominate bone. This right innominate misalignment was listed as a positive value if the net combined change was greater for either/both PI or EX (since both are predicted to lower the ipsilateral femur head relative to the left), and a negative value if the net change in misalignment was greater for either/both the AS or IN (since both are predicted to raise the ipsilateral femur head relative to the left). The relative femur head height was listed as a positive value if the net change was a lower femur head on the right compared to the left and was listed as a negative value if the right femur head was higher compared to the left on the follow-up versus the initial radiograph. In this way, the calculations were configured in a kind of common denominator method such that the net effect was able to be analyzed between the net change in right innominate to the net change in right femur head height.
Results
Statistical analysis
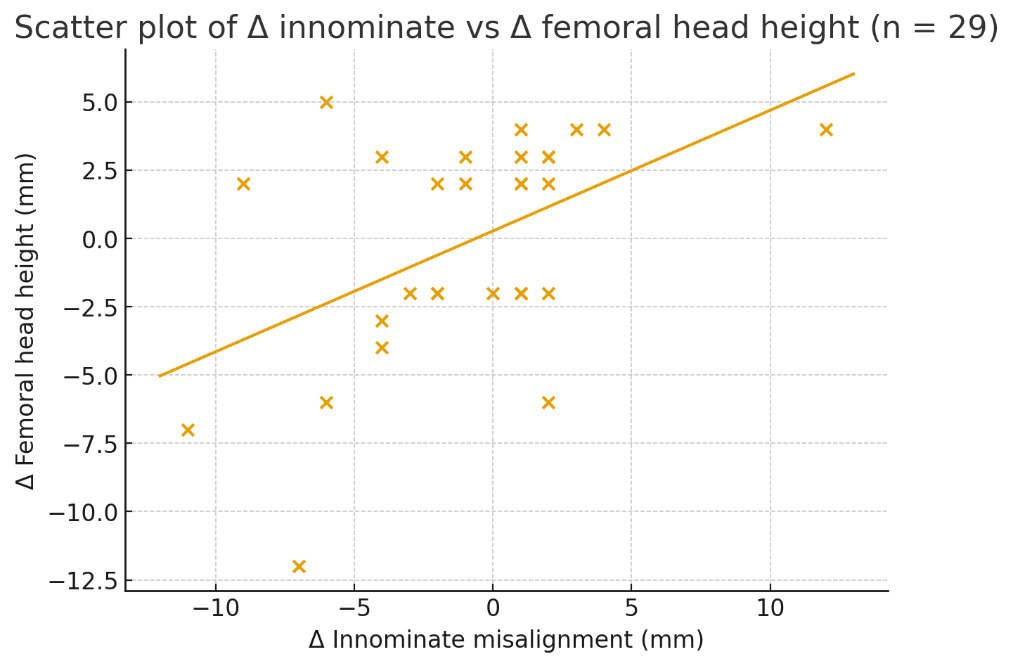
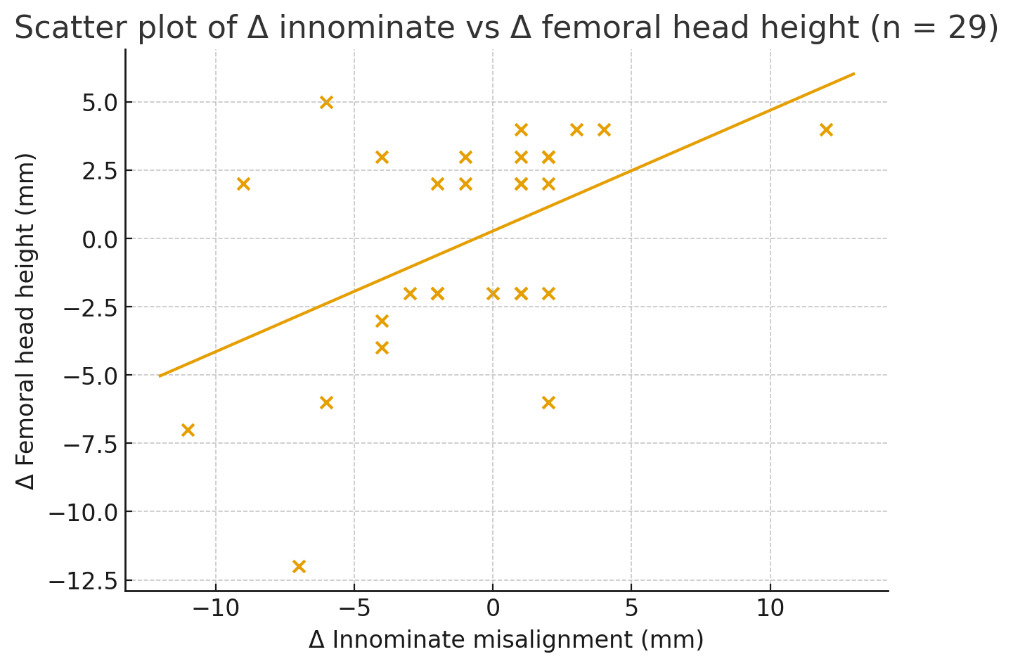
All analyses were run using simple linear regression, treating the change in femoral head height (Δ femur) as the outcome and the change in innominate alignment (Δ innominate) as the predictor. For the full sample of 29 subjects, we calculated the regression slope (β̂), intercept (α̂), standard error (SE), the R² statistic to show how well the model fit the data, and the p-value for testing whether the slope differed from 0.
To determine how stable the findings were, and whether the relationship might be different at higher or lower levels of misalignment, we ran additional assessments:
-
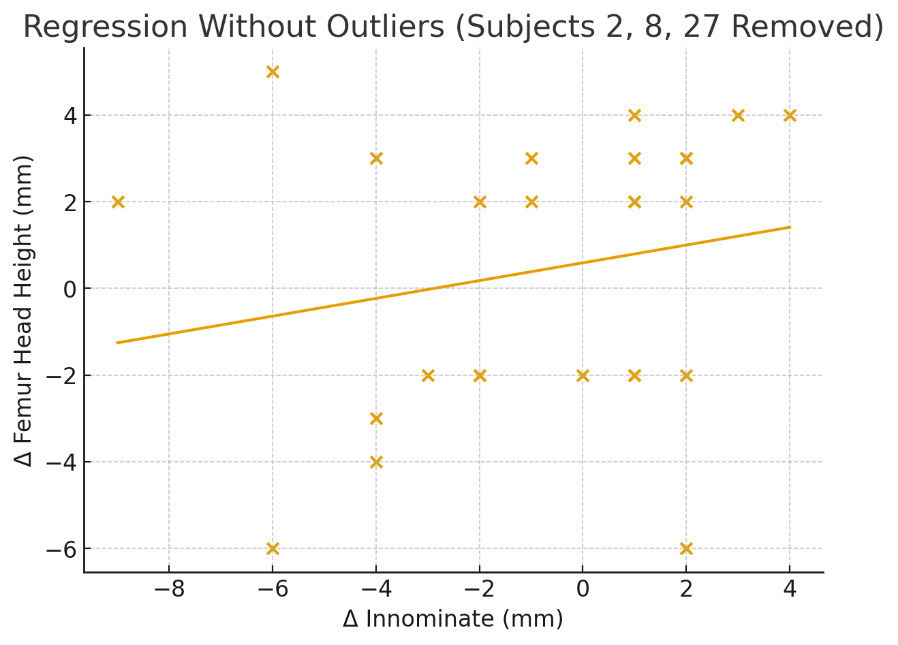
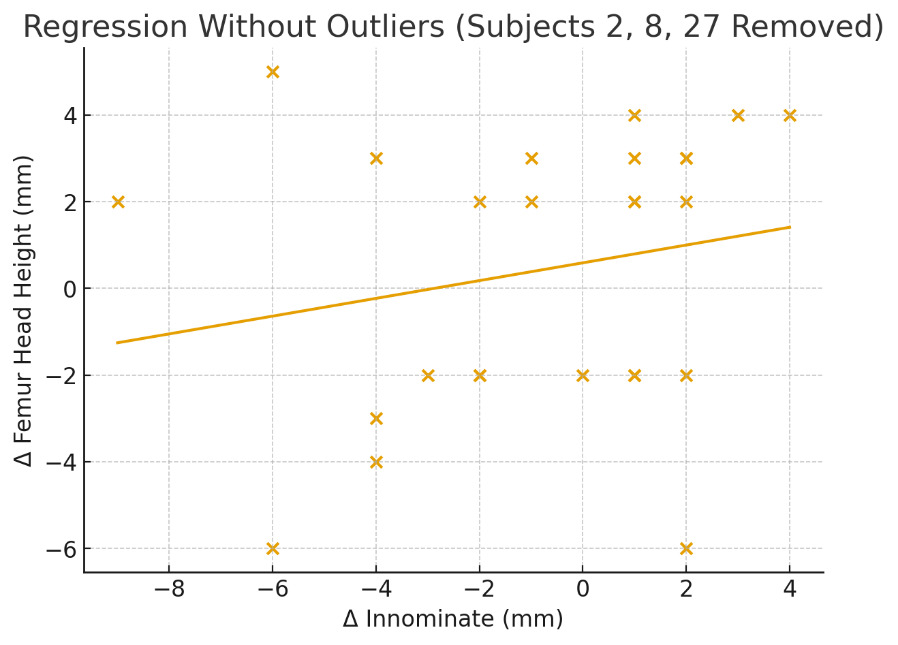
Outlier screening: Potential outliers were initially identified by z-score screening on both Δ innominate and Δ femur (|z| > 2). This screening identified 3 subjects for potential omission. Further review indicated that changes of 11–12 mm in innominate measurements or a 12-mm shift in femur head-height differences between pre- and post-treatment radiographs were unlikely to be biologically plausible. Therefore, three cases (subjects 2, 8, and 27) were excluded in a sensitivity analysis.
-
Split-sample regressions: We ran separate regressions for subjects with positive Δ innominate (increased right-sided innominate alignment; n = 14) and negative Δ innominate (increased left-sided relative alignment; n = 14). This allowed us to determine whether the relationship differed depending on the direction of pelvic change.
A 2-sided α of 0.05 was used. Given the small sample, we are treating the subgroup and outlier-removed results as descriptive rather than definitive.
A total of 29 subjects met the inclusion criteria. The primary analysis examined the linear relationship between changes in innominate misalignment and changes in femoral head level differences on A-P radiographs. The regression produced a slope of 0.442 (95% CI: 0.12 to 0.76) with an intercept of 0.274. Although this numerical estimate lies near the 0.40 ratio proposed by the Gonstead 5:2 rule, the wide confidence interval and weak model fit indicate that the empirical relationship does not meaningfully support that proportional claim at the level of individual subjects. The amount of outcome variation accounted for by the predictor was low (R² = 0.23), meaning that approximately 23% of the variance in femoral head level differences was explained by innominate changes, while the remaining 77% was attributable to other factors, which may be things like biological variability, measurement error, or unrelated pelvic and lower-extremity mechanics. The slope estimate was statistically significant (p = 0.018), but the practical significance was limited by the weak explanatory strength of the model. A residuals-versus-fitted plot did not show patterns suggestive of significant departures from linear regression assumptions, indicating that these assumptions were reasonably met for the purposes of this analysis.
A z-score threshold of |z| > 2 was used as an outlier screening to flag values that fall noticeably outside the general pattern of the data. Outlier screening identified three subjects (2, 8, and 27) showing large deviations. Removal of these outliers resulted in a substantially reduced slope (β = 0.205; 95% CI: –0.21 to 0.62) and a much weaker model (R² = 0.04), suggesting that the apparent association in the full dataset was disproportionately influenced by extreme observations. Split-sample analyses illustrated additional variability: positive innominate changes produced a slope of 0.33 (R² = 0.09) and negative innominate changes yielded a slope of 0.64 (R² = 0.17). Both models demonstrated low explanatory power and substantial dispersion of data points, reflecting inconsistent relationships across subsets. Overall, across all analyses, the empirical patterns deviated substantially from the 5:2 proportionality expected under the Gonstead model.
Split-sample analyses illustrated additional variability:
- Positive innominate changes produced a slope of 0.33 (R² = 0.09).
- Negative innominate changes yielded a slope of 0.64 (R² = 0.17).
Both models demonstrated low explanatory power and substantial dispersion of data points, reflecting inconsistent relationships across subsets. Overall, for all the analyses, the patterns deviated substantially from the 5:2 proportion expected by the Gonstead theory, in relation to individual patient applications.
Table 1 summarizes the findings for 29 subjects, comparing the measured relative femur head heights with the calculated leg length inequality derived using the Gonstead method for assessing innominate bone misalignment in relation to leg-length differences.
Regression values for the results of the original full data set, for the data set with the outliers removed and for separate regressions for positive vs negative changes in innominate measures are shown in Table 2.
Overall, femoral head height changes were highly variable and only weakly related to innominate alignment differences. After outlier removal, the linear association largely dissipated, indicating that the proposed 5:2 proportionality rule was not consistently supported across the sample. Separate analyses for positive and negative innominate differences revealed nonsignificant trends for both subgroups.
Discussion
To place our findings in context, it is important to recognize the factors that may influence measurement accuracy in this study. Improper patient positioning, particularly pelvic rotation or translation, can distort radiographic images. Additionally, variations in body size, anatomical structure, and source-to-object or object-to-film/DR-cassette distances can introduce measurement differences that affect the calculated ratios of pelvic alignment and LLI. There is also a minute magnification factor that adds a very slight error in comparing the measured alignment to the actual alignment, which is very likely clinically insignificant.
Our methods for assessing these potential effects on the calculation of pelvic and FHL measurements have been used in previously published studies.36,48,49 Rotational distortion is reflected in the pelvic alignment measurement by the degree of deviation between the center of the pubic symphysis and the center of the sacrum at S2. A properly centered patient at the time of radiographic acquisition would demonstrate alignment of the pubic symphysis center with the S2 center along the y-axis.
An outlier screening z-score of 2 corresponds to roughly 2 standard deviations from the mean, far enough out in the tails that most observations shouldn’t fall there by chance in a reasonably shaped dataset. Using this cutoff does not “prove” an observation is an error, but it helps identify points that may have an outsized influence on the regression and deserve closer inspection. After removal of outliers, the range of S2-to–pubic center Y-axis net deviation between pre- and post-treatment images in the remaining sample of 26 patients was 0 to 6 mm. To contextualize the measured values in these 26 subjects, we calculated the potential influence of a 6 mm +Θy rotational malposition (the maximum observed in this sample) on the apparent change in LLI between pre- and post-treatment radiographs. This calculation used methods and parameters described in previous studies for estimating pelvic rotation on AP full-spine images,36,49 and was based on measurements from an average-sized adult male (1 of the authors, M.A.L.; 160 lbs, 5’10") using the same radiographic procedures applied in this study.
Based on those parameters, the maximum effect of ±Θy rotation–induced image distortion resulting from a 6 mm S2-to–pubic center Y-axis deviation on the AP full-spine image was determined to be approximately 2 mm of measured LLI. There were 14 subjects with post-treatment LLI value changes observed in our sample of 26 subjects, after the removal of outliers, which fall outside the range attributable solely to rotational image distortion for this example using an average size male. In other words, the changes in LLI seen from the pre- to post-treatment radiographic examinations in those 14 subjects are likely to be attributed to factors other than radiographic image distortion. We can also reasonably assume that these LLI changes were not from anatomical changes in LLI, given that there was no evidence in patient records of events that might cause such a change. Furthermore, these pelvis and LLI measurements using the Gonstead method have been previously shown to be stable and reliable on repeated radiographic examinations after one hour and after 18 days, without significant differences in LLI, sacral height and innominate measurements.33 Therefore, the changes in LLI that were over 2 mm from pre- to post-treatment radiographs were likely some kind of functional adaptations. The magnitude of LLI changes observed in this treatment sample (up to a maximum of 6 mm) appears small enough to be well compensated for and is unlikely to have substantial clinical significance.
Biological variability and the complexity of pelvic and lower extremity biomechanics also likely contribute to the lack of predictability of the relationship between pelvis and leg length measurements. Given these findings, relying on a linear ratio of leg length to pelvis alignment likely does not accurately reflect biomechanical presentations on radiographs.
Strengths and Limitations
Strengths of this study include the use of standardized full-spine radiographs, a single experienced examiner applying consistent and pre-validated Gonstead measurement methods, and it directly evaluates a widely taught clinical rule rather than assuming its validity. Evaluating changes within each subject also helps limit the impact of natural differences between individuals.
Limitations include the retrospective design, small sample size, and use of a single clinical site, which restricts generalizability. This study assessed only the linear aspect of the relationship; potential non-linear or threshold effects, such as changes seen only beyond a certain degree of misalignment, were not evaluated.
Because the study included a relatively small sample, its statistical power was limited, which means the analysis was less able to detect a true relationship even if it exists. As a result, the non-significant findings should be interpreted cautiously. The lack of strong evidence for the 5:2 rule does not necessarily prove the absence of a relationship but rather reflects the limits of a small sample size and wide data variability. Larger studies would be necessary to determine whether Gonstead’s 5:2 rule is truly absent or just too subtle to detect in this dataset. However, the clinical application of the Gonstead 5:2 rule is meant to be used on individual patients when misalignment of the pelvis occurs between innominate bones and when computing the measured versus the predicted anatomical LLI. Given the variability of the data dispersal in this study, it is unlikely that a specific ratio of this nature would be useful in individual patients, even if the overall linear regression exhibited a 5:2 ratio on average.
A key question regarding proper interpretation of the Gonstead 5:2 rule is whether it was intended to describe a general population-level tendency or whether it was meant to guide clinical decisions for individual patients when determining whether lift application is appropriate for correcting leg length inequality. If the rule was meant to reflect a broad tendency in the population, then the regression slope observed in this study (0.442) could be interpreted as consistent with a 5:2 rule, though the sample is small. However, the intended clinical purpose of the ratio has typically been its application to individual patients, and the considerable variability seen in these subjects suggests that the 5:2 rule does not provide a dependable basis for individual decision-making alone.
CONCLUSION
The regression slope (0.442) did not meaningfully align with the 5:2 ratio given the wide variation of data dispersion and inconsistent directional patterns across the dataset. Only 23% of the variance was accounted for by the model (R² = 0.23), indicating limited predictive strength. The 95% confidence interval for the full-sample slope was wide (0.12 to 0.76), further suggesting that the estimated effect was variable with a large range of possible relationships. Removal of outliers further reduced the slope (0.205; 95% CI: –0.21 to 0.62) and weakened the association, and subgroup regressions demonstrated slope estimates that varied substantially between positive and negative innominate changes. Therefore, these findings do not provide substantial support for the null hypothesis, and the data favor the alternative hypothesis that femoral head height differences are not reliably or proportionally predicted by innominate measurement asymmetry according to a 5:2 relationship.
AI Acknowledgment
ChatGPT (OpenAI) 2025 was used to support text editing, assisting in the computation of linear regression models and the creation of exploratory scatter plots using author-provided numerical data, formatting tables and producing Figure 1. All analyses and results were reviewed and confirmed by the authors.
The authors also acknowledge the assistance of docAnalyzer.ai, an AI-powered web application that was used after the manuscript was completed to evaluate the text and provide editorial suggestions for improvement prior to submission. The tool was employed solely for manuscript-level review (e.g., checking clarity, consistency, and adherence to journal style) and did not contribute to the study design, data collection, analysis, or interpretation.
Acknowledgement
We would like to acknowledge David Rowe D.C. for his assistance with patient records.